
Article Figures & Data
Figures
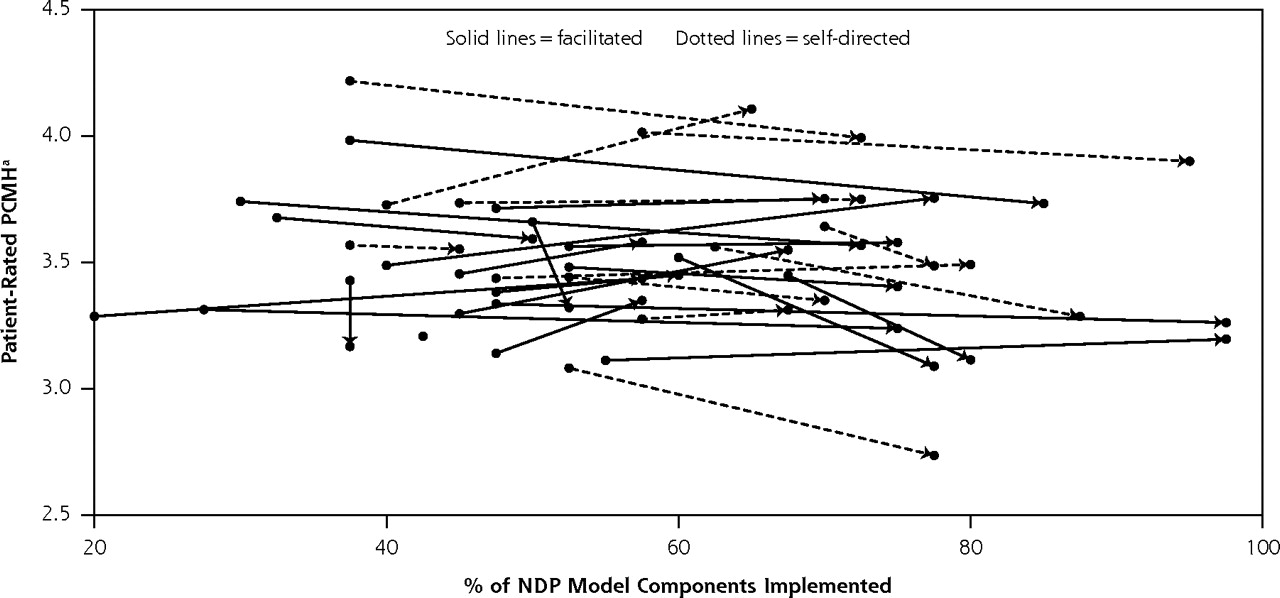
- Figure 1.
Composite score of patient-rated attributes vs NDP model components implemented at baseline and 26 months.
NDP=National Demonstration Project; arrow origin=baseline; arrow termination=26 months.
Notes: Each line represents 1 practice. The scale for the composite score for patient-rated primary care attributes ranged from 1 to 5, with higher scores indicating a higher level of attributes.
a Nutting PA, Crabtree BF, Stewart EE, et al. Effect of facilitation on practice outcomes in the National Demonstration Project model of the patient-centered medical home. Ann Fam Med. 2010;8(Suppl 1):s33–s44.16
Tables
NDP=National Demonstration Project; HR=human resources. Access to care and information (6 components) Same-day appointments Laboratory results highly accessible Online patient services e-Visits Group visits After-hours access coverage Care management (4 components) Population management Wellness promotion Disease prevention Patient engagement/education Practice services (5 components) Comprehensive acute and chronic care Prevention screening Surgical procedures Ancillary therapeutic/support Ancillary diagnostic services Continuity of care (5 components) Community-based services Hospital care Behavioral health care Maternity care Case management Practice management (5 components) Disciplined financial management Cost-benefit decision making Revenue enhancement Personnel/HR management Optimized office design Quality and safety (5 components) Medication management Patient satisfaction feedback Clinical outcomes analysis Quality improvement Practice-based team care Health information technology (5 components) Electronic medical record Electronic prescribing Population management/registry Practice Web site Patient portal Practice-based care (4 components) Provider leadership Shared mission and vision Effective communication Task designation by skill set Measure and Scale Description ACES = Ambulatory Care Experiences Survey; ACES-SF = Ambulatory Care Experiences Survey–Short Form; ACGME = American Council for Graduate Medical Education; ACQA = Ambulatory Care Quality Alliance; CARE = consultation and relational empathy; CPCI = Components of Primary Care Index; HbA1c=hemoglobin A1c; LDL=low-density lipoprotein; N/A=not applicable; PEI=Patient Enablement Index. a Data collected by self-administered patient questionnaires. b Data collected by medical record audits. Patient-rated outcomesa Access to first-contact care (ACES; range, 0–1.0) Help as soon as needed for an illness or injury; appointment for a checkup or routine care as soon as needed; answer to medical question the same day when calling during regular office hours; help or advice needed when calling after regular office hours Coordination of care (CPCI; range, 0–1.0) Keeps track of all my health care; follows up on a problem I’ve had, either at the next visit or by mail, e-mail, or telephone; follows up on my visit to other health care professionals; helps me interpret my laboratory tests, x-rays, or visits to other doctors; communicates with other health professionals I see Comprehensive care (CPCI; range, 0–1.0) Handles emergencies; care of almost any medical problem I may have; go for help with a personal or medical problem; go for care for an ongoing medical problem such as high blood pressure; go for a checkup to prevent illness Personal relationship over time (CPCI; range, 0–1.0) Knows a lot about my family medical history; have been through a lot together; understands what is important to me regarding my health; knows my medical history very well; takes my beliefs and wishes into account in caring for me; knows whether or not I exercise, eat right, smoke, or drink alcohol; knows me well as a person (such as hobbies, job, etc) Global practice experience (range, 0–1.0) (all or none) Strongly agree with: “I receive the care I want and need when and how I want and need it,” and strongly agree with: “I am delighted with this practice.” Self-reported health status (range, 1–5) In general how would you rate your overall health status? (excellent, very good, good, fair, poor) Patient empowerment (range, 0–2.0) Patient enablement (PEI; range, 0–1.0): In relation to your most recent visit, are you: able to cope with life; able to understand your illness; able to cope with your illness; able to keep yourself healthy; confident about your health; able to help yourself? (response options for each: much better, better, same or less, N/A) Consultation and relational empathy measure (CARE; range, 0–1.0): For your last doctor’s visit, how was the doctor at: making you feel at ease; letting you tell your “story”; really listening; being interested in you as a whole person; fully understanding your concerns; showing care and compassion; being positive; explaining things clearly; helping you take control; and making a plan of action with you? (response options for each: excellent, very good, good, fair, poor, N/A) Satisfaction with service relationship (range, 0–3.0) Physician satisfaction (ACES-SF; range, 0–2.0): rating of personal physician (0 = worst, 10 = best); recommend personal physician to family and friends (5 = definitely yes, 1=definitely not) Cultural responsiveness (ACGME; range, 0–1.0): the practice looks down on me and the way I live my life; the practice treats me with respect and dignity; the practice would provide better care if I were of a different race (for each, 5 = strongly agree, 1 = strongly disagree) Condition-specific outcomesb ACQA Starter Set measure (16 measures) 7 prevention measures: breast cancer screening, colon cancer screening, cervical cancer screening, tobacco use history, advice for smoking cessation, seasonal influenza vaccination, and pneumonia vaccination 2 coronary artery disease measures: prescription of lipid-lowering medications, prescription of aspirin prophylaxis 6 diabetes measures: HbA1c measurement, HbA1c under control, blood pressure at target, lipid measurement, LDL cholesterol at target, retinal examination up to date 1 acute care measure: appropriate use of antibiotics in children for upper respiratory tract infections Prevention score (percentage of eligible patients meeting recommendations) US Preventive Services Task Force recommendations by age and sex as of July 2006 Chronic disease care score (range, 0–1.0) Percentage of patients having a diagnosis of diabetes, hypertension, coronary artery disease, and hyperlipidemia receiving recommended treatments and assessments 8 diabetes measures: LDL cholesterol measured in previous year, LDL cholesterol <100 mg/dL, retinal examination by eye professional in previous year, HbA1c measured in the previous year, HbA1c <9%, last blood pressure <130/80 mm Hg, foot examination in the previous year, aspirin prophylaxis 2 hypertension measures: blood pressure at target (<140/90 mm Hg if nondiabetic, <130/80 mm Hg if diabetic), on aspirin prophylaxis 3 coronary artery disease measures: blood pressure at target, aspirin prophylaxis, on lipid-lowering therapy 4 hyperlipidemia measures: on lipid-lowering therapy, LDL at target (<100 mg/dL for diabetic patients and <130 mg/dL for nondiabetic patients), blood pressure at target, on aspirin prophylaxis - Table 3.
Characteristics of Patients Completing Questionnaires and Patients Whose Records Were Reviewed, by Group and Time Point
Baseline 26 Months Characteristic Facilitated Self-Directed Facilitated Self-Directed GED=general equivalency diploma. Patient questionnaires n=568 n=499 n=377 n=383 Age, mean (SD), y 55 (20.7) 49 (21.2) 56 (20.7) 52 (18.5) Women, No. (%) 374 (67) 334 (68) 264 (71) 263 (71) Race, No. (%) White/Caucasian 525 (95) 449 (95) 348 (95) 345 (95) Black/African American 17 (3) 7 (2) 10 (3) 7 (2) Other 11 (2) 19 (4) 7 (2) 12 (3) Ethnicity, No. (%) Hispanic or Latino 13 (3) 17 (4) 9 (3) 13 (4) Highest educational grade completed, No. (%) Less than high school graduation 67 (12) 65 (14) 44 (12) 34 (9) High school graduate or GED 129 (24) 119 (25) 102 (28) 77 (21) Some college or 2-year degree 166 (31) 142 (30) 122 (33) 118 (33) 4-year college graduate 83 (15) 71 (15) 50 (14) 60 (17) More than 4 years of college 96 (18) 81 (17) 50 (14) 72 (20) Employment status, No. (%) Employed 240 (45) 220 (48) 137 (37) 172 (47) Unemployed 6 (1) 4 (1) 6 (2) 7 (2) In school 35 (7) 39 (8) 20 (5) 15 (4) Disabled 25 (5) 22 (5) 17 (5) 14 (4) Looking after home 39 (7) 51 (11) 28 (8) 44 (12) Retired 158 (30) 102 (22) 139 (38) 96 (26) Other 29 (6) 24 (5) 21 (6) 16 (4) With practice ≤10 years, No. (%) 395 (72) 389 (80) 251 (67) 304 (80) Medical record audit n = 960 n = 1,023 n = 963 n = 898 Age, mean (SD), y 50 (58) 44 (23) 45 (23) 41 (23) Women, No. (%) 555 (58) 623 (62) 580 (61) 551 (61) Patient-Rated Outcomes Condition-Specific Outcomesa Group and Time Point, and P Values Access to Care Care Coordination Comprehensive Care Personal Relationship Over Time Global Practice Experienceb Service Relationship Satisfaction Patient Empowerment Self-Rated Health Status ACQA,c% Prevention,d% Chronic Care,e % ACQA = Ambulatory Care Quality Alliance; ANOVA = analysis of variance. Notes: Values in bold meet the study’s definition for a trend (P <.15). Analysis was performed using a generalized full factorial analysis of variance (ANOVA). a Composite score, represents overall percentage of all eligible reviewed care events that met criteria. b Composite score, all or none. c For the 16 measures assessed. d Percentage of age- and sex-specific recommendations of the US Preventive Services Task Force (July 2006) that were met. e Percentage of recommended measures met for diabetes mellitus, hypertension, hyperlipidemia, and coronary artery disease. f Change from baseline to 26-month time point. g Indicates whether there is significant change over time regardless of group. h Indicates whether there are significant group differences regardless of time. i Indicates whether there is significant differential change over time between the groups. Facilitated (n=15) Baseline .88 .76 .82 .76 .28 .91 .67 .66 39.8 36.8 53.4 9 months .88 .76 .82 .77 .29 .91 .68 .69 46.0 37.0 52.4 26 months .86 .75 .81 .76 .26 .90 .69 .68 48.1 41.1 58.7 Changef −.02 −.01 −.01 −.00 −.02 −.01 +.02 +.02 +8.3 +4.3 +5.2 Self-directed (n=14) Baseline .87 .75 .84 .76 .32 .91 .67 .68 35.9 40.5 42.3 9 months .86 .73 .82 .74 .32 .89 .67 .68 39.7 39.2 46.6 26 months .86 .73 .81 .75 .33 .90 .69 .70 45.0 39.8 47.3 Changef −.01 −.02 −.03 −.01 +.01 −.01 +.02 +.02 +9.1 −0.7 +5.0 P values Within groupg .11 .11 .06 .38 .92 .28 .19 .15 .000 .25 .002 Between grouph .64 .38 .70 .62 .34 .54 .96 .42 .20 .68 .003 Group by timei .71 .46 .25 .86 .31 .83 .93 .80 .85 .09 .92
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Differences in Diabetes Care With and Without Certification as a Medical Home
- Physicians' Response to Patients' Quality-of-Life Goals
- Quality of Cardiovascular Disease Care in Small Urban Practices
- A Randomized Trial of High-Value Change Using Practice Facilitation
- Are We Learning More about Patient-centered Medical Homes (PCMHs), or Learning More about Primary Care?
- Effects of Patient-centered Medical Home Transformation on Child Patient Experience
- Longitudinal evaluation of physician payment reform and team-based care for chronic disease management and prevention
- Primary Care Attributes Associated with Receipt of Preventive Care Services: A National Study
- The CardioMetabolic Health Alliance: Working Toward a New Care Model for the Metabolic Syndrome
- Making Personalized Health Care Even More Personalized: Insights From Activities of the IOM Genomics Roundtable
- More Extensive Implementation of the Chronic Care Model is Associated with Better Lipid Control in Diabetes
- Relationship Quality and Patient-Assessed Quality of Care in VA Primary Care Clinics: Development and Validation of the Work Relationships Scale
- Preventive Services Delivery in Patients With Chronic Illnesses: Parallel Opportunities Rather Than Competing Obligations
- Assessment and Measurement of Patient-Centered Medical Home Implementation: The BCBSM Experience
- Advanced Primary Care in San Antonio: Linking Practice and Community Strategies to Improve Health
- Medical Home Transformation: A Gradual Process and a Continuum of Attainment
- Correlation of the Care by Design™ Primary Care Practice Redesign Model and the Principles of the Patient-Centered Medical Home
- Enrolment in primary care networks: impact on outcomes and processes of care for patients with diabetes
- Systematic Review and Meta-Analysis of Practice Facilitation Within Primary Care Settings
- Can We Improve Adherence to Preventive Therapies for Cardiovascular Health?
- Small And Medium-Size Physician Practices Use Few Patient-Centered Medical Home Processes
- Patient-Centered Medical Home and Diabetes
- Implications of Reassigning Patients for the Medical Home: A Case Study