
Article Figures & Data
Figures
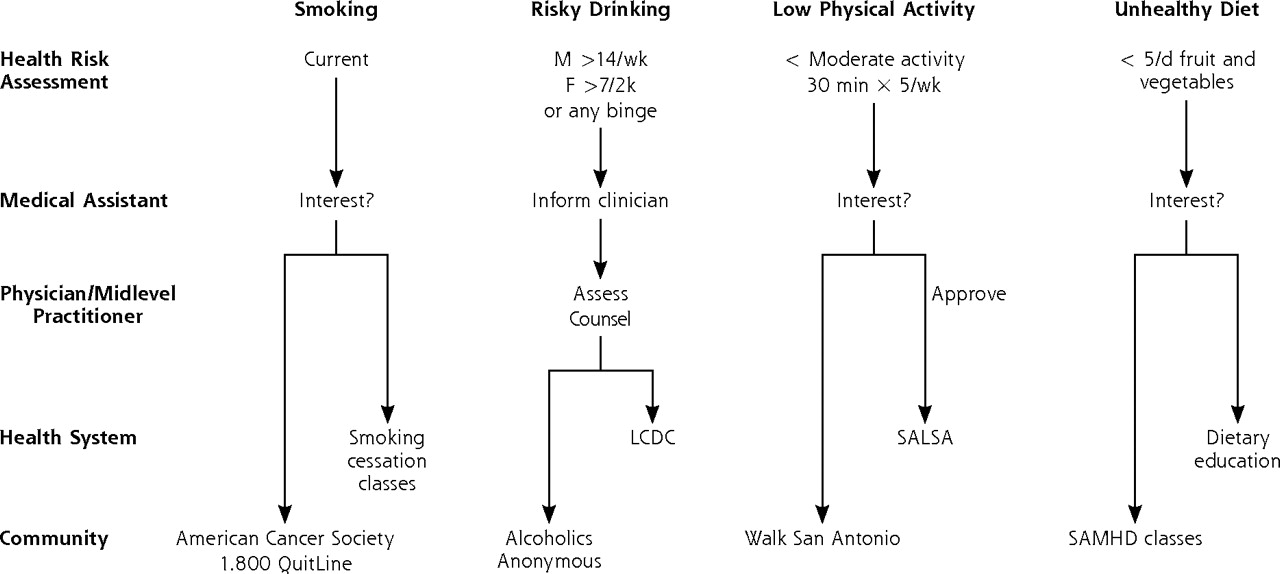
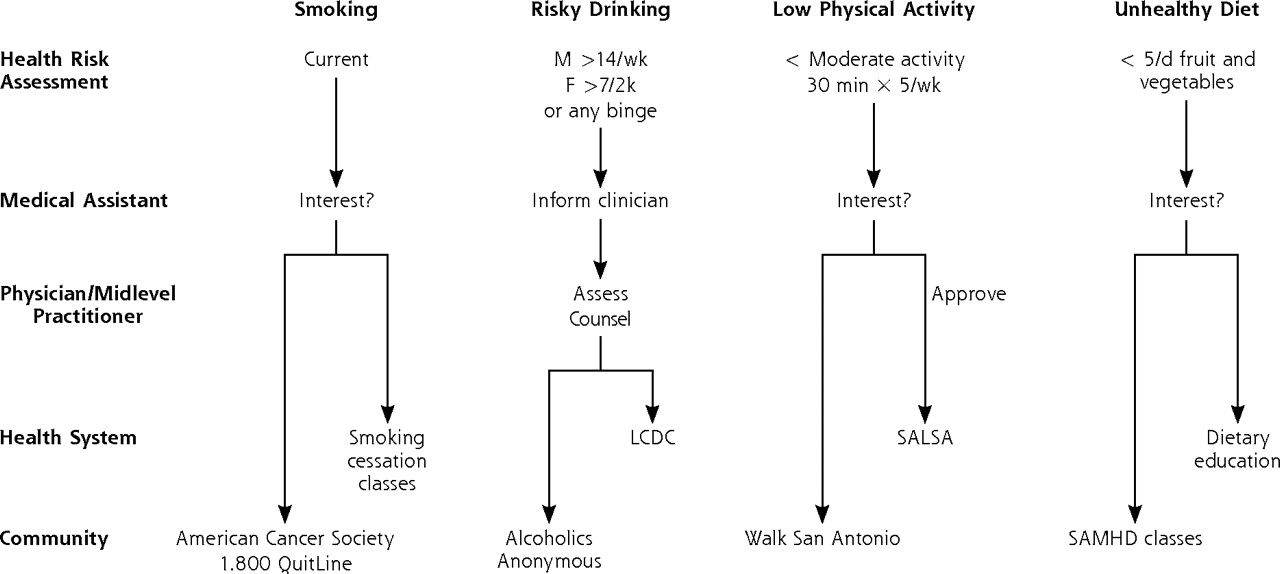
- Figure 1.
Algorithm for medical assistants’ risk behavior assessment and management.
Note: After the health risk assessment, the medical assistant and patient discuss type of referral for smoking, low physical activity, and unhealthy diet. For risky drinking, the medical assistant informs the patient’s clinician and the clinician assesses the need for referral program.
F=female; LCDC=substance abuse clinic; M=male; SALSA=low-impact aerobics, dancing class; SAMHD=San Antonio Metropolitan Health District; Walk San Antonio = community-based walking program at multiple sites.
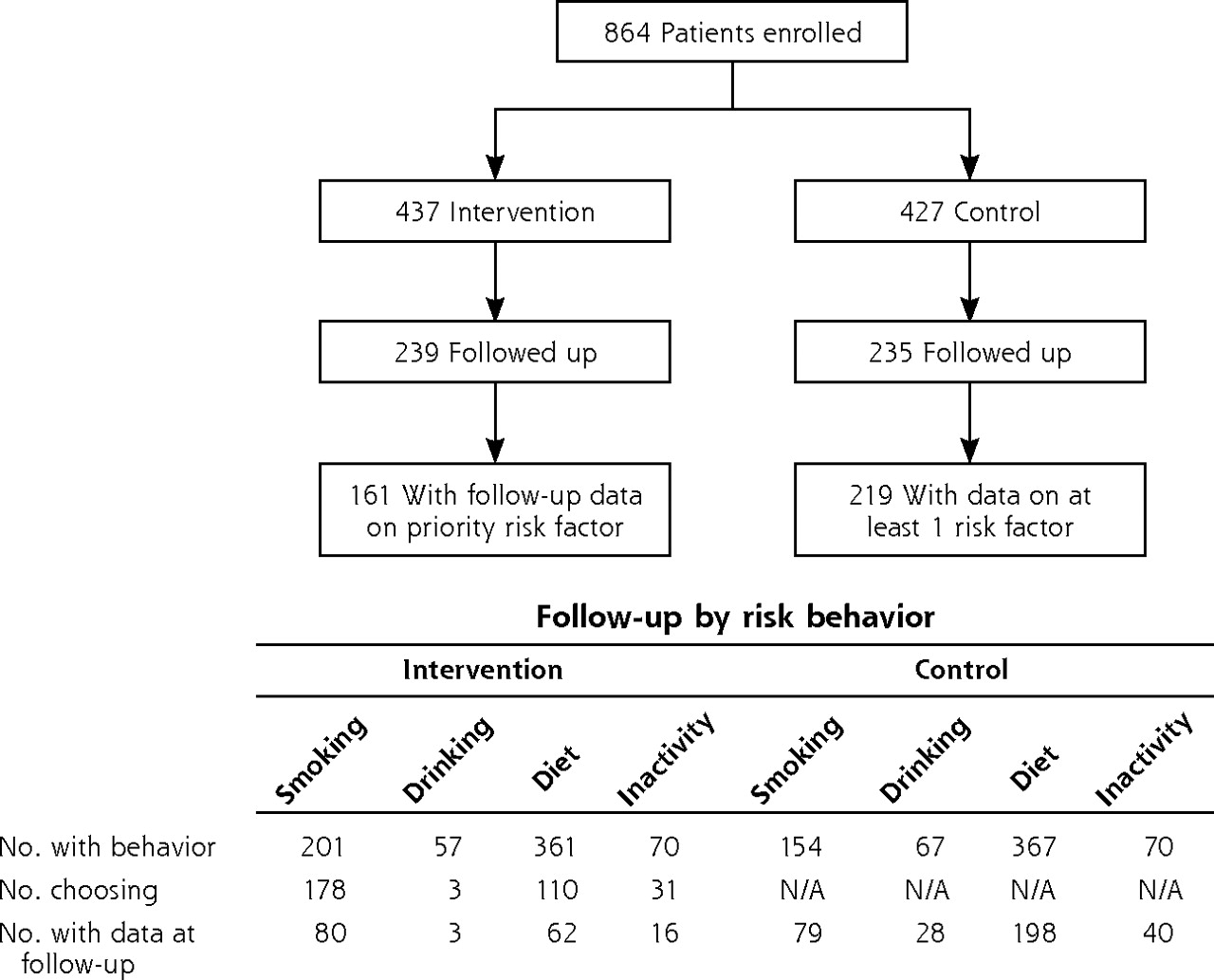
- Figure 2.
Patient flow diagram for randomized trial.
No. with behavior = number of patients with a specified behavioral risk factor. Patients with multiple risk behaviors are counted in more than 1 category. No. choosing = number of patients who chose a specified risk factor as their priority for intervention. Patients could be counted in only 1 category. N/A = patients in the control arm did not choose a priority risk factor for intervention. No. with data at follow-up = number of patients who responded to follow-up questionnaire and who had complete data at baseline and follow-up for the specified risk factor. Intervention patients were counted only in 1 category. Control patients were counted in each category in which they had the specified risk.
Tables
Variable Referral Program N=437 Control N=427 Clinical Populationa Note: Statistical significance evaluated with Fisher’s exact test for categorical variables and 2-sample t test for continuous variables. P >.05 for all comparisons for referral program vs control group, except for mental unhealthy days. a Adult enrollees of Bexar County CareLink Program (see Methods for description). b Target population demographics did not establish these categories separately from Hispanic. c Most, 99.4%, had income <200% of federal poverty limit. d P=.008. Age, mean (SD), y 46.1 (11.6) 46.9 (11.9) 41.0 Female, % 73.7 75.6 57.3 Race and ethnicity, % White, non-Hispanicb 22.6 18.1 Black, non-Hispanic 6.8 7.7 5.2 Hispanic 68.7 71.9 76.4 Other or no responseb 1.9 2.0 – Education, % Not ascertained <12 y 30.5 28.0 – 12 y 35.6 39.6 – >12 y 33.9 32.4 – Income, %c <$10,000 52.7 53.6 – $10–19,999 34.1 32.5 – $20–34,999 10.1 11.9 – >$35,000 3.1 2.1 – Risk behaviors, % Smoking 49.5 50.5 – Risky drinking 18.3 18.9 – Poor diet 93.8 90.0 – Low physical activity 28.5 25.5 – Body mass index (kg/m2) 33.9 33.8 – Unhealthy days, past 30 d Physical, mean 11.7 10.1 – Mental, mean 12.1 9.9d – Risk Behavior Referral Program % (n) Control % (n) Risk Ratio (95% CI) Adjusted Relative Risk (95% CI)a Note: Percentage of patients with specified risk behavior that attended a referral program and adjusted relative risks for referral program and control groups. Numbers in parentheses are denominators for comparisons (intention to treat). Risk ratios and 95% confidence intervals computed with logistic regression; odds ratios converted to relative risk ratios by method of Zhang and Yu.33 Comparison for “any risk behavior” evaluated with 2-sample test of proportions. For comparisons of “any risk behavior,” control group patients can contribute denominator data for multiple risk behaviors. CI=confidence interval. a Adjusted for age, sex, race/ethnicity, and baseline health status. Smoking 75.3 (93) 28.6 (81) 2.25 (1.76–2.62) 2.23 (1.52–2.78) Alcohol 0 (3) 0 (45) – – Diet 60.6 (66) 22.3 (224) 2.30 (1.71–2.03) 1.93 (1.25–2.60) Physical activity 75.0 (16) 26.3 (44) 2.72 (1.61–3.34) 2.02 (0.68–3.17) Any risk behavior 67.4 (177) 21.8 (394) <.001 – - Table 3.
Proportion of Patients With Improved Behavioral Outcomes and Adjusted Relative Risks Comparing Referral Program and Control Groups
Behavior Change Referral Program % (n) Control % (n) Risk Ratio (95% CI) Adjusted Relative Riska (95% CI) Note: Percentage of patients with specified risk behavior that moved to a lower risk category. Numbers in parentheses are denominators for comparisons (intention to treat). Risk ratios and 95% CI computed with logistic regression; odds ratios converted to relative risk ratios by method of Zhang and Yu.33 Comparison for “any risk behavior” evaluated with 2-sample test of proportions. For comparisons of “any risk behavior,” control group patients can contribute denominator data for multiple risk behaviors). Definitions of outcomes: quit smoking = current smoker at baseline (>100 cigarettes in lifetime + smoked in past 7 days) but no smoking in past 7 days at follow-up; quit risky drinking = any binge drinking (5 or more drinks on 1 occasion) or drinking above threshold (>2 drinks per day for men or >1 drink per day for women) in past 30 days at baseline, but neither behavior present in past 30 days at follow-up; eating >5 servings fruit or vegetables = consumed <5 servings per day of fruits or vegetables in past week at baseline, but exceeded that threshold at follow-up; activity >low = inactive by IPAQ algorithm (using minutes per week of sedentary, low, moderate, and vigorous activity) at baseline, but moderate or high at follow-up. CI=confidence interval; IPAQ = International Physical Activity Questionnaire. a Adjusted for age, sex, race/ethnicity, and baseline health status. b Risk ratio not computed because no patients selected alcohol referral programs within program. c P = .19; 2-sample test of proportions. Quit smoking 25.0 (80) 21.5 (79) 1.16 (0.64–1.90) 0.92 (0.45–1.64) Quit risky drinkingb 33.3 (3) 14.2 (28) — — Eating >5 servings fruit and vegetables per day 16.1 (62) 11.1 (198) 1.45 (0.71–2.71) 1.91 (0.82–3.81) Activity >low 25.0 (16) 37.5 (40) 0.67 (0.22–1.47) 0.63 (0.14–1.60) Any behavior change 21.7 (161) 16.9 (343)c — —
Supplemental Tables 1-3; Supplemental Figure
Supplemental Table 1: Prevalence of Individual Risk Behaviors and Risk Behavior Clusters in Entire Sample, n = 864; Supplemental Table 2. Intervention Chosen by Patients With Multiple Behavioral Risks in the Intervention Arm; Supplemental Table 3. Themes and Illustrative Quotations From Interviews With 15 Medical Assistants; Supplemental Figure. Adoption of intervention by medical assistants at 6 primary care clinics.
Files in this Data Supplement:
- Supplemental data: Tables & Figure - PDF file, 4 pages, 144 KB
The Article in Brief
A Medical Assistant-Based Program to Promote Healthy Behaviors in Primary Care
Robert L. Ferrer , and colleagues
Background Most primary care patients have at least one of four major health risk behaviors: smoking, risky drinking, low physical activity, or unhealthy diet. This study sought to determine the effectiveness of a medical assistant-driven program to screen for the unhealthy behaviors, arrange appropriate interventions, and ultimately reduce unhealthy behaviors.
What This Study Found The medical assistant program was much more effective than usual care at linking patients with interventions, more than doubling the proportion of patients referred. Despite the process improvement, however, the program did not succeed in changing any of the four health behaviors.
Implications
- The study results underscore the difficulties in changing health behaviors.
- The authors call for more professional development for medical assistants taking on expanded roles, as well as further work in developing systems to support long-term improvements in patients� behaviors.
Annals Journal Club:
Nov/Dec 2009
Medical Assistants' Role in Improving Preventive and Chronic Illness Care
The Annals of Family Medicine encourages readers to develop the learning community of those seeking to improve health care and health through enhanced primary care. You can participate by conducting a RADICAL journal club, and sharing the results of your discussions in the Annals online discussion for the featured articles. RADICAL is an acronym for: Read, Ask, Discuss, Inquire, Collaborate, Act, and Learn. The word radical also indicates the need to engage diverse participants in thinking critically about important issues affecting primary care, and then acting on those discussions.1How it Works
In each issue, the Annals selects an article or articles and provides discussion tips and questions. We encourage you to take a RADICAL approach to these materials and to post a summary of your conversation in our online discussion. (Open the article online and click on "TRACK Comments: Submit a response.") You can find discussion questions and more information online at: http://www.AnnFamMed.org/AJC/.
CURRENT SELECTION
Articles for Discussion
- Ferrer RL, Mody-Bailey P, Jaen CR, Gott S, Araujo S. A medical assistant-based program to promote health behaviors in primary care. Ann Fam Med. 2009; 7 (6):504-512.
- Gensichen JS, Jaeger C, Peitz M, et al. Health care assistants in primary care depression management: role perception, burdening factors, and disease conception. Ann Fam Med. 2009; 7 (6):513-519.
Discussion Tips
Of the 417,000 medical assistants active in the United States in 2006, 62% worked in physician offices.2 Similar roles exist in other countries. Duties vary but typically are limited to medical care support functions. These 2 articles are relevant to efforts to improve the efficiency and effectiveness of team approaches to primary care by expanding the role of medical assistants. The articles present complementary but contrasting perspectives of chronic illness and preventive care, qualitative and quantitative methods, and US and German social and health care system contexts.Discussion Questions
- What questions are addressed by these articles? How do the questions fit with what already is known on this topic?
- What is the relevance of the research questions for the current economic, practice improvement, and health care system reform efforts?
- How strong are the study designs for answering the questions?
- To what degree can the findings be accounted for by:
- How participants were selected?
- How outcomes were measured?
- Confounding (false attribution of causality because 2 variables discovered to be associated actually are associated with a 3rd factor)?
- Researcher bias?
- Chance?
- What are the main findings?
- To what extent do the characteristics of the person performing the expanded role affect how well things work? What evidence do these articles give to support or refute your opinion?
- How comparable are the study populations to your practice? What is your judgment about the transportability of the findings?
- How (if at all) could these studies change your practice?
- What important researchable questions remain?
- What are the implications of the findings for practice improvement and health care reform?
References
- Stange KC, Miller WL, McLellan LA, et al. Annals journal club: It�s time to get RADICAL. Ann Fam Med. 2006;4(3):196-197. http://annfammed.org/cgi/content/full/4/3/196.
- Medical assistants. In: Occupational Outlook Handbook, 2008-09 Edition. Bureau of Labor Statistics. http://www.bls.gov/oco/ocos164.htm. Accessed Oct 14, 2009.




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Barriers and Facilitators to Expanding Roles of Medical Assistants in Patient-Centered Medical Homes (PCMHs)
- Patterns of Relating Between Physicians and Medical Assistants in Small Family Medicine Offices
- Impact of Peer Health Coaching on Glycemic Control in Low-Income Patients With Diabetes: A Randomized Controlled Trial
- The Role of the Champion in Primary Care Change Efforts: From the State Networks of Colorado Ambulatory Practices and Partners (SNOCAP)
- Improving Multiple Health Risk Behaviors in Primary Care: Lessons from the Prescription for Health COmmon Measures, Better Outcomes (COMBO) Study
- Coordination of Health Behavior Counseling in Primary Care
- Capability and Clinical Success
- Actionable Ideas to Improve Health Care and Health
- Annals Journal Club: Medical Assistants' Role in Improving Preventive and Chronic Illness Care
- In This Issue: Multifaceted Research