
Abstract
PURPOSE The patient-centered medical home (PCMH) is a widely accepted theory of a practice model to improve quality of care, patient satisfaction, and access to primary care services. This study explores existing elements of the PCMH and characteristics of family practices in Virginia.
METHOD We developed and administered a survey questionnaire to capture information on practice characteristics and PCMH elements. We randomly sampled 700 family medicine offices in Virginia from a population of practices derived from the Virginia Board of Medicine Practitioner Information Database. We used a mixed-mode survey, allowing practices in the sample to respond by mail or Internet or at a regional family medicine conference.
RESULTS The survey resulted in a response rate of 56%, with 342 office locations participating in the study. Most practices reported continuity-of-care processes (87%) and clinical guidelines (77%). Fewer reported use of patient surveys (48%), electronic medical record for internal coordination (38%), community linkages for care (31%), and clinical performance measurement (28%). A small number reported patient registries for multiple diseases (19%). Very few practices exhibited all elements outlined in the PCMH model (1%). Practice size (number of physicians) is significantly related to PCMH model alignment.
CONCLUSIONS Most family practices in Virginia exhibit some elements of the PCMH model. Full implementation of the PCMH model is low. Baseline information on practice characteristics, prevalence of PCMH, and challenges of small practices should be considered in guiding efforts, evaluating progress, and developing policies for care model reform.
INTRODUCTION
There has been a growing movement in the last several years to transform family practices to improve access, quality of care, and business functionality. A new model of practice was proposed in 2004 under the Future of Family Medicine1 project to align family medicine with the needs of the population and to meet the goals proposed by the Institute of Medicine to provide care that is patient-centered, safe, timely, and equitable.2 The new model was designed to meet these goals by emphasizing team-based, proactive care supported by effective office systems, technology, and a culture of improvement.1
The medical home has now gained recognition as a promising solution for primary care practices to deliver accessible, high-quality care.3 The patient-centered medical home (PCMH)4 consists of 7 core features agreed upon by multiple medical societies representing primary care physicians. The core features of the PCMH, Table 1⇓, are comprised of elements representing either services provided to patients or characteristics of the practice. PCMH core features are thought to improve access, quality, patient satisfaction, and care coordination.5
Core Features and Corresponding Elements of the Patient-Centered Medical Home4
The model is now a central theme in both federal and state legislation, including a Medicare Demonstration Project6 under the Tax Relief and Health Care Act of 2006 and a recognition program from the National Committee of Quality Assurance (NCQA).7 Despite excitement about the PCMH, there is little information on the degree of practice alignment to PCMH core features. Two previous studies addressed structural components of the PCMH in practices of various specialties. A study conducted by Rittenhouse et al focused on large group practices (those with 20 or more physicians).8 Another study in Massachusetts focused on practices with 2 or more physicians.9 No studies addressed PCMH components in family practices of all sizes.
The goal of our study was to understand the model of care and characteristics of family practices in Virginia. We conducted a survey of practices that resulted in information on most PCMH core features. Certain features and characteristics could not be captured through a practice survey, such as payment reform and patient perception on whether they participated in medical care decision making. We report on characteristics of family practices in Virginia and describe practices’ alignment to 6 of the 7 core features of the PCMH.
METHODS
We used a cross-sectional research design to obtain practice information on characteristics, model of care, and patient services. The Institutional Review Board at Virginia Commonwealth University approved the study.
Survey Methods
Primary data were collected through a survey that included 45 questions based, in part, on the National Survey of Physician Organizations.10 (Our survey questionnaire can be found as a Supplemental Appendix, available at http://www.annfammed.org/cgi/content/full/7/4/301/DC1.) This questionnaire consisted of questions on the use of ancillary care clinicians, patient registries, patient self-management, scheduling arrangements, clinical guidelines, patient surveys, electronic medical record (EMR), continuity of care, community linkages, translation services, performance measurement, teamwork programs, and other practice characteristics. The questionnaire was pretested for clarity and understanding with 8 physicians and 1 family medicine nurse-practitioner. Survey questions were revised based on input received during the pretest.
Population Database
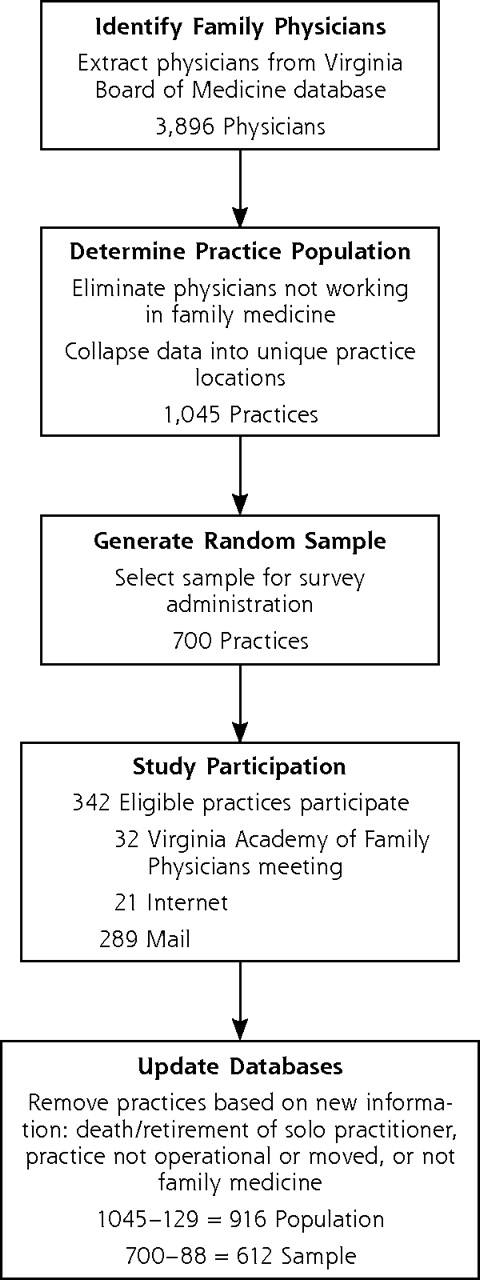
Our study population comprised all Virginia family practices that had at least 1 physician practicing family medicine and that were not a free clinic or pure urgent care center. No complete list of family practices in Virginia existed before this study. We used the Virginia Board of Medicine Practitioner Information Database11 to collect information on all certified family medicine physicians in the state of Virginia (n = 3,896) (Figure 1⇓). We removed physicians not working in family medicine, such as hospitalists, emergency room physicians, and sports medicine specialists. We then collapsed physician information into a list of 1,045 unique office locations. The population database was updated during administration of the questionnaire as new information became available that indicated the practice was not family medicine or was not currently operational. This process resulted in 916 unique family practice locations in Virginia.

Derivation of Study Sample
Recruitment of Practices
The survey was undertaken August 2007 through January 2008, with questionnaires distributed to a randomly selected sample12 of 700 practices in Virginia. We asked physicians to respond to the survey because they are in the best position to provide information on practice characteristics and patient services.
We used mixed-mode methods13 to administer the questionnaire: the mail, the Internet, and at the 2007 Virginia Academy of Family Physicians (VAFP) annual meeting. The objective was to obtain 1 completed questionnaire from each practice in the sample. During the VAFP meeting 32 questionnaires were received from unique practice locations that fell within our sample of 700 practices. The questionnaire was then mailed to the remaining 668 practices in the sample with a cover letter including instructions to complete the questionnaire for that office location and return it by mail or over the Internet. Twenty-one practices submitted their questionnaires online. Another 289 practices completed and returned the hard copy of the questionnaire. The sample was adjusted based on information that indicated the practice was not family medicine or was not operational, which reduced the sample to 612 practices, for a 56% response rate, with 342 unique office locations participating in the study.
Measurement of PCMH Features
Elements Associated with PCMH Core Features
To measure the personal physician feature, we asked a yes-or-no question on whether the practice has specific processes to ensure continuity of care so that most of the time patients receive care from their personal physician. To measure the physician-directed medical team feature, we asked practices whether they use nurses, nurse-practitioners, physician’s assistants, medical assistants, mental health specialists, and patient educators and whether they offered programs for improving employee morale and teamwork. Our measurement of the whole-person orientation feature consisted of 2 questions on the types of patients seen and types of care provided. The measurement assessing the care coordination and integration feature consisted of multiple questions on whether the practice uses a patient registry for specific diseases, uses an EMR, provides community linkages for care, and provides linguistic services for non-English speaking patients. Our measurement of the enhanced access to care feature was based on a question asking whether the practice provides alternative scheduling arrangements, such as scheduled evening or weekend visits. The measurement to assess the quality and safety feature consisted of questions on whether the practice uses clinical guidelines, patient satisfaction surveys, performance measurement for clinical activities, and performance feedback to physicians.
Composite Measures of PCMH
PCMH core features were measured in this study with 14 elements representing infrastructure or services that support a PCMH model. Practices could score 1 point per element, resulting in a PCMH element index for each practice that ranged from 0 to 14. Multiple elements contained yes-or-no questions, such as whether the practice offered programs for employee morale and teamwork. Several elements required the measurement of multiple components, such as the numerous functions possible in an EMR. Practices were awarded 1 point if they responded yes to 50% or more of components for each element. A more stringent threshold, 100%, was applied to the elements representing type of care, patients seen, and patient surveys. We also calculated an index for PCMH core features that ranged from 0 to 6. Practices could score 1 point per PCMH core feature if they exhibited all elements contained in a feature.
Data Analysis
We used standard descriptive statistics to summarize sample characteristics and frequency distributions to determine the number and percentage of practices that used PCMH elements. Regression analyses were conducted to examine the relationship between practice size and the existence of PCMH elements and core features.
RESULTS
Sample-Population Comparison
We compared family practices in the sample (n = 342) with the population (N = 916). Responding practices did not differ significantly from the population based on region, rural or urban location, and acceptance of Medicare and Medicaid (Table 2⇓).
Comparison of Sample With Population Characteristics
Organizational Characteristics
Practices, generally, were single specialty, private, for-profit, and not owned by an outside entity (Table 3⇓). Most practices in the sample were small (less than 20 physicians).
Organizational Characteristics of Participating Family Practices (N = 342)
Elements of the PCMH
Table 4⇓ displays the number and percentage of practices that reported each PCMH element and the index scores for core features.
Measured Elements and Core Features of the Patient-Centered Medical Home (N = 342)
Personal Physician
A high percentage of family practices, 87.4%, reported processes to ensure continuity of care so that most of the time patients received care from their personal physician.
Physician-Directed Medical Team
Most practices (86.8%) used at least 1 ancillary care clinician, whereas 34.8% of practices used 3 or more. More than 60% used nurses, and almost 50% used medical assistants. Patient educators, physician’s assistants, and mental health specialists were used to a lesser extent. More than one-half, 52.9%, of practices reported programs for employee morale and teamwork.
Whole-Person Orientation
A high percentage of practices, 74.3%, had implemented whole-person orientation as it relates to age of patients and types of care provided. Almost all family practices reported the provision of chronic, acute, and preventative care. Approximately 75% of practices reported treating patients of all age-groups.
Care Coordination and Integration
Less than 5% of practices reported patient registries, community linkages for care, an EMR, and provision of linguistic services. Patient registries were used by 33.4% of practices. Diabetes and asthma were the top 2 conditions for patient registries. Few practices reported registries for depression, coronary artery disease, and congestive heart failure. Approximately 30% of family practices reported community linkages for care. Less than 40% reported an EMR. Nearly one-half, 49.1%, of practices reported the provision of linguistic services to facilitate communication with patients.
Enhanced Access
More than 96% reported at least 1 alternative scheduling option. Approximately 36% of practices implemented 3 or more strategies to enhance access to care. Almost 90% reported rapid access techniques for patients to obtain care on short notice, and approximately 40% reported scheduled evenings or weekend visits. Few practices reported group visits and e-mail consultations.
Quality and Safety
Only 17.5% of practices reported implementation of clinical guidelines, patient satisfaction surveys, and performance measurement. Most practices (nearly 77%) reported using clinical guidelines and training physicians in the use of guidelines (approximately 66%). Less than 20% of practices reported an EMR with problem-specific clinical guidelines. Almost 50% of practices reported administering patient satisfaction surveys; the majority of those practices (70%) made improvements based on feedback obtained from patients. A review of performance measurement activities shows that less than 25% of practices reviewed data on results of clinical quality improvement projects, clinician use of evidence-based practices, or outcomes data.
Practice Alignment With the PCMH Model
Elements of the PCMH Model
Of the 342 participating practices, 1.2% reported all 14 elements of the PCHM model. Almost all practices, 97.9%, possess 3 or more elements of the PCMH model; 49.2% possess at least one-half.
Core Features of the PCMH Model
We also measured the alignment of participating practices with the 6 practice level features of the PCMH. Only 1.2% reported all 6 features of the PCHM. The majority of practices, 78.4%, reported 2 or more, and 42.2% reported 3 or more core features.
Practice Size and PCMH Alignment
We conducted regression analyses to investigate the relationship between practice size and PCMH alignment while controlling for area and practice characteristics. The indices for total PCMH elements and total PCMH core features were used as dependent variables with practice size (number of physicians) and several geographic and practice characteristics as explanatory variables. We found that size was significantly related to both total PCMH elements (P = .000) and total PCMH core features (P = .000). Further analyses showed that size is not significantly related to personal physician (P = .299) or enhanced access (P = .122), but it is significantly related to quality and safety (P = .011), whole-person orientation (P = .007), medical team (P = .000), and coordination of care (P = .009).
DISCUSSION
These results indicate that most family practices are aligned with the PCMH model in the areas of whole-person orientation and personal physician. Practices are challenged with other aspects of the PCMH model, particularly areas that require considerable financial and knowledge resources, such as EMRs and performance measurement for clinical activities. Increased attention is needed to transform family practice in the areas of quality and safety, coordination of care, team-based care, and enhanced access to care.
The infrequent prevalence of the PCMH elements in family practices is an important consideration for policy makers and payer organizations in establishing programs and reimbursement methods centered on this model. The present reimbursement system rewards the number of patients seen, so practices naturally structure themselves to see a large number of patients. Practices are not paid for many elements of the PCMH model, which is reflected in this study by the low prevalence of certain PCMH elements. The NCQA recently revised their practice recognition program to incorporate elements of the PCMH.7 The NCQA program focuses heavily on EMR functionality for communication, quality, and care management. Our results indicate that most practices in Virginia would require considerable transformation to meet all requirements of the NCQA recognition program.
The Rittenhouse study of PCMH infrastructure in large group practices showed that very large organizational size was strongly associated with greater alignment with the PCMH model.8 The Massachusetts study showed that larger practices were more aligned with the PCMH model than smaller practices.9 Our results support the findings from these studies. It is clear that many small practices are not aligned with the PCMH model. Either small practices do not have the resources to implement the PCMH model, or certain elements do not make sense for a small practice. Because small practices represent an important component of our health care delivery system, policy makers need to consider the challenges small practices face and should develop specific policies for supporting small practices in developing efficient and effective models of care.
The Rittenhouse study found a higher prevalence of EMRs, patient registries, quality measurement, and performance feedback to physicians.8 Because our study included practices of all sizes, it is not surprising that our results show a lower prevalence of most PCMH elements than the Rittenhouse findings. The Massachusetts study, which looked at capabilities of practices that contribute clinical performance data to a statewide quality initiative, found a much higher prevalence of several PCMH elements—EMR capabilities, assistance for patient self-management, and clinical performance measurement.9 This finding indicates that states focusing on improving quality in primary care practices may have better success at supporting structural components to enhance quality of care. The moderately low existence of PCMH elements reported in our study suggests that additional support from state and national organizations is needed for practice transformation.
Several study limitations should be considered when evaluating our results. A cross-sectional study allows us to capture information on practices at only one point in time. The lack of existing data on family practices in Virginia limits our ability to make detailed comparisons of the sample with the population. As a result, our sample may be unrepresentative on some unmeasured aspects of the practice. The use of a survey instrument to recruit practices may have generated a self-selected sample, thus limiting generalizability. The survey instrument may also have introduced bias resulting from the objectivity of individual survey respondents and variability in interpretation of question wording. Another design limitation is that we collected information from practices in Virginia only, not from all family practices in the United States. We were not able to measure all aspects of the PCMH model. A structured survey of practices cannot capture important information regarding patient perceptions, team cohesiveness, and the appropriateness of elements for a specific practice. These topics should be addressed in future research along with the efficiency and effectiveness of the PCMH model.
This baseline study of the prevalence of PCMH elements among Virginia family practices informs policy makers by indicating what elements need to be reimbursed and supported. Policy makers and medical associations need to understand the number of PCMH elements in practices, the elements and core features that require attention, and strategies to achieve the PCMH model and its potential outcomes, an effort that will take considerable resources and coordination among clinicians, payers, and purchasers of service. It has been estimated that to move a practice from an NCQA-uncertified state to a high-level designation would cost approximately $100,000 per clinician.14
There is clearly a need to evaluate and disseminate such innovations among family practices. The TransforMED program15 is a major initiative to accomplish this goal on a national level. State chapters and local health care systems can work together to support care model redesign by means of communities of practice16 that focus on solving shared problems. These efforts can be greatly enhanced by collaboration with payers and employers. The National Business Coalition on Health17 and the Patient-Centered Primary Care Collaborative18 are promoting demonstration projects and disseminating successful models. Innovation in family medicine residency education can also make major contributions. Finally, partnerships between academic units of family medicine and community practices may have much to offer in designing, implementing, evaluating, and promoting better care models.
Acknowledgments
We thank Stephen S. Mick, PhD, for his scholarly contribution to this research project. We also thank Lee W. Frederiksen, PhD, for his guidance in developing the survey instrument.
Footnotes
-
Conflicts of Interest: none reported
- Received for publication January 5, 2009.
- Revision received April 9, 2009.
- Accepted for publication May 21, 2009.
- © 2009 Annals of Family Medicine, Inc.




{kind=link}
Jump to section
Related Articles
Cited By...
- Effects of Patient-centered Medical Home Transformation on Child Patient Experience
- Managing Chronic Illness: Physician Practices Increased The Use Of Care Management And Medical Home Processes
- Small And Medium-Size Physician Practices Use Few Patient-Centered Medical Home Processes
- Summary of the National Demonstration Project and Recommendations for the Patient-Centered Medical Home
- Principles of the Patient-Centered Medical Home and Preventive Services Delivery
- In This Issue: Systematic Strategies and Individualized Approaches to Care