
Article Figures & Data
Figures
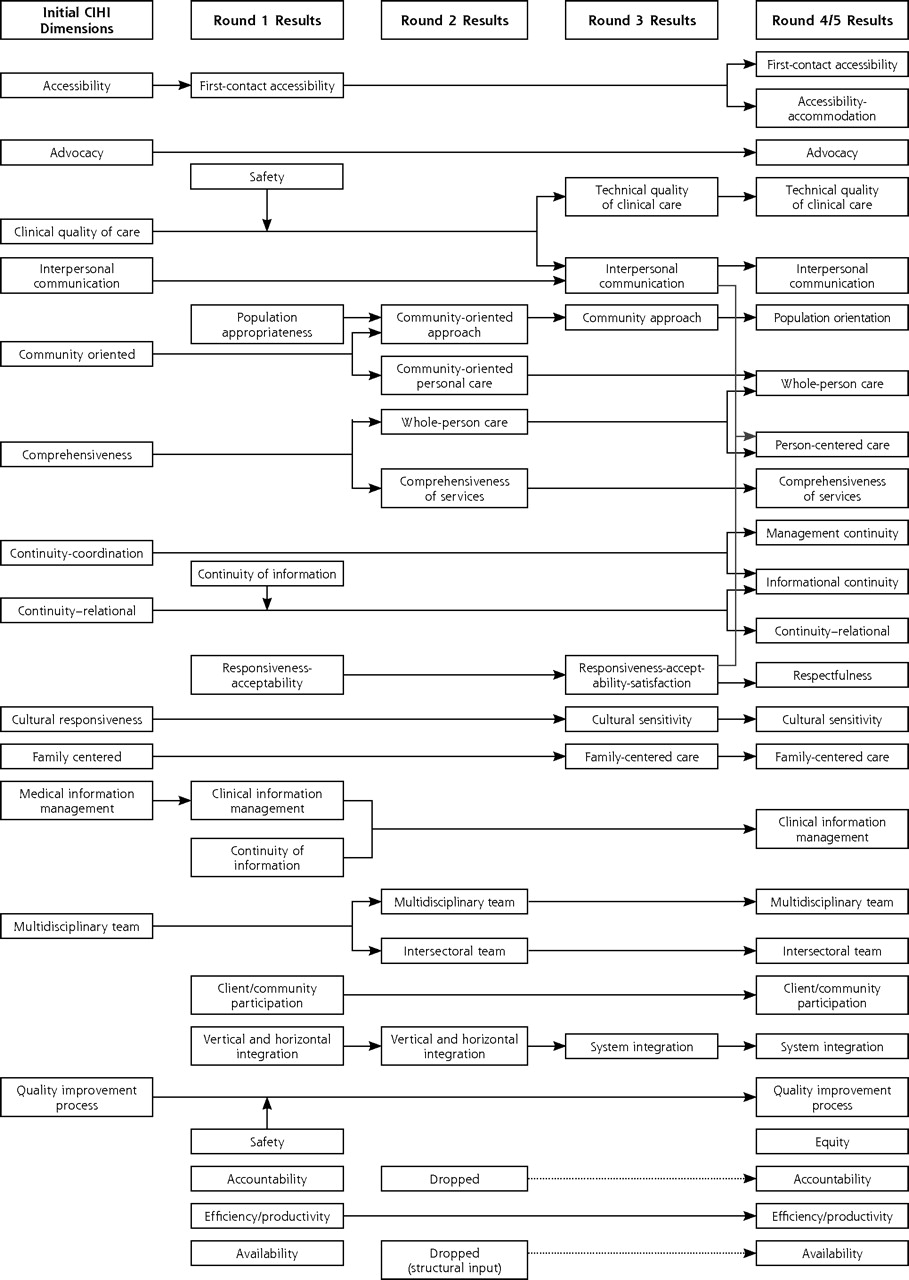
- Figure 1.
Evolution of primary health care dimensions in Delphi consultation.

Tables
- Table 1.
Attributes of Primary Health Care, Grouped by Type, Showing Specificity to Primary Health Care and Best Information Source for Measurement
Best Information Source for Evaluation Attribute* Specific to Primary Care Patient Clinician Report Administrative Data Chart + = Appropriate source mentioned by 1 or 2 experts; ++ = best source according to several experts (this attribute was introduced at the last consensus event); +++ = best source according to all experts. * Attributes in alphabetical order within groupings. † Although the quality of comprehensiveness is not specific to primary health care, the content is. ‡ Proposed at the last meeting but not submitted for consensus. Clinical practice attributes Accessibility, fist-contact Yes +++ Accessibility-accommodation Not assessed Comprehensiveness of services No (?)† ++ ++ + + Informational continuity (new)‡ Not assessed Management continuity No +++ + Technical quality of clinical care No ++ (peer) ++ Practice structural dimensions Clinical information management No + ++ + + Multidisciplinary team No + +++ Quality improvement process No +++ + System integration No + +++ Person-oriented dimensions Advocacy No ++ ++ Continuity – relational Yes +++ + Cultural sensitivity No +++ + Family-centered care Yes +++ + + Interpersonal communication No +++ + Respectfulness No +++ Whole-person care No +++ + Community-oriented dimensions Client/community participation No ++ ++ Equity Not assessed ++ + + Intersectoral team Yes +++ + Population orientation Yes + ++ + System performance dimensions Accountability No ++ (peer) + (self) ++ Availability No + + (self) ++ Efficiency/productivity No +++ + - Table 2.
Attributes of Primary Health Care: Final Operational Definitions and Degree of Consensus Achieved
Concept: Operational Definition Degree of Consensus Note: New attributes were suggested at the last meeting but not submitted to the consensus process. * This definition is nonoperational. Clinical practice attributes First-contact accessibility: The ease with which a person can obtain needed care (including advice and support) from the practitioner of choice within a time frame appropriate to the urgency of the problem High Accessibility-accommodation: The way primary health care resources are organized to accommodate a wide range of patients’ abilities to contact health care clinicians and reach health care services. (The organization of characteristics such as telephone services, flexible appointment systems, hours of operation, and walk-in periods) New Comprehensiveness of services: The provision, either directly or indirectly, of a full range of services to meet patients’ health care needs. This includes health promotion, prevention, diagnosis and treatment of common conditions, referral to other clinicians, management of chronic conditions, rehabilitation, palliative care and, in some models, social services High Informational continuity: The extent to which information about past care is used to make current care appropriate to the patient New Management continuity: The delivery of services by different clinicians in a timely and complementary manner such that care is connected and coherent High Technical quality of clinical care: The degree to which clinical procedures reflect current research evidence and/or meet commonly accepted standards for technical content or skill High Structural dimensions Clinical information management: The adequacy of methods and systems to capture, update, retrieve, and monitor patient data in a timely, pertinent, and confidential manner High Multidisciplinary team: Practitioners from various health disciplines collaborate in providing ongoing health care High Quality improvement process: The institutionalization of policies and procedures that provide feedback about structures and practices and that lead to improvements in clinical quality of care and provide assurance of safety High System integration: The extent to which the health care unit organization has established and maintains linkages with other parts of the health care and social service system to facilitate transfer of care and coordinate concurrent care between different health care organizations High Person-oriented dimensions Advocacy: The extent to which clinicians represent the best interests of individual patients and patient groups in matters of health (including broad determinants) and health care Moderate Continuity-relational: A therapeutic relationship between a patient and one or more clinicians that spans various health care events and results in accumulated knowledge of the patient and care consistent with the patient’s needs High Cultural sensitivity: The extent to which a clinician integrates cultural considerations into communication, assessment, diagnosis, and treatment planning High Family-centered care: The extent to which the clinician considers the family (in all its expressions) and understands its influence on a person’s health and engages it as a partner in ongoing health care Moderate Interpersonal communication: The ability of the clinician to elicit and understand patient concerns, explain health care issues, and engage in shared decision making, if desired High Respectfulness: The extent to which health professionals and support staff meet users’ expectations about interpersonal treatment, demonstrate respect for the dignity of patients, and provide adequate privacy High Whole-person care: The extent to which a clinician elicits and considers the physical, emotional, and social aspects of a patient’s health and considers the community context in their care Moderate Community-oriented dimensions Client/community participation: The involvement of clients and community members in decisions regarding the structure of the practice and services provided (eg, advisory committees, community governance) Moderate Equity: The extent to which access to health care and quality services are provided on the basis of health needs, with-out systematic differences on the basis of individual or social characteristics High Intersectoral team: The extent to which the primary care clinician collaborates with practitioners from nonhealth sectors in providing services that influence health Low Population orientation: The extent to which the primary care clinicians assess and respond to the health needs of the population they serve. (In professional models, the population is the patient population served; in community models, it is defined by geography or social characteristics) High System performance Accountability: The extent to which the responsibilities of professionals and governance structures are defined, their performance is monitored, and appropriate information on results is made available to stakeholders Moderate Availability: The fit between the number and type of human and physical resources and the volume and types of care required by the catchment population served in a defined period of time High Efficiency/productivity: Achieving the desired results with the most cost-effective use of resources* Low
The Article in Brief
Operational Definitions of Attributes of Primary Health Care: Consensus Among Canadian Experts
Jeannie Haggerty, PhD, and colleagues
Background In 2004, the authors consulted with Canadian primary health care experts. Their goal was to develop definitions of key primary care system features to be evaluated in Canada�s health care system.
What This Study Found This process resulted in 25 operational definitions of features of primary health care. Those that are specific to primary care are first-contact, accessibility, relational continuity, family-centered care, population orientation, and intersectoral teamwork. (The last 2 refer to community-oriented models of primary care.)
Implications
- These measurable definitions will help in efforts to assess initiatives to renew primary health care and will serve as a guide for instrument selection.
- To get a valid and global evaluation of primary health care, data are needed from a variety of sources, including patients, clinicians, and administrative data.




{kind=link}
Jump to section
Related Articles
Cited By...
- Quality of primary healthcare for chronic diseases in low-resource settings: evidence from a mixed methods study in rural China
- Socio-economic and Demographic Factors Influencing Interpersonal Communication Between Patients and Family Physicians: A Protocol for a Systematic Review
- Evaluation of the introduction of QOF quality improvement modules in English general practice: early findings from a rapid, qualitative exploration of implementation
- Team-based care Evaluation and Adoption Model (TEAM) Framework: Supporting the comprehensive evaluation of primary care transformation over time
- Primary care bonus payments and patient-reported access in urban Ontario: a cross-sectional study
- Comparison between primary care service delivery in Malaysia and other participating countries of the QUALICOPC project: a cross-sectional study
- Engagement of nurse practitioners in primary health care in northern British Columbia: a mixed-methods study
- How to implement patient experience surveys and use their findings for service improvement: a qualitative expert consultation study in Australian general practice
- Evaluating the implementation of collaborative teams in community family practice using the Primary Care Assessment Tool
- Patients perceptions of access to primary care: Analysis of the QUALICOPC Patient Experiences Survey
- Analysis of definitions of general practice, family medicine, and primary health care: a terminological analysis
- Alignment of Canadian Primary Care With the Patient Medical Home Model: A QUALICO-PC Study
- First contact: what does it mean for family practice in 2017?
- Academic family health teams: Part 1: patient perceptions of core primary care domains
- Academic family health teams: Part 2: patient perceptions of access
- Integrated Primary Care Teams (IPCT) pilot project in Quebec: a protocol paper
- Improving awareness, accountability, and access through health coaching: Qualitative study of patients' perspectives
- Should we use outcomes data to help manage general practice?
- Patients assessments of the continuity of primary care in Finland: a 15-year follow-up questionnaire survey
- Patient-reported confidence in primary healthcare: are there disparities by ethnicity or language?
- Patient-reported access to primary care in Ontario: Effect of organizational characteristics
- Family-centred care delivery: Comparing models of primary care service delivery in Ontario
- Understanding of family medicine in Africa: a qualitative study of leaders views
- Measuring Patients' Perceptions of Patient-Centered Care: A Systematic Review of Tools for Family Medicine
- Family practice registered nurses: The time has come
- Community orientation in primary care practices: Results from the Comparison of Models of Primary Health Care in Ontario Study
- In This Issue: Clinical Diagnosis and Management