
- Social responsibility
- Canada
- medical schools
- public health
- rural population
- rural health services
- workforce
- health planning
- medical education
INTRODUCTION
I am delighted to have been asked to provide a commentary to follow the excellent case study by Berg and Norris1 on integrating workforce planning, medical school expansion, medical school admissions, curriculum, and research at the University of Washington and in the WWAMI (Washington, Wyoming, Alaska, Montana, and Idaho) regional medical education program. The Association of American Medical Colleges in their 2005 report Achieving Accountability (http://www.aamc.org/publications) outlines 2 levels or kinds of accountability.2 Level I accountability refers to institutional requirements, for example, legal requirements, financial audits, and accreditation. Level II accountability refers to institutional choices, that is, how an individual academic medical center carries out its mission. The Washington/WWAMI case study fits more closely with the latter than with the former, but fits most closely with the vision for social accountability developed by the Canadian medical schools.3
PHYSICIAN WORKFORCE PLANNING
Achieving self-sufficiency of physician supply is one of the biggest social accountability challenges facing medical schools, governments, and other stakeholders. The University of Washington study found that the 5 WWAMI states are at the bottom of the states in number of medical school and residency slots per capita, import most of their physicians, and have a shortage of rural physicians.1 The University of Washington/WWAMI program has a mission to train health professionals for its region and is basing medical school expansion, admissions, curriculum, and research on workforce analysis.
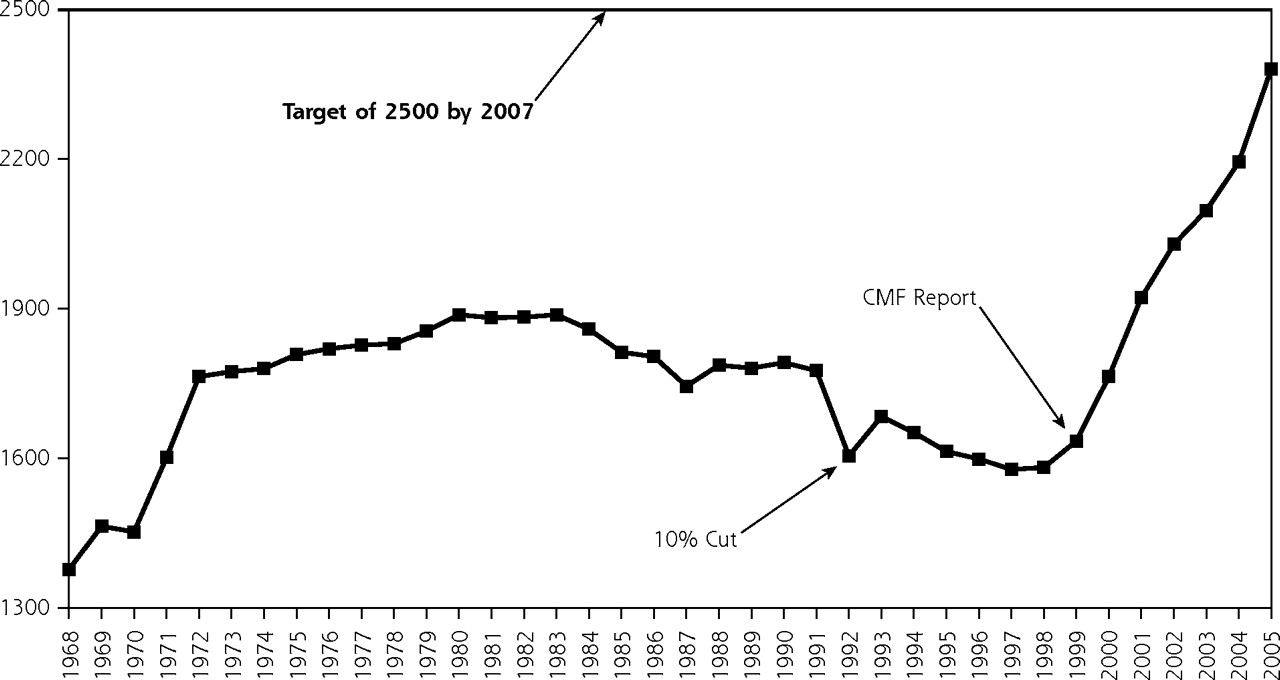
Canada, like the United States, has developed a pronounced shortage and maldistribution of physicians and has relied on a substantial importation of international medical graduates, who currently make up 22.7% of the Canadian medical workforce, in an attempt to meet the growing needs of the population.4 This is a cautionary tale of mistaken workforce planning. A commissioned report published in 1991, Toward Integrated Medical Resource Policies for Canada, projected an oversupply of physicians in the coming decade.5 Based in part on this projection, the government offices that controlled provincial medical student enrollment numbers cut back medical school enrollment by 10% for the nation. The subsequent reduction in physician numbers turned out to be an enormous mistake: the predicted oversupply turned into a severe shortage in the decade after the report as the health care system and patient care needs evolved. Medical schools have now responded to this societal need (with increased government funding) by increasing enrollment (Figure 1⇓).

First-year enrollment in medical schools in Canada, 1968 to 2005.
Source: Canadian Medical Education Statistics, Vol 28. Association of Faculties of Medicine of Canada, 2006.
CMF = CMF Report: Canadian Medical Forum Task Force on Physician Supply in Canada (Report 1999). Available at http://cua.org/socioeconomics/physician_supply_2000.pdf. Accessed 20 August 2006.
Notes: As geographic background, Canada has an area of 3.9 million square miles (making it larger than the United States) but has only 32 million people and 17 medical schools.
The biggest expansion is taking place at the medical school that is closest to the University of Washington, the University of British Columbia’s medical school, which has its main campus in Vancouver. This school is increasing enrollment from an entering class size of 128 in 2003 to one of 224 in 2005.6 This expansion involved establishing satellite campuses in Prince George (the Northern Medical Program) and Victoria (the Island Medical Program) with a distributed rural and regional community-based educational model building on the experience of the WWAMI program.
Canada has also established an innovative new Northern Ontario School of Medicine (NOSM) with a class of 56 students who started September 2005.7 Its 2 main campuses in Thunder Bay and Sudbury are 1,000 km apart, and the learning will take place in communities throughout Northern Ontario with a very distributed educational model.
Despite the large increases in medical school enrollment currently taking place across Canada, it will be at least a decade before physician human resources recover because of the length of time from entry into medical school to entry into practice (and compounding factors, including an aging population that will require more, not fewer, physicians). This experience illustrates how incredibly difficult it is to plan physician workforce needs. Changes in health technology, physician practice patterns, community needs, and funding for health care are all difficult to assess and act on now, let alone to use as the basis for recommendations for the future. In this regard, governments and health organizations and the Association of Faculties of Medicine of Canada have partnered in Task Force I and II to develop a new physician human resource strategy for Canada and published a major analysis in 2005 and recommendations in 2006.4,8
Where and how the new physicians will practice is vitally important, and much of the expansion of medical schools is rural and regionally based. In Canada, as in the United States, the physician shortage is worse in rural communities, especially in frontier regions, such as the provinces of Newfoundland and Labrador, New Brunswick, and Saskatchewan, and the 3 northern territories.4,9 Also as in the United States, the research on medical education shows that both rural background and rural medical education are important factors that contribute to the recruitment and retention of rural physicians.10–13 Similarly, mirroring the situation in the United States, rural residents are underrepresented in Canadian medical schools, making up 10.8% of medical students but fully 22.4% of the population.14,15 With 30% to 40% of its students from rural areas, Memorial University of Newfoundland (MUN) is the exception.
Similar to, though smaller than, the University of Washington/WWAMI program, MUN (http://www.med.mun.ca) serves a very rural and regional population. The province of Newfoundland and Labrador has a population of 512,000 and an area of 156,649 square miles, with geography and climate similar to those of Alaska. Like the WWAMI program, the MUN medical education program is very decentralized, involving both undergraduate and postgraduate clinical educational placements throughout Newfoundland and Labrador, particularly in family medicine.16 The postgraduate family medicine residency training program can include 8 months or more in Labrador in the NorFam (Northern Family Medicine Education) program, which is one of our examples of building “the pipeline to practice”—a WWAMI term.17 Some 17.2% of medical doctors graduating from MUN practice in rural areas, compared with 11% of those graduating from all Canadian medical schools.18 Fully 46% of graduates of the MUN family medicine residency training program practice in rural areas, compared with 20.9% of those from all Canadian family medicine programs.18 And whereas 41.2% of family physicians who do their family medicine residency training in Newfoundland and Labrador practice in rural communities, only 13.4% of graduates of all of Canada’s family medicine residency training programs do so.19
SOCIAL ACCOUNTABILITY
The mission for MUN medical school, developed many years before the social accountability vision for Canadian medical schools, is “to enhance the health of the people of Newfoundland and Labrador by educating physicians and health scientists; by conducting research in clinical and basic medical sciences and applied health sciences and by promoting the skills and attitudes of lifelong learning.” Social accountability is the fabric that binds medical schools and their communities and regions together.
In 2001, Health Canada published Social Accountability: A Vision for Canadian Medical Schools, a report developed by a task force of multiple stakeholders, including strong involvement of Canada’s medical schools.3 This social accountability vision begins with the 1995 World Health Organization (WHO) definition of social accountability of medical schools as “the obligation to direct their education, research and service of activities towards addressing the priority health concerns of the community, region and/or nation that they have a mandate to serve. The priority health concerns are to be identified jointly by governments, health care organizations, health professionals and public.”20 By identifying and responding to the needs of the community, Canadian medical schools along with their partners have a major role to play in influencing the changes in the health care system that are necessary to ensure an effective, efficient, accessible, equitable, and sustainable system in the 21st century. Social accountability is essential in shaping the future of medical education, research, and health care in response to present and future societal needs.
The social accountability vision for Canadian medical schools sees an important leadership role for medical schools in key areas:
-
The development of a clear and shared vision of the health care system and of the health care providers (both individuals and institutions) of the 21st century, a vision that will have to be clearly articulated and constantly revised to respond to changing needs
-
The optimal preparation of future practitioners to respond to population needs
-
The establishment and promotion of innovative practice patterns to better meet individual and community needs
-
The reinforcement of partnerships with other stakeholders, including academic health centers, governments, communities, and other relevant professional and lay organizations
-
Advocacy for the services and resources needed for optimal patient care
-
The definition and clarification of the concept of social accountability, and the dissemination of methods for measuring responsiveness to societal needs
-
The inclusion of the concept of social accountability in the accreditation process of medical schools and other health institutions
Canada’s medical schools have established several national social accountability projects and activities. These have several important, broad defining features: input/participation of broadly based groups of stakeholders (governments, universities, the public/communities, professions, health administrators, students, and health policy makers, represented in the Partnership Pentagram shown in Figure 2⇓); identification of key Canadian priorities; buy-in and participation from all 17 medical schools; and development of sustainable multiyear funding.
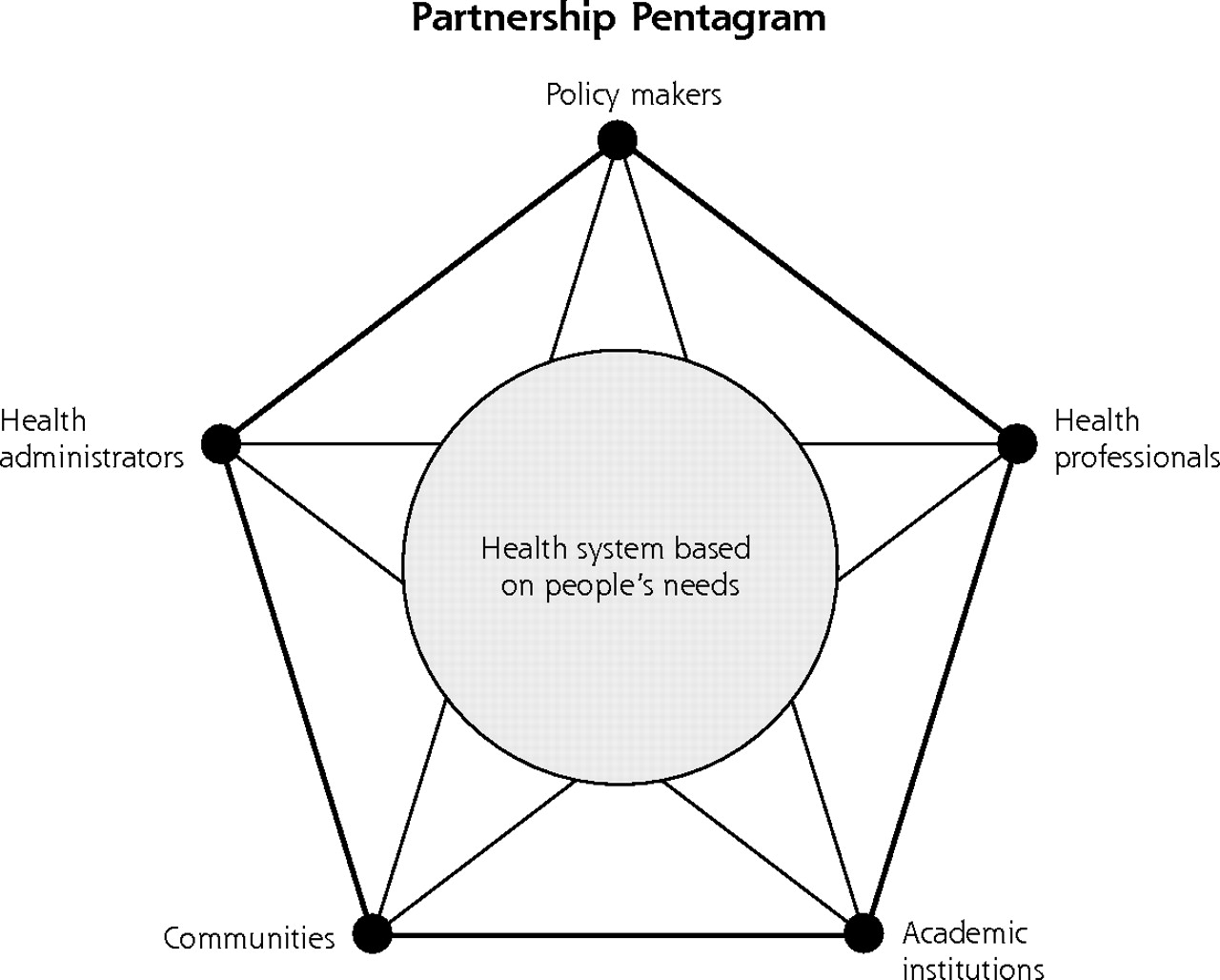
A partnership pentagram showing the 5 broad groups of stakeholders influencing the social accountability projects of Canadian medical schools.
Note: Adapted from: World Health Organization. Towards Unity for Health: Challenges and opportunities for partnership in health development. Geneva: WHO; 2000. Available at: http://www.who.int/entity/hrh/documents/en/TUFH_challenges.pdf. Accessed 7 August 2006. See also 2004 Association of Canadian Medical Colleges (ACMC) Social Accountabilities Poster. Presented at the 2004 ACMC-CAME (Canadian Association for Medical Education) annual meeting, Halifax, Nova Scotia. Available at: http://www.afmc.ca/pages/articles_social_accountability.html. Accessed 7 August 2006.
Two examples of the national social accountability projects of Canadian medical schools are the enhancement of aboriginal health and the strengthening of public health nationally. Both of these projects arose in response to key identified Canadian needs. The former project is driven by the poor health status of Canada’s aboriginal people and the lack of health care professionals, particularly aboriginal physicians, for that community. The latter project was initiated by a public health threat. The epidemic of severe acute respiratory syndrome (SARS) made it clear that Canada needed to increase the capacity, strength, and efficiency of its public health system, which would clearly require the involvement and participation of Canada’s medical schools from coast to coast. More information on these projects is available online (http://www.afmc.ca/pages/articles_social_accountability.html).
Canadian medical schools not only partake in social accountability projects at the national level, but they also have many social accountability roles and projects related to the general and specific needs of their regions. This also certainly seems to be in evidence in the University of Washington/WWAMI case study.
In conclusion, all medical schools contribute to the needs of society by educating tomorrow’s doctors and doing research that makes a difference. The heart of the concept of social accountability/responsibility is that by directing medical school education, research, and service activities toward addressing the priority health concerns of their community/region, their nation, or both, medical schools can make the greatest contribution to the health and well-being of humanity.
Footnotes
-
Conflicts of interest: none reported
- Received for publication January 12, 2006.
- Accepted for publication February 27, 2006.
- © 2006 Annals of Family Medicine, Inc.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Responsabilite sociale: Perspective du Nunavut
- Social accountability: Nunavut perspective
- Determinants of first practice location: Among Manitoba medical graduates
- On TRACK: Challenges and Insights
- Shaping the Future of Academic Health Centers: The Potential Contributions of Departments of Family Medicine