
Article Figures & Data
Figures
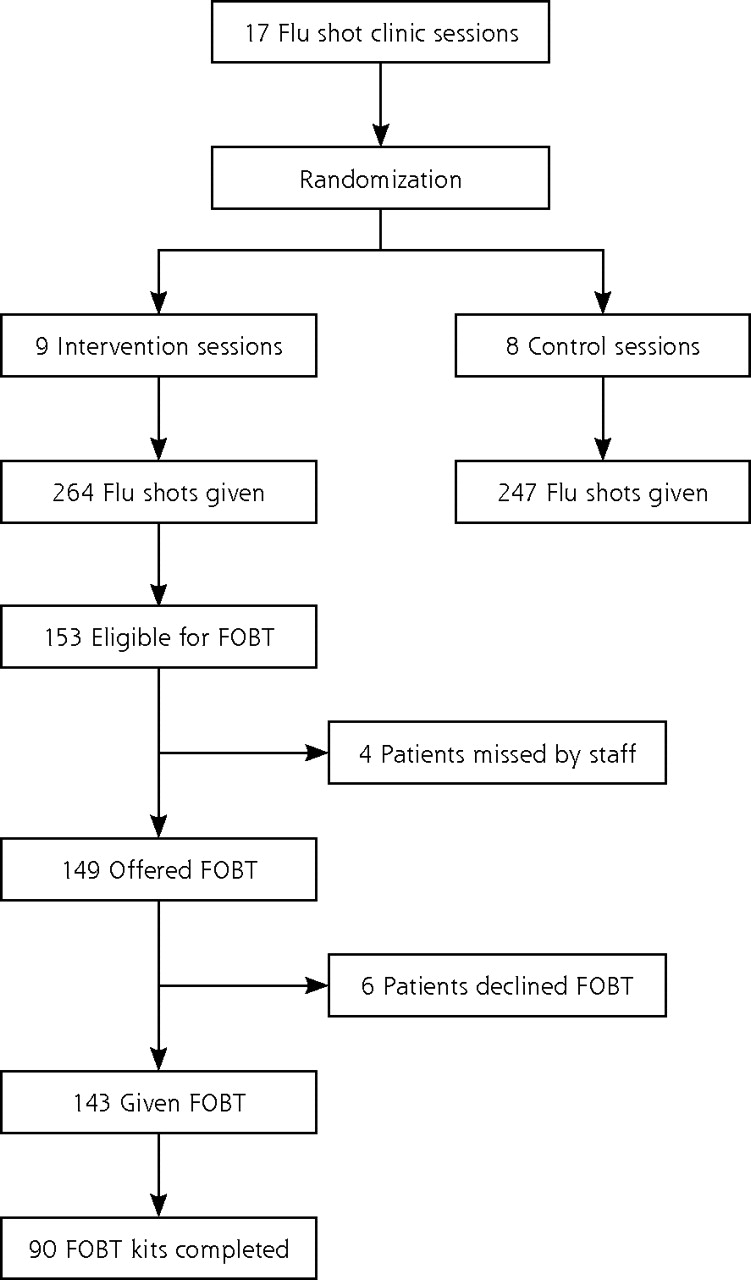
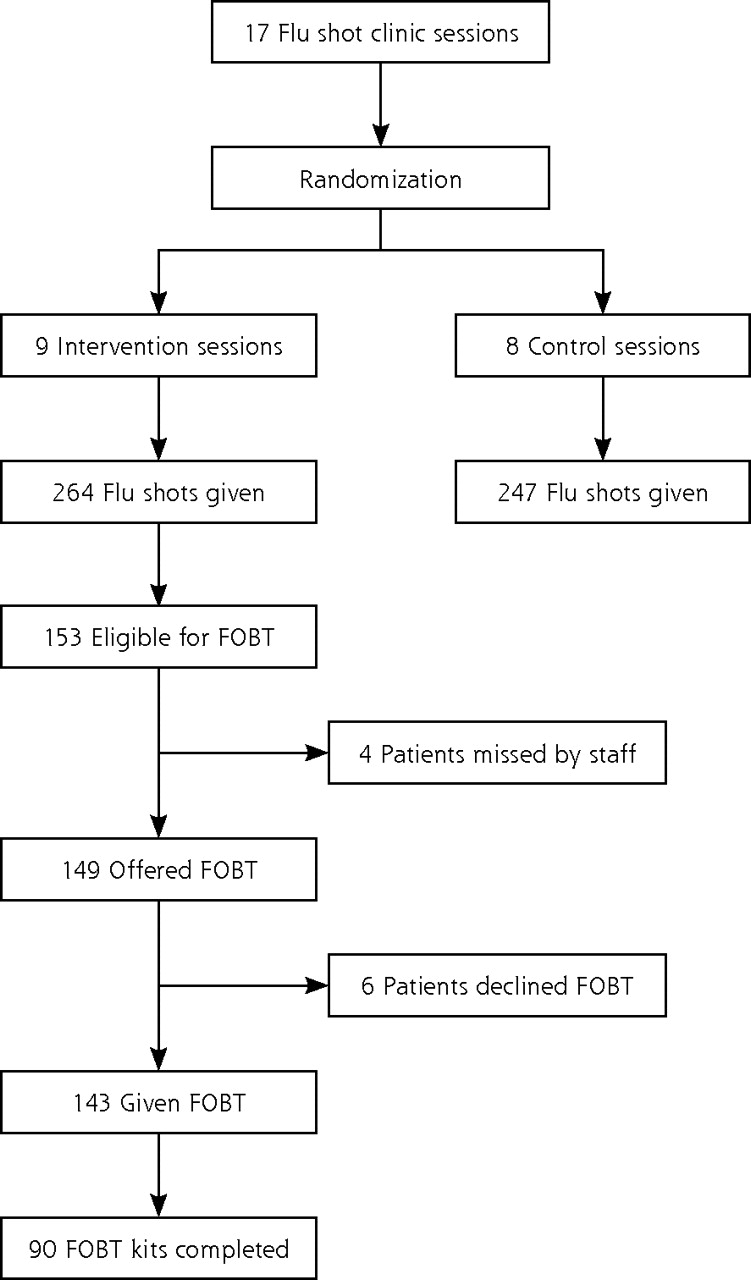
- Figure 1.
Flow diagram for study participants.
Tables
- Table 1.
Demographic Characteristics of Study Participants (N = 514) in the Control and Intervention Groups
Characteristics Control (n=246) Intervention (n=268) P Value CRCS = colorectal cancer screening; DCBE = double-contrast barium enema; FOBT = fecal occult blood test; FS = flexible sigmoidoscopy. a 2-sample t test. b Pearson χ2 test. Age, mean (SD), years 65.6 (7.4) 63.7 (7.6) .004a Female sex, % 65.9 61.2 .273b Ethnicity, % .142b African American 6.1 5.6 Asian/Pacific Islander 56.1 48.1 Latino 25.2 35.8 Non-Latino white 9.8 7.8 Other/unknown 2.8 2.6 Non-English primary language, % 75.6 72.0 .392b Economic indicator: insurance, % .638b Medicare 43.5 40.3 Medicaid 37.0 38.4 Uninsured 17.9 20.5 Other 1.6 0.8 Economic indicator: yearly income, mean (SD), $ 10,967 (6,377) 9,785 (6,383) .036a Health care access in the last year Primary care visits, mean (SD), No. 6.0 (3.7) 5.4 (3.5) .091a One or more hospitalizations, % 4.9 8.2 .129b One or more emergency department visits, % 7.3 10.4 .214b Preintervention flu shot and CRCS status, % Received flu shot in last year 68.7 69.8 .792b Baseline status for CRCS tests, % FOBT in last 12 months 36.2 35.4 .863b FS in last 5 years 9.8 10.5 .795b DCBE in last 5 years 1.6 1.1 .621b Colonoscopy in last 10 years 16.3 17.2 .784b - Table 2.
Preintervention and Postintervention Changes in Percentage of Study Participants Up-to-Date with Colorectal Cancer Screening in the Control and Intervention Groups
CRCS Status Control (n=246) Intervention (n=268) Between Group P Value CRCS=colorectal cancer screening. a Pearson χ2 test. b 2-sample Wilcoxon rank-sum test on the preintervention-postintervention difference scores. c McNemar test. CRCS up-to-date before influenza season (October 16, 2006), % 52.9 54.5 .711a CRCS up-to-date after influenza season (March 31, 2007), % 57.3 84.3 <.001a Percentage point change +4.4 (−0.7 to 9.7) +29.8 (23.7 to 36.0) <.001b Preintervention to postintervention P valuec .071 <.001 - Table 3.
Postintervention Percentage of Study Participants Up-to-Date With Colorectal Cancer Screening According to Baseline Screening Status (Initially Up-to-Date or Initially Not Up-to-Date)
Study Participants Control No. (%) Intervention No. (%) P Valuea a Pearson χ2 test. Total patients initially not up-to-date 116 122 Patients who became up-to-date 24 (20.7) 83 (68.0) <.001 Total patients initially up-to-date 130 146 Patients who remained up-to-date 117 (90.0) 143 (98.0) <.005 - Table 4.
Multivariate Logistic Regression Analysis of Predictors of Being Up-to-Date with Colorectal Cancer Screening at End of Influenza Season (March 31, 2007) for Study Participants (N = 514)
Predictor Variable Patients Initially Overdue for CRCS (n=238) OR (95% CI) Patients Initially Up-to-Date for CRCS (n=276) OR (95% CI) CRCS=colorectal cancer screening; OR=odds ratio. a P <.001 for comparison with reference category. b P <.05 for comparison with reference category. Study arm, intervention (vs control) 11.3 (5.8–22.0)a 5.8 (1.5–22.0)a Age, 50–64 y (vs 65–79 y) 0.8 (0.4–1.5) 1.0 (0.3–3.4) Sex, male (vs female) 1.1 (0.6–2.1) 2.5 (0.7–9.3) Ethnicity, Hispanic (vs Asian) 0.8 (0.4–1.6) 0.4 (0.1–1.3) Other (vs Asian) 0.5 (0.2–1.1) 1.7 (0.2–15.9) Primary language, English (vs non-English) 0.8 (0.4–1.8) 2.0 (0.4–10.0) Insurance, insured (vs uninsured) 1.4 (0.6–3.2) 1.3 (0.3– 5.2) Income, above median (vs below) 2.0 (1.1–3.8)b 0.7 (0.2–2.0) Primary care visits, above median (vs below median) 2.0 (1.0–3.7)b 0.7 ( 0.2–2.3)
The Article in Brief
Offering Annual Fecal Occult Blood Tests During Flu Shot Clinics Increases Colorectal Cancer Screening Rates
Michael B. Potter , and colleagues
Background Only about one-half of eligible adults aged 50 years and older report being up-to-date on screening for colorectal cancer. The home fecal occult blood test (FOBT) is the least expensive screening method, but there are often educational, linguistic, ethnic, social, or cultural barriers to its use. This study examines whether offering home FOBT tests during annual flu shot clinics is an effective way to increase rates of colorectal cancer screening.
What This Study Found Offering home FOBT to eligible patients at a primary care-based annual flu shot clinic dramatically increases colorectal cancer screening rates among those in attendance. In this study of 514 patients at an annual flu shot clinic, screening rates increased by almost 30 percentage points among those offered an FOBT compared with an insignificant increase of 4 percentage points in screening among those who weren't offered the test.
Implications
- Annual flu shot activities provide an opportunity for nonphysician staff to offer FOBT to patients older than 50 years who need it at a time when they are already thinking about illness prevention.
- Combining annual FOBT and flu shot activities could become an effective way to promote colorectal cancer screening in primary care settings, especially in communities and clinics where FOBT remains the primary screening option.
Annals Journal Club Selection:
Jan/Feb 2009
The Annals of Family Medicine encourages readers to develop the learning community of those seeking to improve health care and health through enhanced primary care. You can participate by conducting a RADICAL journal club, and sharing the results of your discussions in the Annals online discussion for the featured articles. RADICAL is an acronym for: Read, Ask, Discuss, Inquire, Collaborate, Act, and Learn. The word radical also indicates the need to engage diverse participants in thinking critically about important issues affecting primary care, and then acting on those discussions.1How it Works
In each issue, the Annals selects an article or articles and provides discussion tips and questions. We encourage you to take a RADICAL approach to these materials and to post a summary of your conversation in our online discussion. (Open the article online and click on "TRACK Comments: Submit a response.") You can find discussion questions and more information online at: http://www.AnnFamMed.org/AJC/.
Article for Discussion
- Potter MP, Phengrasamy L, Hudes ES, McPhee SJ, Walsh JME. Offering home fecal occult blood tests at flu shot clinics increases colorectal cancer screening rates. Ann Fam Med. 2009;7(1):17-23.
Discussion Tips
This clinical trial shows a dramatic effect of adding fecal occult blood testing to flu shot clinics. In addition to critiquing the article, it may be worthwhile to consider how the findings might be reinvented in your practice setting.Discussion Questions
- What question is addressed by the article? How does the question fit with what already is known on this topic?
- How does theory inform the intervention design?
- How strong is the study design for answering the question?
- How do the study methods compare with the CONSORT criteria for clinical trials?2 What adjustments in the criteria are necessitated by the randomization of clinic days rather than individuals?
- What is the degree to which can the findings be accounted for by:
- How participants were selected? The exclusion criteria and drop outs? Are any biases likely to be important?
- How outcomes were measured?
- Confounding (false attribution of causality because 2 variables discovered to be associated actually are associated with a 3rd factor)?
- How information was interpreted?
- Chance?
- What are the main findings? How large is the effect?
- What do we learn from the secondary analyses of factors associated with variations in screening completion, and from the description of attempts to follow up patients with positive fecal occult blood tests? What factors affect interpretation of these findings that are less an issue with interpreting the main effects of the clinical trial?
- How transportable are the findings to your clinical setting? What factors might affect this transportability?
- What are some next steps for applying the findings or answering other questions that this study raises?
References
- Stange KC, Miller WL, McLellan LA, et al. Annals journal club: It�s time to get RADICAL. Ann Fam Med. 2006;4:196-197. http://annfammed.org/cgi/content/full/4/3/196.
- CONSORT Group. CONSORT: Consolidated Standards of Reporting Trials. http://www.consort-statement.org/. Accessed Oct 26, 2008.




{kind=link}
Jump to section
Related Articles
Cited By...
- Faecal immunochemical tests versus guaiac faecal occult blood tests: what clinicians and colorectal cancer screening programme organisers need to know
- Feasibility of a call-in centre to deliver colorectal cancer screening in primary care
- System-Based Participatory Research in Health Care: An Approach for Sustainable Translational Research and Quality Improvement
- Implementation Insights
- Annals Journal Club: Symbiosis Instead of Competing Demands: A Tale of Two Preventive Services
- The Aftermath of Efficacy
- The Complexity of and Opportunity for Screening in Primary Care