
Article Figures & Data
Figures
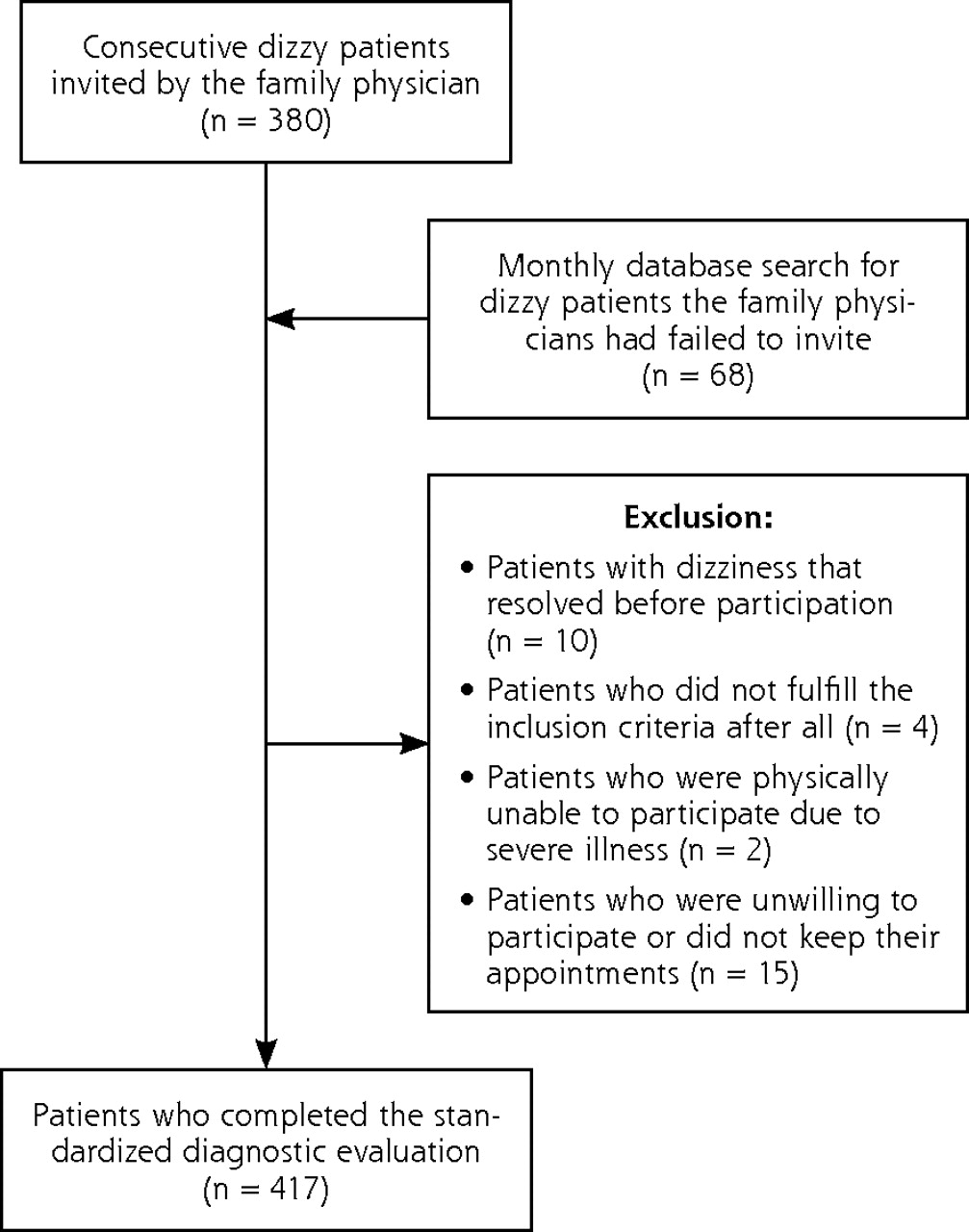
- Figure 1.
Flowchart of participants through the study.

Tables
Characteristic Value Sex, female, No. (%) 307 (74) Age, mean (range), y 78.5 (65–95) Living situation, No. (%) Alone 254 (61) Home for the elderly, or other institution 66 (16) Ethnic background, No. (%) Dutch native 342 (82) Western immigrant 31 (7) Non-Western immigrant 44 (11) Level of education, No. (%) Elementary school 119 (29) High school 247 (59) College/university 51 (12) Smoking, No. (%) 62 (15) Drugs, total. Drugs per patient, mean (SD), No. 4.4 (3.0) Polypharmacy (patients using >5 drugs), No. % 21 138 (33) Fall-risk–increasing drugs (FRID) 22 FRID per patient, mean (SD), No. 1.9 (1.5) Patients using ≥3 FRID, No. (%) 154 (37) Distribution of FRID, No. (%) Diuretics 149 (36) β-Blockers 128 (31) Calcium channel blockers 80 (19) Angiotensin receptor blockers 71 (17) Angiotensin converting enzyme inhibitors 67 (16) Anxiolytics/hypnotics 52 (12) Nitrates 51 (12) Hypoglycemics 48 (12) Antidepressants 35 (8) Antivertigo drugs 31 (7) Analgesics 25 (6) α-Blockers 21 (5) Neuroleptics 16 (4) Antiarrhythmics 15 (4) Digoxin 13 (3) Antihistamines 11 (3) Medical history Cardiovascular disease, No. (%) Hypertension 239 (57) Ischemic heart disease 111 (27) Arrhythmia 94 (23) Heart valve disease 58 (14) Myocardial infarction 57 (14) Ear, nose, and throat disease, No. (%) Benign paroxysmal positional dizziness 40 (10) Ménière’s disease 27 (6) Acoustic neuroma 1 (0.2) Neurological disease, No. (%) Migraine 79 (19) Cerebrovascular disease 66 (16) Parkinson disease 7 (2) Epilepsy 6 (1) Multiple sclerosis 1 (0.2) Locomotor disease, No. (%) Arthrosis of the knee (gonarthrosis) 120 (29) Arthrosis of the hip (coxarthrosis) 78 (19) Psychiatric illness, No. (%) Depressive disorder 101 (24) Anxiety disorder 75 (18) Other, No. (%) Cataract 199 (48) Diabetes 78 (19) Macular degeneration 27 (7) Characteristic No. % a Adds up to more than 100%, because more than 1 answer is possible. Descriptiona Instability or unsteadiness 287 69 Loss of balance 280 67 Light-headedness 248 59 Rotational sensation 228 55 Tendency to fall 226 54 Giddy 176 42 Environment spinning 137 33 Becoming unwell 115 28 Near faint 97 23 Everything turning black 68 16 Other dizziness 83 20 Onset 2–4 wk 30 7 1–6 mo 98 24 6–24 mo 110 26 2–10 y 120 29 >10 y 59 14 Duration of symptoms <10 sec 110 26 10–60 sec 78 19 Several minutes 71 17 Several minutes to 1 h 22 5 >1 h 35 8 Constant when present 26 6 Combination of above possibilities 75 18 Frequency Continuous 42 10 Daily 195 47 Weekly 105 25 Monthly 50 12 Annually 25 6 Provoking circumstancesa Getting up from a lying or sitting position 292 70 Bending forward 258 62 Turning head 223 53 Looking up 210 50 Exercise 140 34 Standing still 99 24 Strong emotions 82 20 Other 109 26 None 17 4 Associated symptomsa Falling/almost falling 207 50 Trouble with walking 184 44 Nausea 112 27 Sweaty, pale, or clammy 91 22 Fear 82 20 Dyspnea 48 12 Tinnitus 42 10 Palpitations 41 10 Chest pain 28 7 Diplopia 27 6 Hearing problems 24 6 Trouble with speaking or swallowing 12 3 Other 57 14 None 110 26 Chest pain 28 7 - Table 3.
Abnormal Findings During the Examination of 417 Dizzy Elderly Patients in Primary Care
Examination by System Findings No. % ODS = oculi dexter et sinister; PRIME-MD = Primary Care Evaluation of Mental Disorders. Note: For diagnostic criteria, see Supplemental Appendix 2, available at http://www.annfammed.org/cgi/content/full/8/3/196/DC1. a Not measured because of edema, severe obesity, or irregular pulse. b Not performed because of fear, pathology of neck or back, or other physical problems of the patient. c Unreliable test result because of suboptimal testing conditions during home visit. d An electrocardiogram was indicated if (1) a patient complained of presyncopal dizziness (a faint feeling, light-headedness, or a feeling of everything turning black), (2) palpitations were associated with dizziness, or (3) exercise provoked complaints of dizziness. e Continuous-loop event recording indicated if electrocardiogram did not show a clear explanation. f Questionnaire incomplete. Physical examination Cardiovascular system Pulse Bradycardia 23 6 Tachycardia 1 0 Irregular 50 12 Blood pressure Systolic blood pressure ≥160 mm Hg 198 48 Orthostatic hypotension test Positive, without reproduction of symptoms 43 10 Positive, with reproduction of symptoms 58 14 Unknowna 5 1 Auscultation of the heart Systolic/diastolic murmur without radiation 57 14 Systolic/diastolic murmur with radiation 48 12 Locomotor system Orthopedic screening Limited stability at rest 193 46 Limited stability during walking 177 42 Limited mobility hip(s) 152 37 Limited mobility knee(s) 105 25 Limited mobility ankle(s) 50 12 Tandem gait Tandem gait score ≥40 32 8 Not possible, because of lack of stability 115 28 The timed up-and-go test Abnormal (≥20 sec) 71 17 Not possible, because of lack of stability 3 1 Neurological system Tendon reflexes Abnormal patellar tendon reflex 89 21 Abnormal Achilles tendon reflex 68 16 Abnormal plantar responses 9 2 Semmes-Weinstein mono-filament test 25%–50% disturbed 65 16 50%–75% disturbed 62 15 >75% disturbed 80 19 Vestibular system Otoscopy Otitis media/externa 7 2 Perforated tympanic membrane 13 3 Deformities tympanic membrane/inner ear caused by trauma or surgery 7 2 Dix-Hallpike maneuver Positive 44 11 Unknownb 31 7 Remaining tests Corrected visual acuity Abnormal (ODS ≤0.5 [Snellen metric]) 120 29 Unknownc 31 7 Additional tests Cardiovascular system Electrocardiogram Atrial fibrillation (known) 13 3 Atrial fibrillation (new) 5 1 Bradycardia 7 2 Premature ventricular complexes in bigeminy 1 0 Tachycardia (>100/min) 1 0 Third-degree atrioventricular block 2 0 Not indicatedd 107 26 Continuous-loop event recording Bradycardia 1 0 Sick sinus 1 0 Tachycardia (>100/min) 2 0 Premature ending by the patient 3 1 Premature ending because of allergic response to electrodes 4 1 Premature ending for other medical reason(s) 3 1 Not registerede 357 86 Laboratory tests Hemoglobin Moderately severe anemia 5 1 Severe anemia 3 1 Nonfasting blood glucose Hyperglycemia 7 2 Psychiatric testing PRIME-MD Patient Health Questionnaire One or more of listed diagnoses 174 42 Major depressive disorder 53 13 Other depressive disorder 60 14 Panic disorder 19 5 Other anxiety disorder 42 10 Any somatoform disorder 89 21 Probable alcohol abuse/dependence 10 2 Any eating disorder 3 1 Unknown 2 0 Vestibular system Audiometry Abnormal audiogram both ears 199 48 Characteristic No. % Note: Data for each patient were independently reviewed by a family physician, a geriatrician, and a nursing home doctor. a Adds up to more than 100%, because more than 1 dizziness subtype per patient is possible. Dizziness subtypea Presyncope 288 69 Vertigo 171 41 Disequilibrium 166 40 Other dizziness 7 2 No consensus 16 4 Total 648 Number of dizziness subtypes per patient 1 217 52 2 137 33 3 47 11 No consensus 16 4 Total 417 100 Major Cause Minor Cause Totala Characteristic No. % No. % No. % Note: Data for each patient were independently reviewed by a family physician, a geriatrician, and a nursing home doctor. a Adds up to more than 100%, because more than 1 cause of dizziness per patient is possible. Contributing causes Adverse drug effect 10 2 96 23 106 25 Cardiovascular disease (including cerebrovascular disease) 237 57 66 16 303 73 Locomotor disease 15 4 43 10 58 14 Metabolic or endocrine conditions 3 1 3 1 6 1 Neurological disease (excluding cerebrovascular disease) 12 3 36 9 48 12 Psychiatric illness 41 10 40 10 81 19 Peripheral vestibular disease 60 14 40 10 100 24 Impaired vision 2 0 3 1 5 1 Other causes 3 1 4 1 7 2 Unclear 34 8 – – 34 8 Total 417 100 331 79 748 179 Contributing causes per patient 1 126 30 2 191 46 3 59 14 4 6 1 5 1 0 Unclear 34 8 Total 417 100
Supplemental Appendixes
Supplemental Appendix 1. Search Strategy Used in Electronic Databases for Identifying Dizzy Patients Family Physicians Had Failed to Invite (15 Search Terms and 3 ICPC Codes); Supplemental Appendix 2. Diagnostic Criteria During the Evaluation of Dizzy Elderly Patients; Supplemental Appendix 3. Score Form Used by the Reviewers
Files in this Data Supplement:
- Supplemental data: Appendix 1 -3 - PDF file, 4 pages, 130 KB
The Article in Brief
Causes of Persistent Dizziness in Elderly Patients in Primary Care
Otto R. Maarsingh , and colleagues
Background Although dizzy patients are usually seen in primary care settings, most diagnostic studies of dizziness have been performed in secondary or tertiary care settings. This study assesses causes and types of dizziness in elderly primary care patients.
What This Study Found Cardiovascular disease was the most common major cause of dizziness, followed by peripheral vestibular disease and psychiatric illness. The most common minor contributory cause of dizziness was an adverse drug effect. In a large proportion of patients, there was more than one cause of dizziness.
Implications
- Primary care clinicians should consider multiple causes when treating dizzy patients.
Annals Journal Club:
May/Jun 2010
Causes of Dizziness in the Elderly
The Annals of Family Medicine encourages readers to develop a learning community of those seeking to improve health care and health through enhanced primary care. You can participate by conducting a RADICAL journal club and sharing the results of your discussions in the Annals online discussion for the featured articles. RADICAL is an acronym for Read, Ask, Discuss, Inquire, Collaborate, Act, and Learn. The word radical also indicates the need to engage diverse participants in thinking critically about important issues affecting primary care and then acting on those discussions.1How it Works
In each issue, the Annals selects an article or articles and provides discussion tips and questions. We encourage you to take a RADICAL approach to these materials and to post a summary of your conversation in our online discussion. (Open the article online and click on "TRACK Comments: Submit a response.") You can find discussion questions and more information online at: http://www.AnnFamMed.org/AJC/.
CURRENT SELECTION
Article for Discussion
- Maarsingh OR, Dros J, Schellevis FG, et al. Causes of persistent dizziness in elderly patients in primary care. Ann Fam Med. 2010; 8(3):196-205.
Discussion Tips
This article provides an opportunity to consider the causes of a common symptom among elderly patients seen in primary care.Discussion Questions
- What question(s) are addressed by this article?
- Why is this study needed beyond previous research on this topic?
- How strong is the study design for answering the question?
- To what degree can the findings be accounted for by:
- How physicians and their patients were selected or excluded?
- How the main variables were measured?
- Confounding (false attribution of causality because 2 variables discovered to be associated actually are associated with a third factor)?
- Chance?
- How strong are the methods for linking participating patients� dizziness and the cause to which it was attributed?
- How much does the Delphi procedure used to develop the evaluation protocol enhance your judgment of the appropriateness and completeness of the protocol?
- What are the main study findings?
- How does the sensitivity analysis aid your interpretation of the findings?
- How comparable is the study sample to your practice? What is your judgment about the transportability of the findings?
- How might this study change your practice?
- What important researchable questions remain?
References
- Stange KC, Miller WL, McLellan LA, et al. Annals journal club: It�s time to get RADICAL. Ann Fam Med. 2006;4(3):196-197. http://annfammed.org/cgi/content/full/4/3/196.




{kind=link}
Jump to section
Related Articles
Cited By...
- Prospective diagnostic accuracy study of history taking and physical examination for adults with vertigo in general practice: study protocol
- Prognosis and Survival of Older Patients With Dizziness in Primary Care: A 10-Year Prospective Cohort Study
- Working-age adults perspectives on living with persistent postural-perceptual dizziness: a qualitative exploratory study
- Predicting an Unfavorable Course of Dizziness in Older Patients
- Guided and unguided internet-based vestibular rehabilitation versus usual care for dizzy adults of 50 years and older: a protocol for a three-armed randomised trial
- Authors reply to Seemungal and Bolland and colleagues
- Effects of Nonpharmacological Interventions for Dizziness in Older People: Systematic Review
- Looks vestibular: irrational prescribing of antivertiginous drugs for older dizzy patients in general practice
- Annals Journal Club: Causes of Dizziness in the Elderly
- In This Issue: The Nourishment and Support of Family Medicine