
Article Figures & Data
Figures
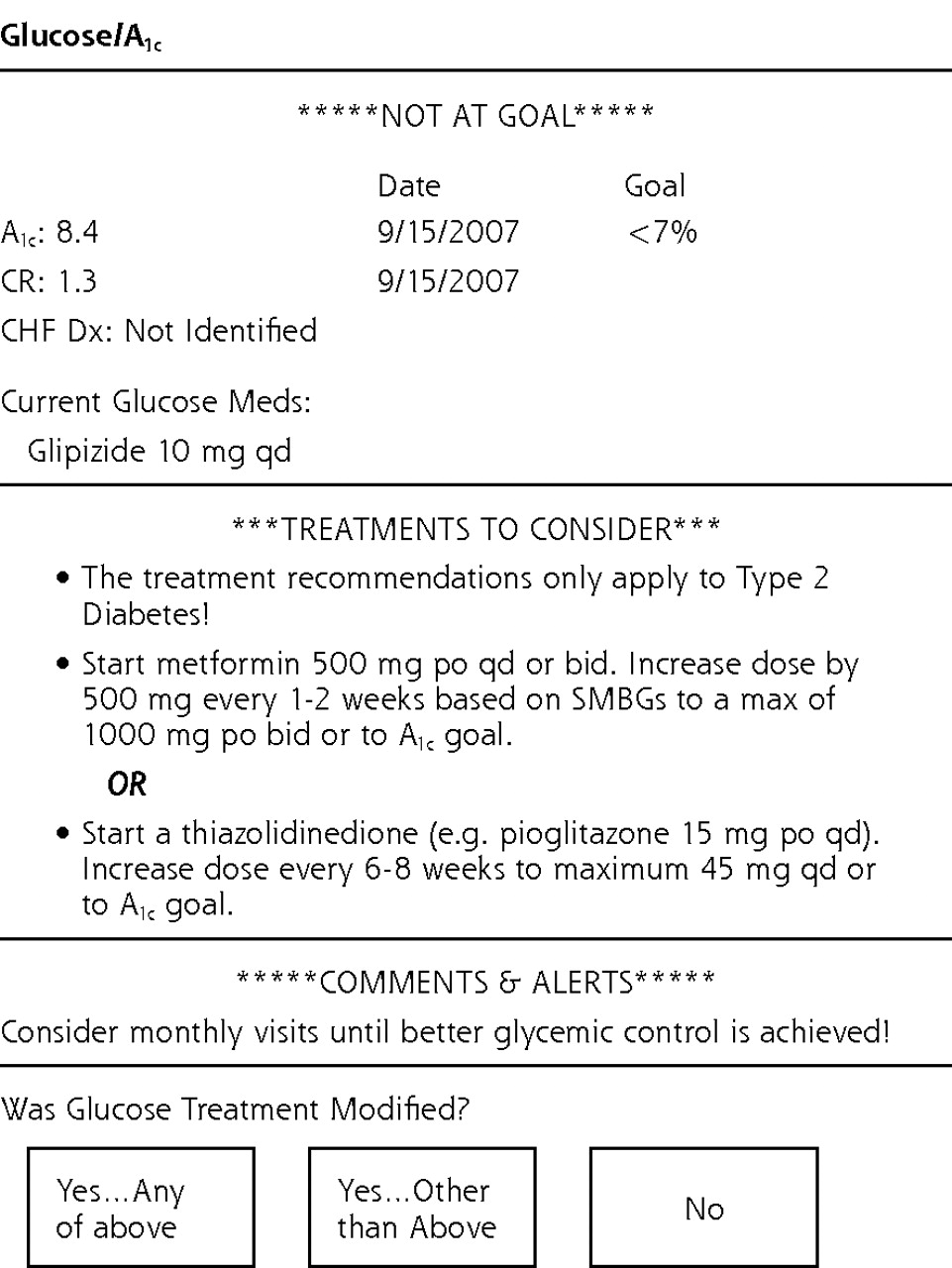
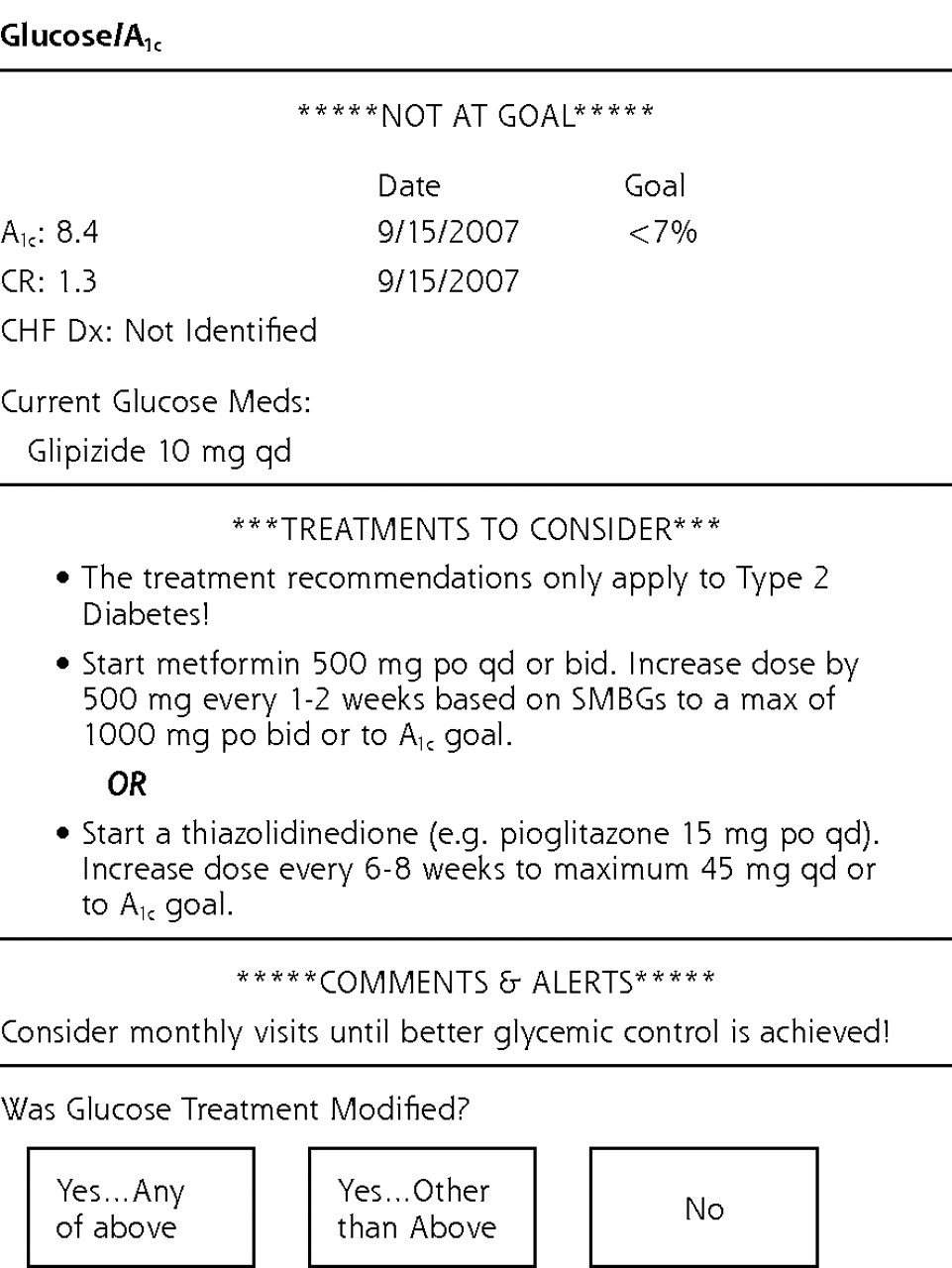
- Figure 1.
Example of Diabetes Wizard.
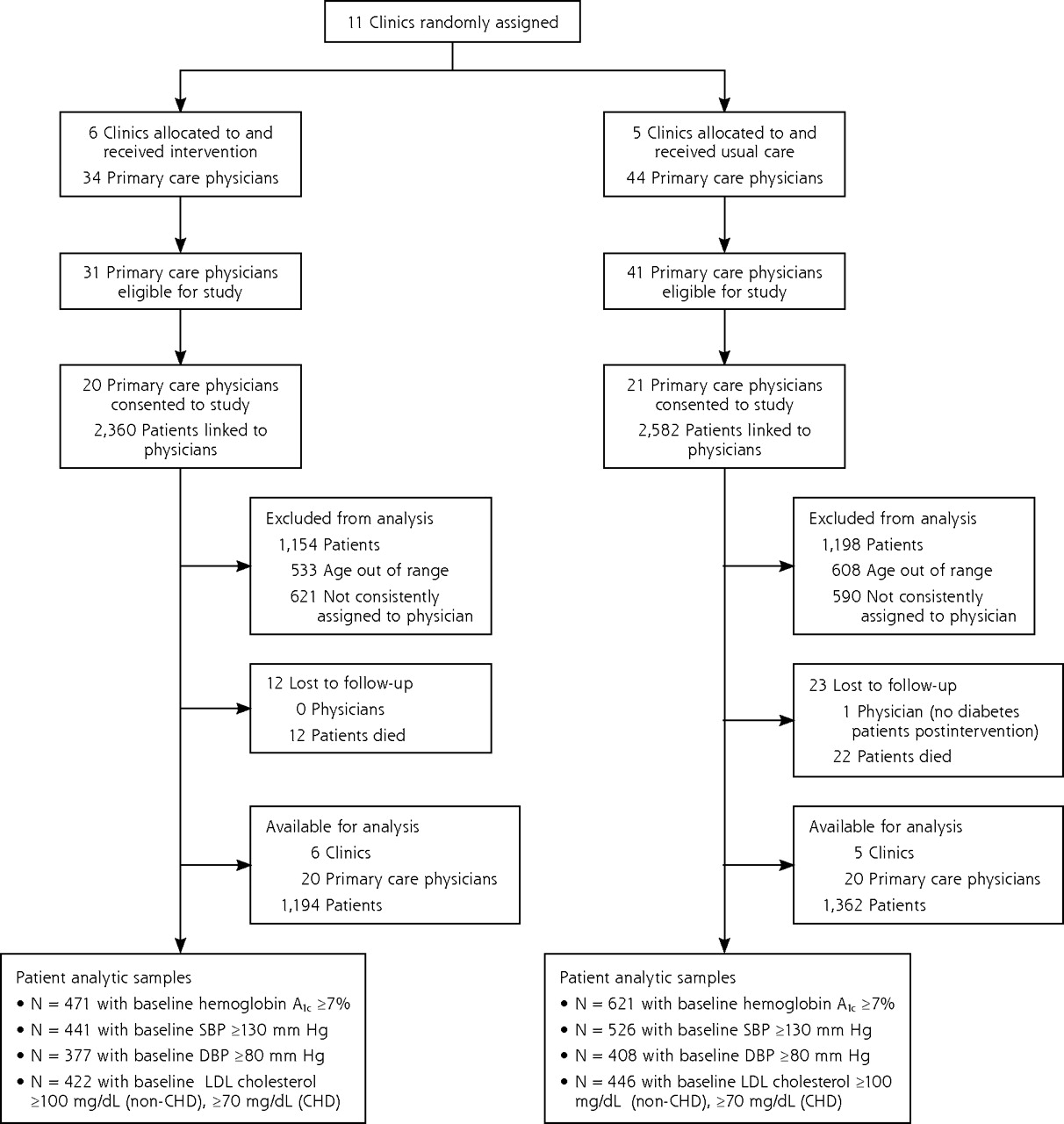
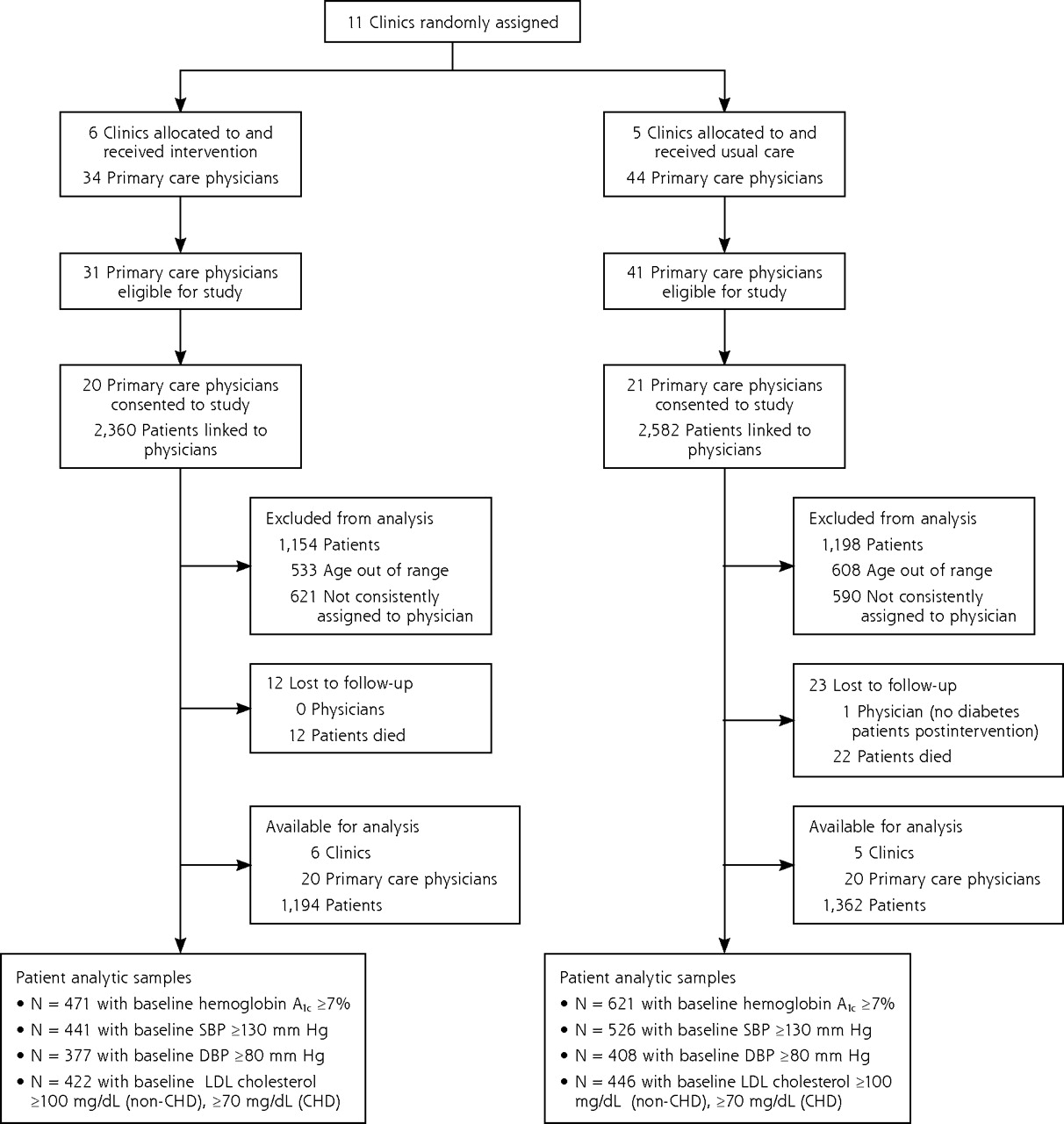
- Figure 2.
Diagram illustrating randomization and disposition of clinics, primary care physicians, and diabetes patients.
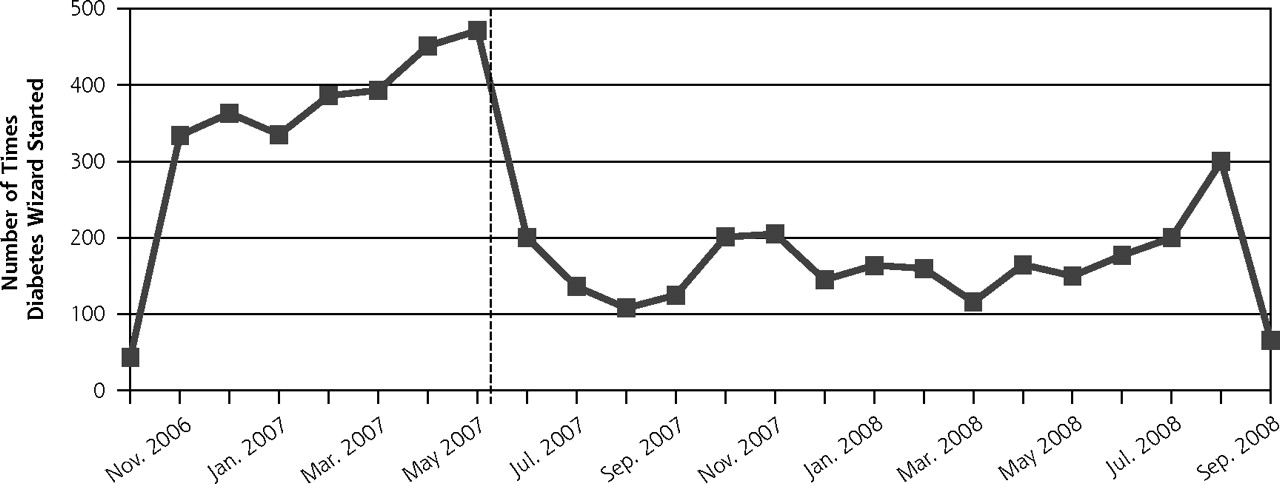
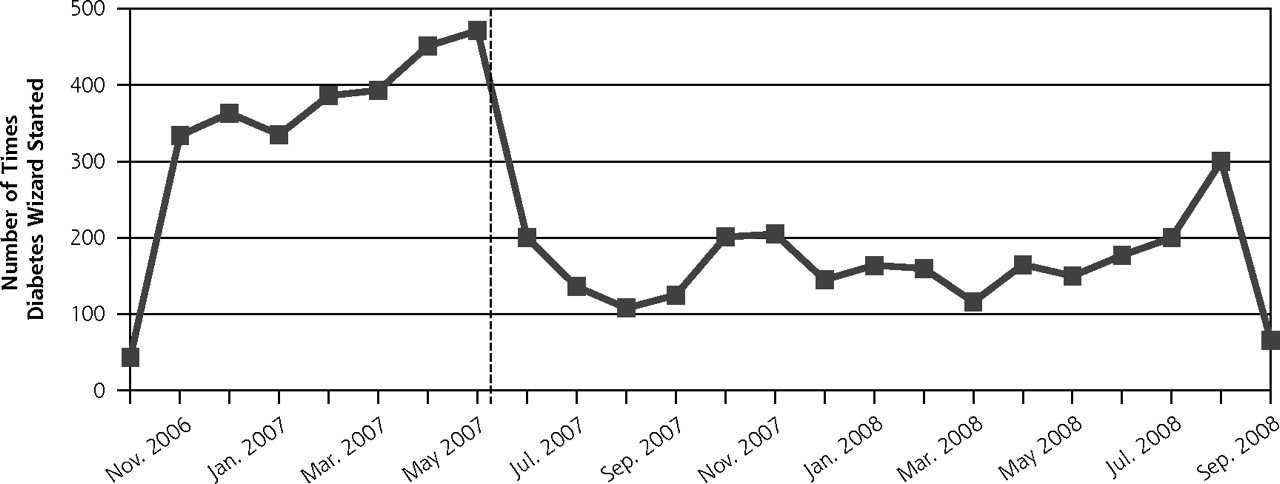
- Figure 3.
Diabetes Wizard use during and after intervention for the intervention group only.
Tables
- Table 1.
Characteristics of Study Physicians and Diabetes Patients Linked to Those Study Physicians at Intervention and Control Clinics
Variable Intervention Clinic Control Clinic P Valuea a P value derived from independent samples t test or Pearson χ2. Patients Total No. 1,194 1,362 Mean age (SD), y 57.0 (10.7) 57.5 (10.1) .23 Female, % 46.7 54.5 <.001 White race, % 82.8 70.6 <.001 Coronary heart disease preintervention, % 12.1 12.6 .75 Congestive heart failure preintervention, % 2.9 3.6 .35 Preintervention first glycated A1c, mean (SD) [median], % 7.4 (1.68) [7.0] 7.4 (1.67) [7.0] .47 Preintervention first systolic blood pressure, mean (SD) [median], mm Hg 127.3 (17.4) [126] 126.8 (17.1) [125] .40 Preintervention first diastolic blood pressure, mean (SD) [median], mm Hg 74.5 (10.9) [74] 73.5 (10.5) [74] .023 Preintervention first LDL cholesterol value, mean (SD) [median], mg/dL 99.4 (34.5) [94] 95.9 (33.8) [90] .019 Primary care physicians Total No. 20 20 Age, mean (SD), y 49.2 (9.9) 50.2 (7.3) .71 Family physician,% 80.0 45.0 .02 Female physician, % 55.0 50.0 .75 Diabetes patients per physician, mean (SD), No. 43.7 (17.3) 55.8 (30.2) .13 - Table 2.
Rates and Counts of Diabetes Encounters, Glycated Hemoglobin Tests, Low-Density Lipoprotein Cholesterol Tests, and Blood Pressure Measures, Comparing Intervention and Control Clinics in the Preintervention and Postintervention Periods
Intervention Clinic Control Clinic Variable Pre-intervention 12 mo Post-intervention 12 mo Change Pre-intervention 12 mo Post-intervention 12 mo Change Intervention Effecta P Valueb Hemoglobin A1c=glycated hemoglobin; CI=confidence interval; LDL = low-density lipoprotein. a The intervention effect column illustrates the differential amount of change in the intervention arm relative to the control arm comparing pre- with postintervention. b P value associated with the time × condition term in a generalized linear mixed model with repeated time measurements, study arm, and their interaction. c P <.001. d P <.01. e P <.05. Patients with 1 or more encounters or tests, proportion (95% CI) Diabetes encounters .850 (.820–.876) .949 (.932–.962) .099c .875 (.849–.897) .956 (.941–.967) .081c .018 .78 Hemoglobin A1c tests .829 (.788–.864) .940 (.919–.956) .112c .858 (.822–.888) .929 (.906–.947) .071c .041 .045 Blood pressure measurements .986 (.977–.991) .988 (.980–.993) .003 .986 (.978–.991) .981 (.971–.987) −.005 .008 .28 LDL cholesterol tests .819 (.779–.854) .871 (.838–.899) .052d .846 (.809–.876) .865 (.831–.892) .019 .033 .14 Encounters or tests done per patient, mean (95% CI), No. Diabetes encounters 3.9 (3.6–4.4) 4.5 (4.1–4.9) 0.49d 4.4 (4.1–4.8) 5.1 (4.7–5.5) 0.68c −0.20 .33 Hemoglobin A1c tests 2.0 (1.8–2.1) 2.4 (2.2–2.5) 0.41c 2.0 (1.8–2.2) 2.3 (2.2–2.5) 0.31c 0.11 .09 LDL tests 1.4 (1.2–1.5) 1.5 (1.4–1.7) 0.17d 1.4 (1.3–1.6) 1.5 (1.4–1.6) 0.08 0.09 .09 - Table 3.
Changes and Proportion of Adult Diabetes Patients at Goal on Glycated Hemoglobin, Blood Pressure, and LDL Cholesterol Measures Among Intervention and Control Group Primary Care Physicians and Clinics in the Preintervention (Baseline) and Postintervention Periods
Intervention Clinic Control Clinic Variable No. Baseline Post-intervention Change Baseline Post-intervention Change Intervention Effecta P Valueb DBP = diastolic blood pressure; hemoglobin A1c=glycated hemoglobin; LDL=low-density lipoprotein; SBP=systolic blood pressure; SE=standard error. a The intervention effect column illustrates the differential amount of change in the intervention arm relative to the control arm comparing before and after the intervention. b For mean value analysis, P value associated with the time × condition term in a general linear mixed model with repeated time measurements, study arm, and their interaction. For proportion at goal analysis, P value associated with study arm. c P <.001. Hemoglobin A1c, mean (SE), % 1,092 8.5 (0.09) 7.9 (0.09) −0.58c 8.4 (0.08) 8.1 (0.08) −0.32c −0.26 .01 Hemoglobin A1c <7%, % (SE) 1,144 78.4 (2.0) 79.2 (2.0) −0.8 .80 SBP, mean (SE), mm Hg 894 141.3 (0.70) 130.5 (0.70) −10.8c 141.6 (0.69) 131.5 (0.69) −10.1c −0.70 .56 SBP <130 mm Hg, % (SE) 1,506 80.2 (1.6) 75.1 (1.6) 5.1 .03 DBP, mean (SE), mm Hg 731 85.1 (0.52) 76.8 (0.52) −8.3c 84.6 (0.51) 77.1 (0.51) −7.5c −0.82 .38 DBP <80 mm Hg, % (SE) 1,669 85.6 (1.4) 81.7 (1.5) 3.9 .07 LDL cholesterol, mean (SE), mg/dL 868 122.3 (1.7) 97.9 (1.8) −24.4c 124.1 (1.7) 98.3 (1.8) −25.8c 1.37 .62 LDL cholesterol <100 mg/dL (or <70 mg/dL if heart disease), % (SE) 1,362 85.2 (1.6) 83.9 (1.5) 1.4 .53
The Article in Brief
Impact of Electronic Health Record Clinical Decision Support on Diabetes Care: A Randomized Trial
Patrick J. O'Connor , and colleagues
Background This study tests a diabetes decision support tool embedded in an electronic health record. The tool offers doctors drug-specific treatment suggestions based on the patient�s current treatment, clinical goals, other medical conditions, and kidney and liver functions.
What This Study Found Compared with patients in the control group, patients in the intervention group had significantly better hemoglobin A1c values, better maintenance of systolic blood pressure control, and borderline better maintenance of diastolic blood pressure control. Participating doctors were highly satisfied with the intervention, and many continued using the technology after the study ended.
Implications
- The authors conclude that, in the coming era of genomic medicine and personalized chronic disease care, clinical support decision strategies like the one tested in this trial, capable of simultaneously standardizing and personalizing clinical care, will become essential to effective primary care.




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Harnessing the power of clinical decision support systems: challenges and opportunities
- Does Clinical Decision Support Increase Appropriate Medication Prescribing for Cardiovascular Risk Reduction?
- A systematic review of ontology-based clinical decision support system rules: usage, management, and interoperability
- CONSORT extension for the reporting of randomised controlled trials conducted using cohorts and routinely collected data (CONSORT-ROUTINE): checklist with explanation and elaboration
- Benefits and harms of intensive glycemic control in patients with type 2 diabetes
- CM-SHARE: Development, Integration, and Adoption of an Electronic Health Record-Linked Digital Health Solution to Support Care for Diabetes in Primary Care
- Interventional study to improve diabetic guidelines adherence using mobile health (m-Health) technology in Lahore, Pakistan
- Strategies to Prioritize Clinical Options in Primary Care
- The breadth and burden of data collection in clinical practice
- Rebuttal: Do electronic medical records improve quality of care?: Yes
- Refutation : Les dossiers medicaux electroniques ameliorent-ils la qualite des soins?: Oui
- Horses and buggies have some advantages over cars, but no one is turning back
- An Internet-Based Diabetes Management Platform Improves Team Care and Outcomes in an Urban Latino Population
- Response to Comment on O'Connor et al. Randomized Trial of Telephone Outreach to Improve Medication Adherence and Metabolic Control in Adults With Diabetes. Diabetes Care 2014;37:3317-3324
- Randomized Trial of Telephone Outreach to Improve Medication Adherence and Metabolic Control in Adults With Diabetes
- Standards of Medical Care in Diabetes--2014
- Standards of Medical Care in Diabetes--2013
- Quality improvement collaboratives in the age of health informatics--new wine in new wineskins
- Validation of prescribing appropriateness criteria for older Australians using the RAND/UCLA appropriateness method
- Typical Electronic Health Record Use in Primary Care Practices and the Quality of Diabetes Care
- Standards of Medical Care in Diabetes--2012
- Consensus Report: Diabetes Performance Measures: Current Status and Future Directions
- Diabetes Performance Measures: Current Status and Future Directions
- Courage and Change
- In This Issue: Clinical Decision Support