
Article Figures & Data
Figures
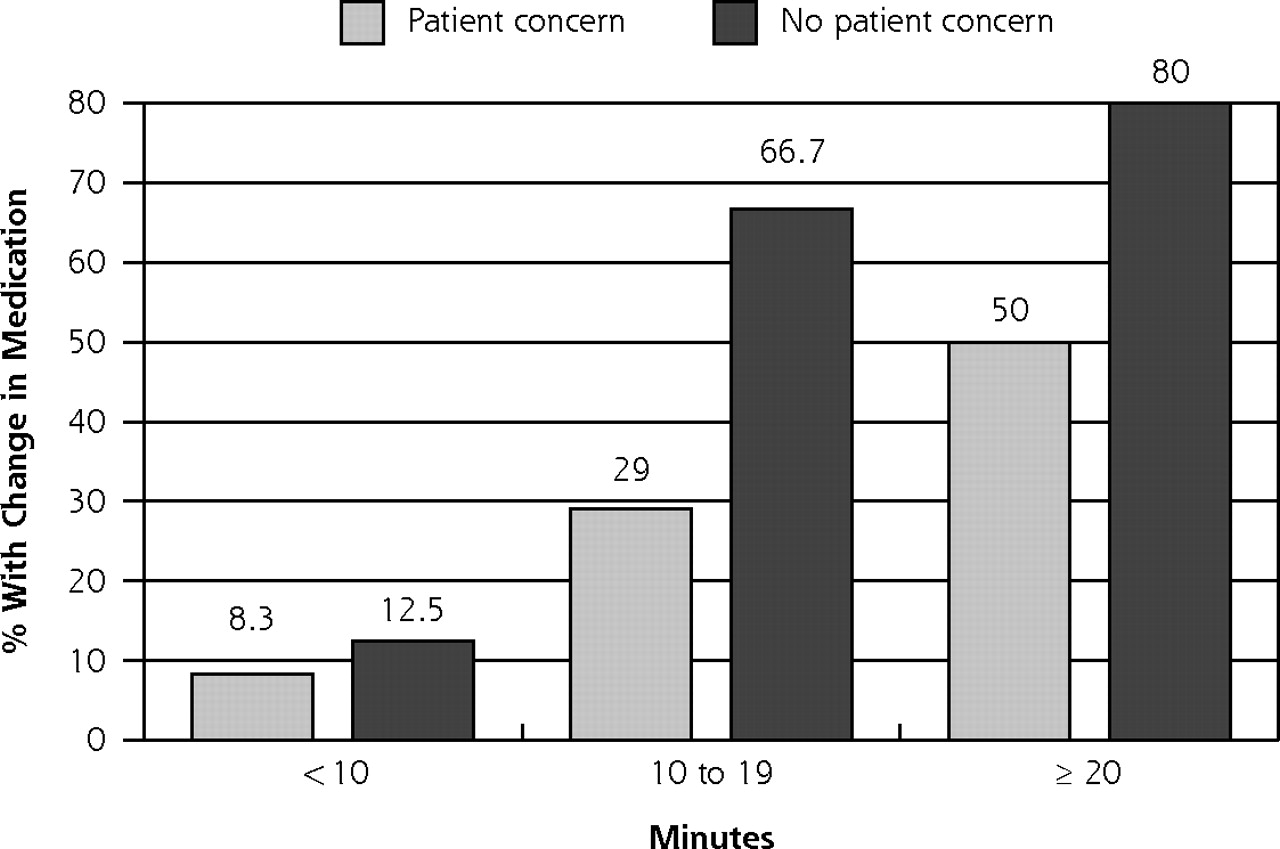
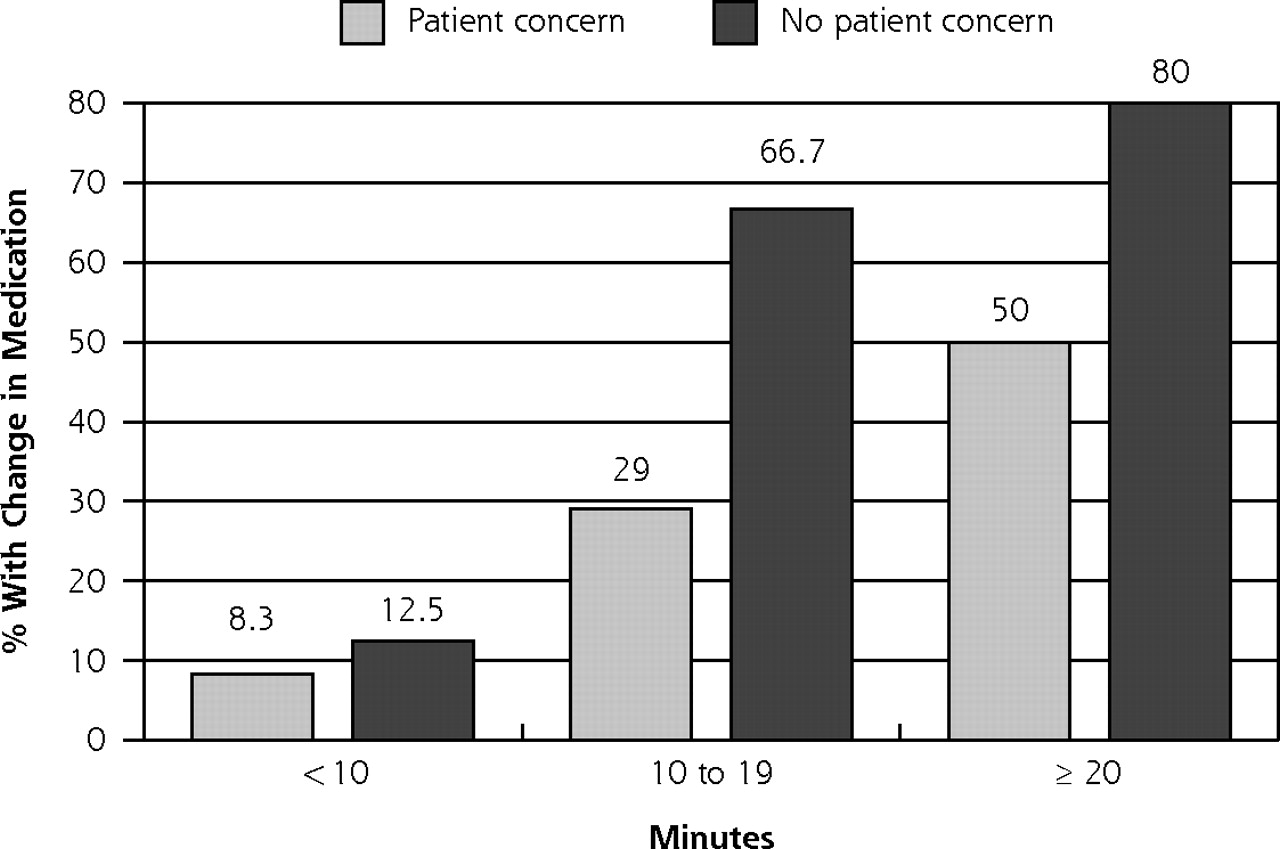
- Figure 1.
Percentage of patients with a change in medication, by encounter length and presence of patient concerns.
Note: χ2 across Patient concern: 7.26 (P =.03); χ2 across No patient concern: 6.93 (P =.03).
Tables
Characteristic Mean (SD) or % Hemoglobin A1c=glycosylated hemoglobin. Age, years 59.0 (13.3) Female, % 51.3 Hispanic, % 59.2 Hemoglobin A1c level >7.0% 55.4, >8.0% 34.5 Length of encounter, minutes 17.0 (8.4) Number of patient concerns 2.0 (1.9) Encounters with a change in hypoglycemic medication, % All 26.7 With hemoglobin A1c level >7% 35.6 With hemoglobin A1c level >8% 42.9 With hemoglobin A1c level >9% 46.4 Days to next scheduled appointment 60.9 (43.2) - Table 2.
Changes in Medication by Patient and Encounter Characteristics if Hemoglobin A1c Value Was Greater Than 7% (n = 98)
Characteristic Change in Medication Mean (SD) or % No Change in Medication Mean (SD) or % P Value Hemoglobin A1c=glycosylated hemoglobin. Patient characteristics Age, years 57.5 (13.2) 56.7 (13.5) .76 Female, % 54.9 50.0 .55 Hispanic, % 60.8 59.6 .88 Number of comorbidities 4.8 (2.2) 4.3 (1.9) .22 Hemoglobin A1c, % 8.6 (2.1) 7.3 (1.7) <.001 Previous hemoglobin A1c level worse, % 51.5 50.9 .95 Number of long-term medications 7.09 (3.14) 5.51 (2.92) .02 Encounter characteristics Number of patient concerns 1.5 (1.3) 2.4 (2.1) .04 Number of topics discussed by physician 13.4 (4.49) 11.3 (5.05) .05 Length of encounter, minutes 19.4 (7.2) 15.4 (7.8) .02 Number of days since last measured hemoglobin A1c 70.8 (94.8) 110.2 (170.5) .07 Percentage of encounter devoted to: Discussing nutrition 5.23 (6.25) 2.91 (4.76) .07 Discussing exercise 1.50 (2.24) 1.71 (3.20) .77 Discussing medication compliance 7.47 (6.26) 7.79 (6.09) .83 Percentage of encounter time until: Evaluation/feedback of test results 48 (0.29) 0.62 (0.80) .44 Discussion of planning treatment 74 (0.28) 0.80 (0.43) .57 If A1c >7% (n=98) If A1c >8% (n=61) Predictor Odds Ratio 95% CI Odds Ratio 95% CI CI=confidence interval; hemoglobin A1c=glycosylated hemoglobin. Number of patient concerns 0.51 0.40–0.65 0.52 0.33–0.83 Number of clinician topics 1.02 0.93–1.12 1.00 0.90–1.10 Length of encounter in minutes 1.08 1.00–1.17 1.00 0.93–1.09 Most recent hemoglobin A1c value 1.11 0.83–1.48 1.15 0.77–1.74 Number of long-term medications 1.10 0.93–1.31 1.03 0.86–1.24 Days since last hemoglobin A1c 1.00 0.99–1.00 1.00 1.00–1.00
The Article in Brief
Competing Demands or Clinical Inertia: The Case of Elevated Glycosylated Hemoglobin
Michael L. Parchman, MD, MPH , and colleagues
Background Medication plays a key role in controlling blood sugars in diabetes patients. This study examines two possible reasons why primary care doctors might not change the medication of diabetes patients whose blood sugar is not well controlled: "clinical inertia" (recognizing but not acting on a medical problem), and "competing demands" (the need to address several medical problems, patient concerns, and preventive health measures in the limited time of a doctor visit).
What This Study Found Primary care doctors address and prioritize many medical issues during patient visits. As the number of medical issues raised by a patient with high blood sugar goes up, the likelihood of a change in their medication goes down. Compared with other doctor visits, those in which diabetes medication is changed are longer, and the patient has fewer medical concerns but a higher blood sugar. Doctors spend the same amount of time discussing self-care measures with patients who have high blood sugars, regardless of whether they change the medication.
Implications
- The ability to treat multiple conditions is a strength of primary care. Because multiple conditions present competing demands, the patient and doctor must set goals and priorities during their visits.
- Studies using the term "clinical inertia" usually focus only on diabetes care and not the patients� other health care needs. As a result, approaches to diabetes care based on clinical inertia are likely to be ineffective.
- The concept of competing demands better describes the diabetes patient�s primary care visit than the concept of clinical inertia.




{kind=link}
Jump to section
Related Articles
Cited By...
- Does Clinical Decision Support Increase Appropriate Medication Prescribing for Cardiovascular Risk Reduction?
- Patients With Type 2 Diabetes Are Willing to Do More to Overcome Therapeutic Inertia: Results From a Double-Blind Survey
- Turning Points as Opportunities to Partner with Patients Living with type 2 Diabetes or Prediabetes
- Supporting care for suboptimally controlled type 2 diabetes mellitus in general practice with a clinical decision support system: a mixed methods pilot cluster randomised trial
- A Behavioral Perspective of Therapeutic Inertia: A Look at the Transition to Insulin Therapy
- Overview of Therapeutic Inertia in Diabetes: Prevalence, Causes, and Consequences
- Therapeutic Inertia in People With Type 2 Diabetes in Primary Care: A Challenge That Just Wont Go Away
- Key factors for overcoming psychological insulin resistance: an examination of patient perspectives through content analysis
- GP-OSMOTIC trial protocol: an individually randomised controlled trial to determine the effect of retrospective continuous glucose monitoring (r-CGM) on HbA1c in adults with type 2 diabetes in general practice
- Outcomes For High-Needs Patients: Practices With A Higher Proportion Of These Patients Have An Edge
- Examining the effects of comorbidities on disease-modifying therapy use in multiple sclerosis
- Provider beliefs about diabetes treatment have little impact on glycemic control of their patients with diabetes
- Perspectives in Primary Care: Implementing Patient-Centered Care Coordination for Individuals with Multiple Chronic Medical Conditions
- Potential Antidepressant Overtreatment Associated with Office Use of Brief Depression Symptom Measures
- "My approach to this job is ... one person at a time": Perceived discordance between population-level quality targets and patient-centred care
- Variations in Coronary Artery Disease Secondary Prevention Prescriptions Among Outpatient Cardiology Practices: Insights From the NCDR (National Cardiovascular Data Registry)
- Improved Outcomes in Diabetes Care for Rural African Americans
- Perceptions of Usability and Design for Prefilled Insulin Delivery Devices for Patients With Type 2 Diabetes
- Implementing and Evaluating Electronic Standing Orders in Primary Care Practice: A PPRNet Study
- Does Diabetes Care Differ by Type of Chronic Comorbidity?: An evaluation of the Piette and Kerr framework
- Health Coaching to Improve Hypertension Treatment in a Low-Income, Minority Population
- Treatment Adjustment and Medication Adherence for Complex Patients With Diabetes, Heart Disease, and Depression: A Randomized Controlled Trial
- Treatment Intensification in a Hypertension Telemanagement Trial: Clinical Inertia or Good Clinical Judgment?
- Effective Use of Structured Self-Management of Blood Glucose in Type 2 Diabetes: Lessons From the STeP Study
- A Logic Model Framework for Evaluation and Planning in a Primary Care Practice-based Research Network (PBRN)
- Diabetes Performance Measures: Current Status and Future Directions
- Consensus Report: Diabetes Performance Measures: Current Status and Future Directions
- Why system inertia makes health reform so difficult
- Impact of Electronic Health Record Clinical Decision Support on Diabetes Care: A Randomized Trial
- The Chronic Care Model and Exercise Discussions during Primary Care Diabetes Encounters
- Cardiometabolic treatment decisions in patients with type 2 diabetes: the role of repeated measurements and medication burden
- Participatory Decision Making, Patient Activation, Medication Adherence, and Intermediate Clinical Outcomes in Type 2 Diabetes: A STARNet Study
- Antidepressant Medication Use for Primary Care Patients with and without Medical Comorbidities: A National Electronic Health Record (EHR) Network Study
- Features of the Chronic Care Model (CCM) Associated with Behavioral Counseling and Diabetes Care in Community Primary Care
- Diabetes and Poor Disease Control: Is Comorbid Depression Associated With Poor Medication Adherence or Lack of Treatment Intensification?
- The Decision to Intensify Therapy in Patients with Type 2 Diabetes: Results from an Experiment Using a Clinical Case Vignette
- Comparing Methods of Measuring Treatment Intensification in Hypertension Care
- Factors Associated With Intensification of Oral Diabetes Medications in Primary Care Provider-Patient Dyads: A Cohort Study
- The Gordian Knot of Chronic Illness Care
- The Medical Home: Growing Evidence to Support a New Approach to Primary Care
- The Potential of Group Visits in Diabetes Care
- Is 'Clinical Inertia' Blaming Without Understanding? Are Competing Demands Excuses?
- In This Issue: New Concepts for Diabetes and Chronic Disease Management