
Abstract
PURPOSE We wanted to analyze National Institutes of Health (NIH) awards to departments of family medicine.
METHODS We obtained the list of NIH awards to departments of family medicine in 2003, and collected additional information from the Internet regarding each principal investigator (PI), including whether he or she worked primarily in a core (central) organizational component within a family medicine department.
RESULTS One hundred forty-nine NIH awards were granted to 45 departments of family medicine, for a total of $60,085,000. Of 146 awards with a designated PI, approximately two thirds of awards (89, 61%) and awarded dollars ($39,850,000, 70%) went to PIs who were either not full-time family medicine faculty primarily working in family medicine departments, or they were not working in core family medicine organizational components. Few awards to physician PIs in these non-core areas were to family physicians (4 of 37, 11%), whereas most awards to physician PIs in core family medicine areas went to family physicians (40 of 45, 89%). In contrast, most K awards (research career programs) went to PIs in core areas (19 of 23, 83%), and most to family physicians (17 of 23, 74%). Nationally, only 17 R01 awards (research project, traditional) went to family physicians.
CONCLUSIONS Most NIH awards to family medicine departments went to PIs in noncore organizational components, where most physician PIs were not family physicians. Family medicine departments interested in increasing NIH funding may want to consider 4 models that appear to exist: individual faculty in core departmental components, K awards, core faculty also working in university-wide organizational components that provide research infrastructure, and integrating noncore administrative components into the department.
INTRODUCTION
During the past 3 decades, departments of family medicine have made substantial contributions within US medical schools, especially in the areas of clinical care and education. Even so, family medicine has yet to achieve parity with many other academic departments regarding research.1–6 Overall, medical research is funded by a wide variety of sources. National Institutes of Health (NIH) funding remains the major research yardstick for most medical schools as a result of its prestige, the large amount of funds awarded each year, and its relatively high indirect cost rate.7 Among family medicine departments, however, the role of NIH-funded research remains unclear. The NIH has not been a major source of family medicine research funding,1 and no single NIH institute specifically focuses on primary care or family medicine research areas.8 Nonetheless, NIH funding is highly sought after by most medical school deans and chairs of family medicine alike.
Currently, the major data source reporting NIH funding to family medicine departments is the yearly report, “NIH Extramural Awards to Medical School Departments,” which ranks all academic departments. Data in this report are minimal, however, reporting a rank list by dollar amount awarded to each department that receives funding, and including only school name, address, total dollar amount awarded to the department, and total number of grants awarded.
To learn more about NIH funding awarded to departments of family medicine, we undertook a study to analyze the 2003 annual report of “NIH Extramural Awards to Medical School Departments.”9 We also believed that a better understanding of recent NIH funding of family medicine departments could provide important information for all family medicine academic departments.
METHODS
We obtained from the NIH a publicly available list of all 127 individual awards to departments of family medicine in 2003. For each grant, data included the name, city, and state of the medical school; grant number; NIH funding institute; name of the principal investigator (PI); grant project title; and dollar amount of the award (which we rounded to the nearest thousanth dollar).
As a result of discussions with other family medicine researchers, we became aware that a small number of medical schools had a policy of reporting their research awards for family medicine departments under the NIH listing for Departments of Public Health and Preventive Medicine. As a result, we also obtained this list from the NIH. To determine which of these awards might more appropriately be classified with departments of family medicine, we reviewed all 501 grants and searched their respective medical school Internet sites to determine the faculty appointments for each PI listed. We identified 23 grants for which the PI had a faculty appointment in the department of family medicine. We then determined whether any of these PIs had their primary faculty appointment in either a Department of Preventive Medicine or a Department or School of Public Health. After identifying and excluding 1 such individual, we added the available data for the remaining 22 awards to our original list of 127 NIH awards.
Next, 2 of the authors (HKR and NDG) independently searched the Internet to obtain additional information for each PI from this revised list of 149 awards. For each PI, 3 searches were conducted: first on the Internet search engine Google; second on the home page of the PI’s medical school; and finally on the home page of their school’s family medicine department. Information for each PI obtained from these searches included their academic degrees and all faculty appointments, including academic rank and departments. The medical specialty was obtained for each physician PI from the American Board of Medical Specialties (ABMS), and family medicine board certification status was verified through the American Board of Family Medicine (ABFM).
In addition, for each PI, we made an attempt to identify the organizational structure or component (eg, section, division, unit, center, or area), where they appeared to primarily work, using the Web sites, work address, e-mail address, etc. We dichotomized PIs by whether they were working in a core (or central) organizational component within a family medicine department. PIs were deemed to be working in a core family medicine component if they (1) were full-time faculty working primarily at the medical school, (2) had their primary academic appointment in a department of family medicine, and (3) worked primarily within an organizational component within a department of family medicine that was part of the central focus of family medicine departments at most medical schools (eg, educational, clinical, and family medicine research areas, regardless of whether they were organized into formal sections or divisions).
PIs were considered to be in noncore family medicine components if they (1) were not primarily working at the medical school; (2) were not on the full-time faculty; (3) did not have their primary academic appointment in a family medicine department; (4) primarily worked in an organizational component or area of the university that was administratively not within the department of family medicine; or (5) worked primarily within a family medicine department, but in an organizational component (either formal or not) that (a) was not a central component of family medicine and not administratively located within the family medicine department at most other medical schools, (b) included multiple individuals, and (c) served as a resource for the larger medical school or university.
All data were entered into an Excel spreadsheet and analyzed descriptively. Because we analyzed the entire data set of NIH awards to family medicine departments in 2003, inferential statistics were not needed.
RESULTS
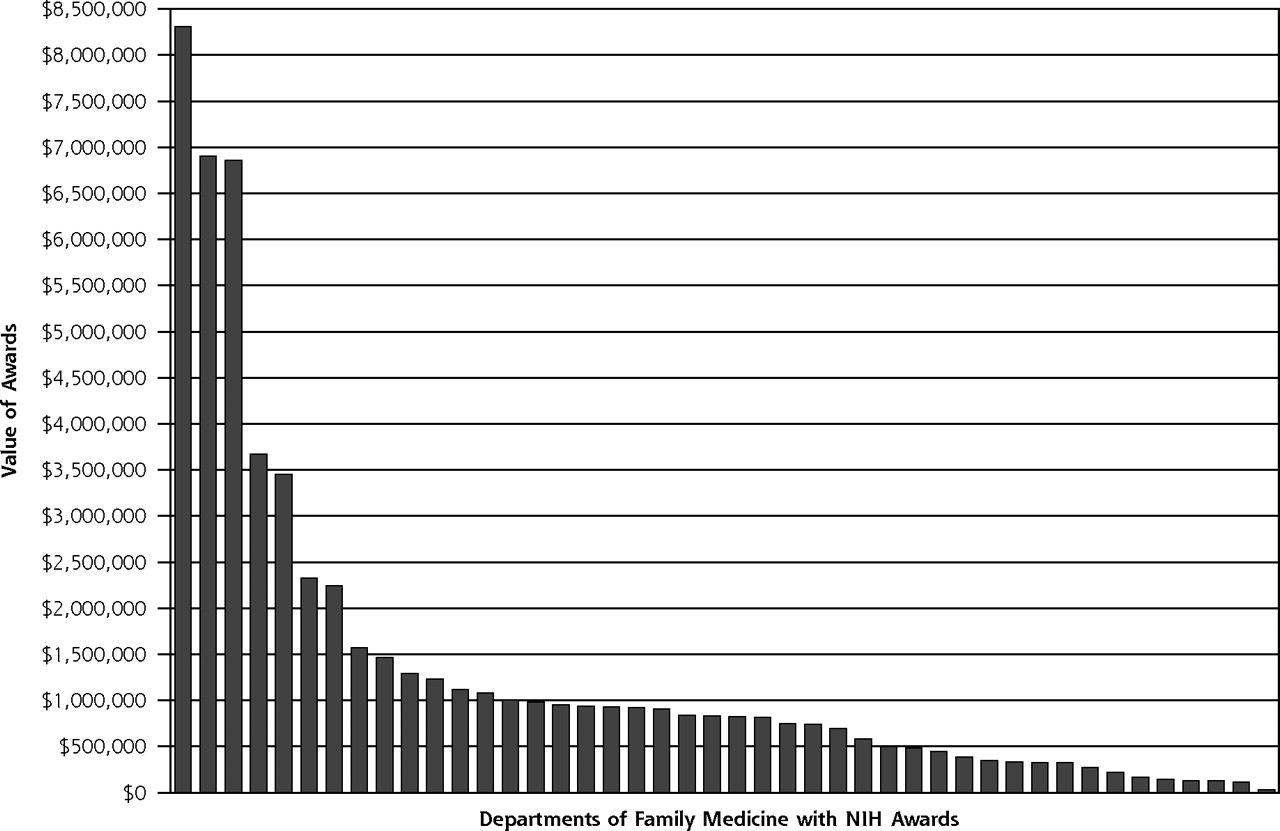
In 2003, there were 149 NIH grants awarded to 45 of the 113 (40%) departments of family medicine in US medical schools, for a total of $60,085,000. The 7 medical schools with the largest amount of NIH funding in family medicine were awarded almost one half of all grants (65 of 149, 44%), and 56% of all awarded dollars ($33,771,000) (Figure 1⇓).
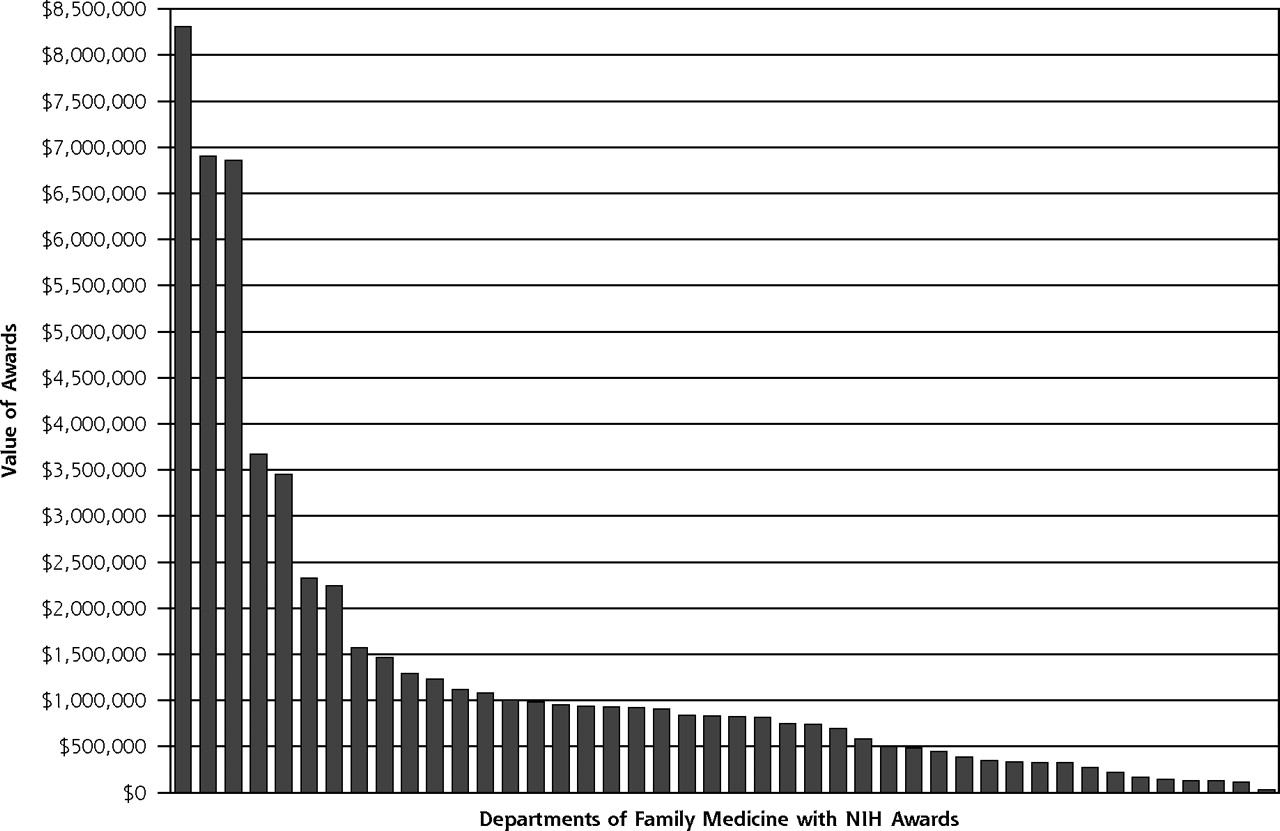
Value of National Institutes of Health (NIH) awards to departments of family medicine, by department, 2003.
Overall, 8 NIH institutes were responsible for providing 82% of all awards (122) and 75% of all awarded dollars ($45,126,000); the National Cancer Institute (NCI) was the largest source of grant funding (Table 1⇓). Seventy-two percent of all awards were for R (research project) awards, and 15% were for K (research career programs) awards (Table 2⇓); overall R01 awards (research project, traditional) were the most common specific type of award, representing 44% of all awards (66).
Number of National Institutes of Health (NIH) Awards and Value of Awards to Departments of Family Medicine, by NIH Institute, 2003
Number of National Institutes of Health Awards and Value of Awards to Departments of Family Medicine, by Grant Type, 2003
Of the 149 NIH awards, 3 which were awarded as part of the Women’s Health Initiative (total funding of $2,978,000) did not identify a PI, and were not considered in any further analyses. The remaining 146 grants ($57,107,000) were awarded to 109 different PIs. Of these awards, almost one half (63, 43%) went to PIs with nonmedical doctoral degrees. Of awards to PIs with a medical degree, more than two thirds (58 of 82, 71%) also had another advanced degree (Table 3⇓). Of awards to physician PIs, however, only about one half (44 of 82, 54%) went to family physicians (Table 4⇓).
Number of National Institutes of Health Awards and Value of Awards to Departments of Family Medicine, by Principal Investigator Degree(s), 2003
Number of National Institute of Health Awards to Departments of Family Medicine, by Physician Principal Investigator Specialty, 2003
Dichotomizing all 146 awards into whether the PI appeared to be working primarily in a core organizational component of a family medicine department showed that 57 awards (39%) went to PIs in core areas (Figure 2⇓), accounting for 30% of awarded dollars ($17,257,000). These 57 awards included 13 awards to PIs who also spent substantial time working in a university component that was outside the family medicine department (eg, cancer center, health services research center). Eighty-nine awards went to PIs in noncore organizational components, including 15 to PIs who were either not primarily working at the university or were not on the full-time faculty, and 37 to PIs whose primary academic appointment was not in family medicine or who were primarily working in an organizational component not located within the department (eg, a university cancer center, health services research center, dean’s office). In addition, 37 awards went to PIs who were working primarily within a department of family medicine, but they were classified as being noncore because the area in which they worked was not a central or typical component of most family medicine departments, included multiple people, and served the university-wide community (eg, divisions, units, or centers devoted entirely to nutrition, infection, global health, human sexuality, epidemiology, biostatistics, health services research, or a master in public health program).
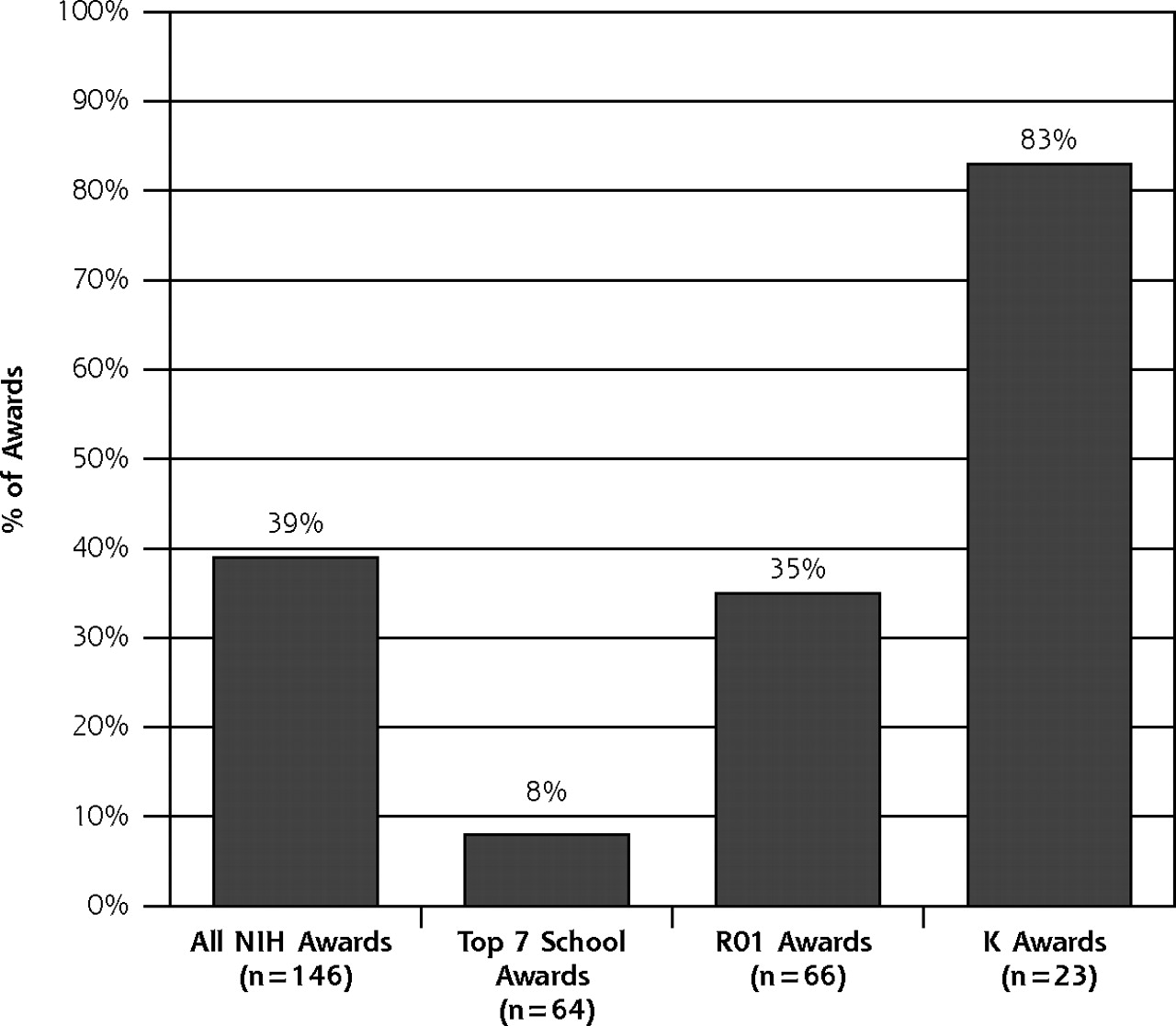
Percentage of National Institutes of Health (NIH) awards to principal investigators in core organizational components of departments of family medicine, 2003.
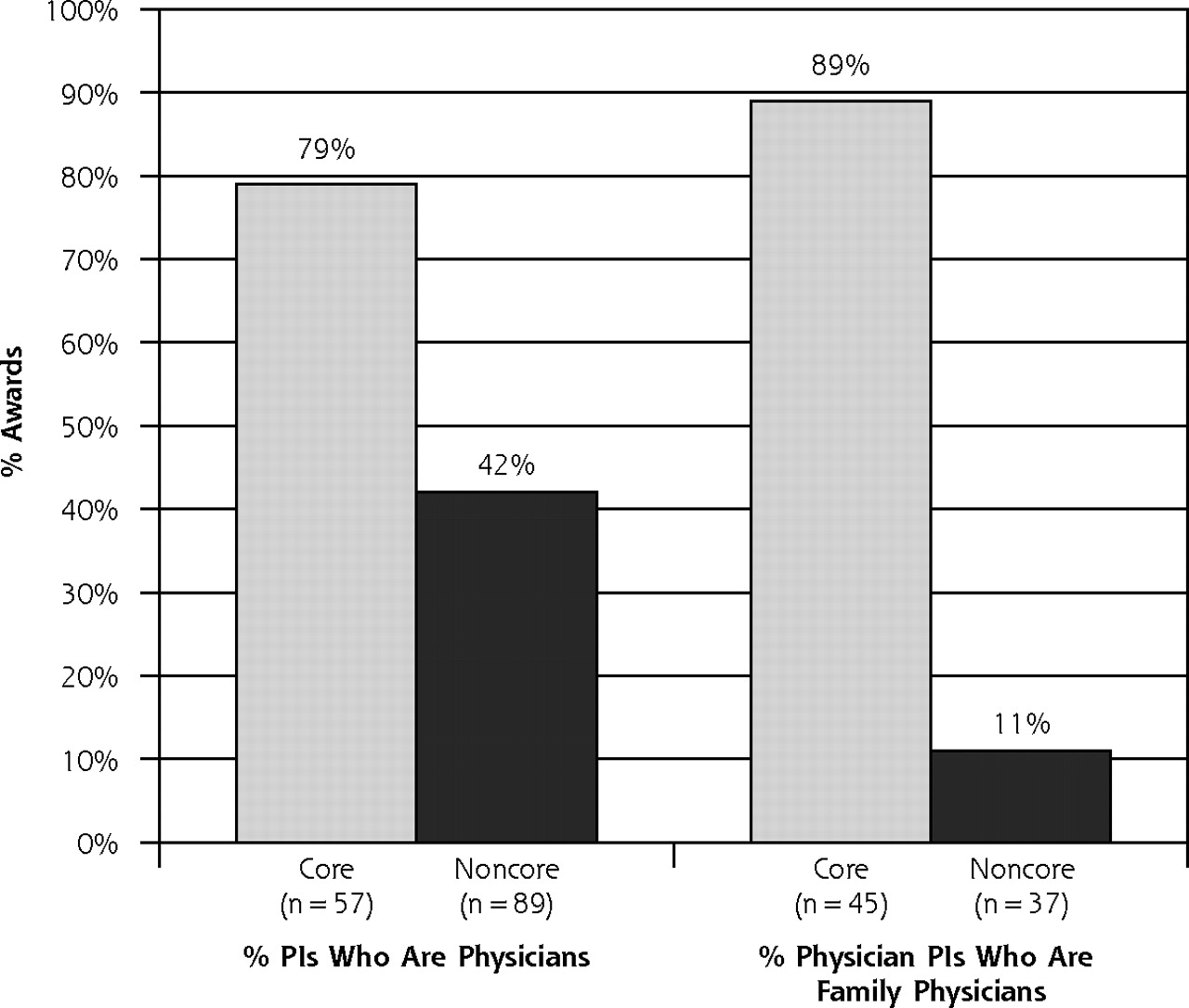
The percentage of PIs in core areas who were physicians was almost twice as high as those in noncore areas (79% vs 42%; Figure 3⇓). Furthermore, of awards to physician PIs, the great majority working in core areas were family physicians (40 of 45, 89%), whereas very few awards to physician PIs in noncore areas went to family physicians (4 of 37, 11%).
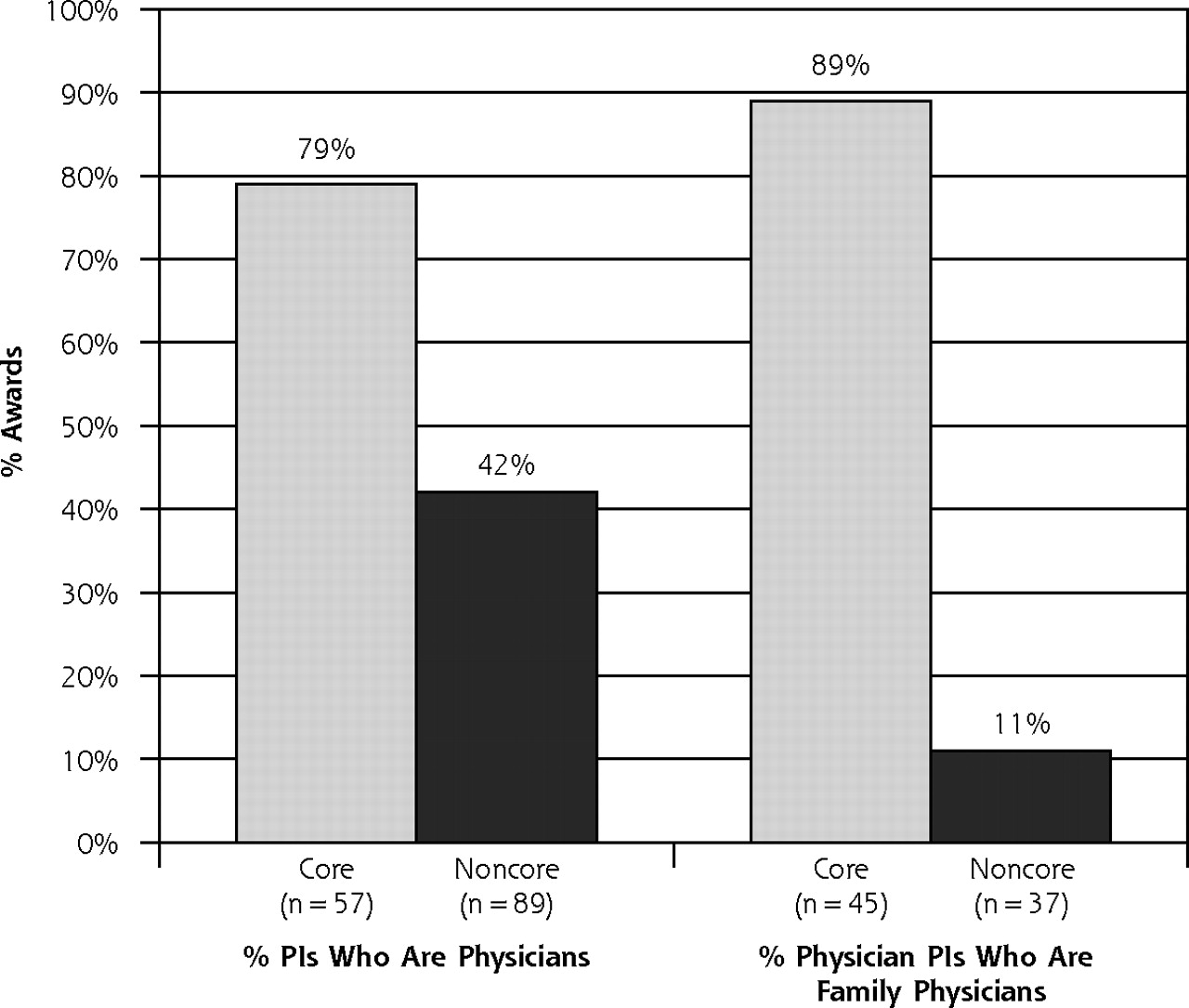
Percentage of National Institutes of Health (NIH) awards to principal investigators (PIs) who are physicians, and percentage of NIH awards to physician PIs who are family physicians, by core and noncore organizational components of departments of family medicine, 2003.
Among the 7 departments with the largest amount of NIH funding, these trends were even more pronounced. Almost all of these grants went to PIs who were in noncore family medicine administrative components (59 of 64, 92%; Figure 2⇑); and only 17% of awards to physician PIs went to family physicians (6 of 35).
Looking specifically at R01 grants, which represented 57% of all dollars awarded ($34,001,000), the pattern was similar to that for all NIH awards. PIs were physicians in approximately one half of these awards (34 of 66, 52%), and only one half of these were family physicians (17 of 34, 50%). In almost two thirds of R01 awards, PIs were working in noncore components (Figure 2⇑). Overall, most R01 awards to PIs in core areas were to physicians (18 of 23, 78%), compared with 16 of 43 (37%) awards to physician PIs in noncore areas. Furthermore, almost all awards to physician PIs in core components were to family physicians (16 of 18, 89%), whereas only 1 in a noncore area went to a family physician (1 of 16, 6%).
In contrast, the pattern regarding K awards was reversed, with most K awards going to PIs in core areas (Figure 2⇑). Most of these career awards (18 of 23, 78%) went to physicians, with 17 of these to family physicians (94%). Overall, the 23 K awards were granted to 16 different medical schools, 12 of which (75%) also received another NIH award; 9 of these included at least 1 R01 grant. For the 5 departments with more than 1 K award, all had at least 1 other NIH award, which for 4 included an R01 grant.
DISCUSSION
Despite its successful 35-year history, the discipline of family medicine continues to struggle with its research productivity.1–3,5 This study analyzed NIH research awards to departments of family medicine in 2003. Almost one half of all awards went to nonphysicians with doctoral degrees, representing a critically important resource for family medicine research. Of physician PIs, however, only one half of all grants went to family physicians, and nationally, only 17 R01 awards and 17 K awards went to family physicians—reinforcing the critical importance of increasing the research capacity in family medicine.1,4,6 This study also showed that the great majority of NIH funding to family medicine departments went to PIs who primarily work in noncore areas. That few physician PIs in noncore areas were family physicians (11%, compared with 89% in core areas) reinforces our claim that these noncore components are not a central part of most family medicine departments.
The outcomes of this analysis provide 4 different patterns that could serve as useful models for family medicine departments. First, family medicine faculty in core areas can develop their own focus of research and obtain NIH funding. Second, junior investigators working in core family medicine areas can obtain K awards; although this career development mechanism represents an important model for increasing research capacity, the need for mentors will often require that departments have other NIH-funded researchers. A third model, about which little has been written, is for family medicine faculty to spend substantial amounts of time in noncore university-wide areas that can provide important research infrastructures (eg, university-based health services research center) while also spending considerable time working in their own department. These interdisciplinary centers represent an important, though potentially underutilized, opportunity for family medicine faculty without requiring the development of an extensive research infrastructure within the department. Finally, the most common current model is for family medicine departments to incorporate faculty or university-wide components not usually a part of family medicine departments. This option appears limited in most universities and is dependent on taking advantage of unique institutional opportunities for restructuring.
This study has 3 significant limitations. Most important, it analyzed NIH grants from only 1 year, and the results may therefore not be generalizable to other time periods. Second, the Internet, which we used to obtain information regarding PIs, might not always be accurate or current, and the primary location of the PI within an institution is not always clearly defined. Finally, our definitions of what constitutes core and noncore family medicine components might not be universally accepted, although we believe that our methods resulted in a clear designation in almost all instances.
This study raises issues that are important to the future of family medicine research and to academic departments of family medicine.8 Obviously, the use of NIH funding as the predominate metric for medical school research status is of serious concern, as a considerable amount of family medicine research is funded through other equally important sources, including other federal agencies and foundations. Furthermore, although this study increases our understanding of NIH funding in departments of family medicine, the overall role of NIH funding in family medicine research remains unclear. Whereas the NIH primarily focuses on basic science and subspecialty research, the new NIH Roadmap includes areas highly relevant to family medicine research. In addition, many NIH grant titles from this analysis appeared especially suited to family medicine (eg, improving colorectal cancer screening in primary care, and adherence to depression treatments among the elderly), and family medicine has the potential to make unique and important contributions to many NIH research priorities.8,10
Acknowledgments
The authors would like to acknowledge the helpful comments of Paul C. Brucker, MD, and James J. Diamond, PhD, on earlier drafts of this manuscript.
Footnotes
-
Conflicts of interest: none reported
-
Funding support: This study was supported in part through a grant for Academic Administrative Units in Family Medicine, Bureau of Health Professions, Health Resources Services Administration, Department of Health and Human Services, grant #D54HP00178.
- Received for publication September 14, 2005.
- Revision received December 28, 2005.
- Accepted for publication January 16, 2006.
- © 2006 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Pathways to Physician Scientist Careers in Family Medicine
- BUILDING RESEARCH & SCHOLARSHIP CAPACITY IN DEPARTMENTS OF FAMILY MEDICINE: A NEW JOINT ADFM-NAPCRG INITIATIVE
- Family Medicine in the Research Revolution
- THE CHALLENGE TO BUILD RESEARCH CAPACITY IN FAMILY MEDICINE: IS OUR DISCIPLINE READY?
- Off the Roadmap? Family Medicine's Grant Funding and Committee Representation at NIH
- How Can Practice-based Research Contribute to the Elimination of Health Disparities?
- In This Issue: Capacity for Caring and Generating New Knowledge