
Article Figures & Data
Figures
- Figure 1.
Conceptual model of how tailored messages on family risk status and recommended preventive strategies would result in behavioral changes.
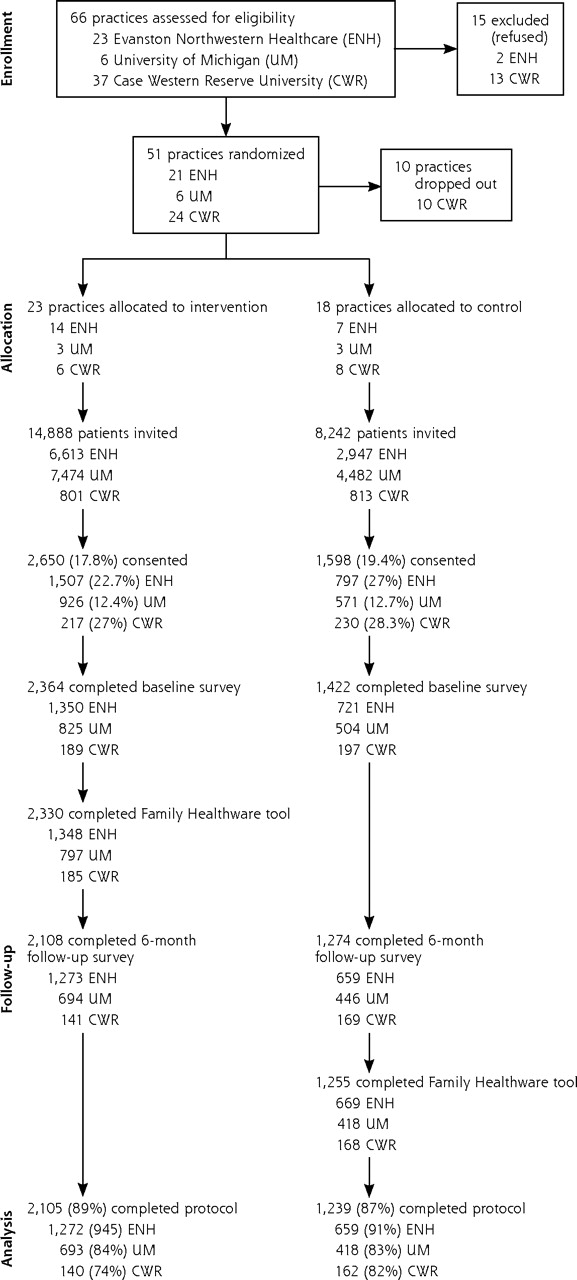
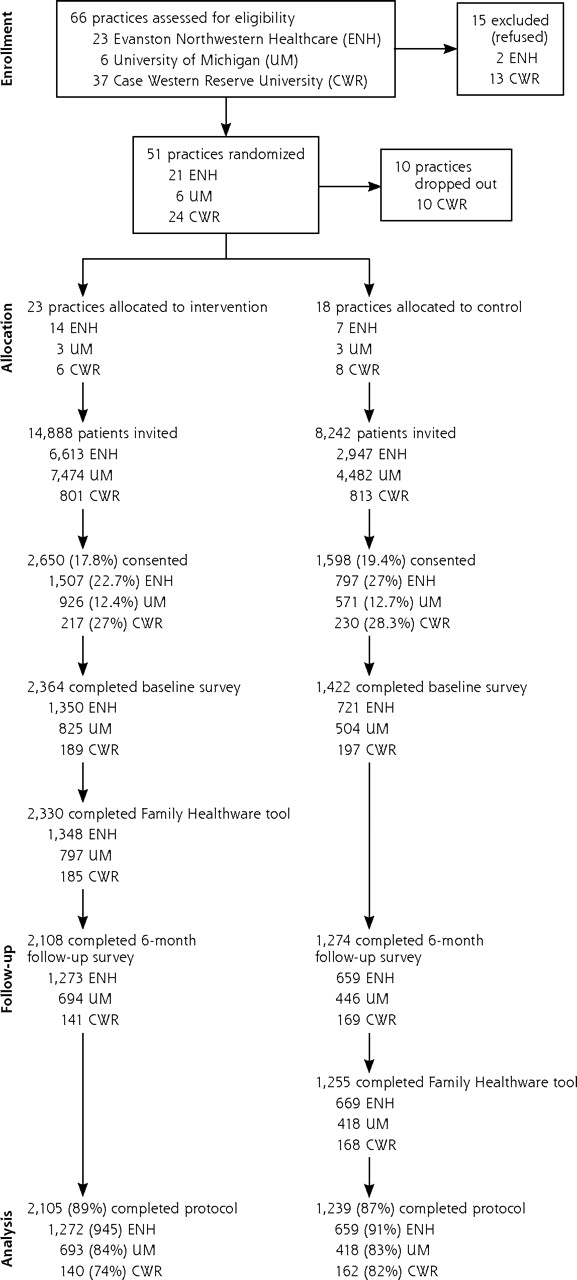
- Figure 2.
Consort diagram of practice and participant recruitment.

Tables
Characteristics Intervention Arm (n=2,364) No. (%) Control Arm (n=1,422) No. (%) Note: After adjusting for practice clustering and site differences, the only statistically significant difference between the study arms exists for starting season (P=.003). a Income for 12% was not reported in either group. Sex, female 1,676 (71) 962 (68) Age, mean (SD), y 50.3 (8.4) 51.1 (8.0) Hispanic or Latino 58 (2) 29 (2) Race White 2,134 (90) 1,320 (93) Black or African American 87 (4) 35 (3) Asian 70 (3) 31 (2) Other 42 (2) 20 (1) More than 1 race 31 (1) 16 (1) Marital status Single, never married 203 (9) 96 (7) Married or living with partner 1,857 (79) 1,135 (80) Separated or divorced 260 (11) 160 (12) Widowed 44 (2) 31 (2) Season study started January–April 1,179 (50) 411 (29) May–August 704 (30) 375 (26) September–December 481 (20) 636 (45) Annual household incomea Less than $25,000 91 (4) 41 (3) $25,001 to $35,000 102 (5) 45 (4) $35,001 to $50,000 218 (11) 106 (8) $50,001 to $75,000 402 (19) 228 (18) More than $75,000 1,262 (61) 834 (66) Currently has health insurance 2,276 (96) 1,380 (97) Intervention Arm (n = 2,330)aNo. (%) Control Arm (n = 1,255)aNo. (%) Risk Weak Moderate Strong Weak Moderate Strong a Sample size excludes participants without complete family history data. b P value <.05 is based on a comparison of proportions between study arms and adjusted for practice clustering and site differences. Coronary heart disease 947 (41) 615 (26) 768 (33) 502 (40) 323 (26) 430 (34) Stroke 1,212 (52) 783 (34) 335 (14) 640 (51) 419 (33) 196 (16) Diabetesb 1,426 (61) 643 (28) 261 (11) 812 (65) 302 (24) 141 (11) Colorectal cancer 2,015 (87) 263 (11) 52 (2) 1069 (85) 147 (12) 39 (3) Breast cancer 1,799 (77) 305 (13) 226 (10) 990 (79) 139 (11) 126 (10) Ovarian cancer 2,107 (91) 125 (5) 98 (4) 1135 (90) 73 (6) 47 (4) Characteristics Intervention Arm (n=2,364) No. (%) Control Arm (n=1,422) No. (%) Note: Comparison between study arms was carried out after adjusting for practice clustering and covarying effects of age, sex and study sites. a P<.05. Smoking Current 185 (8) 108 (8) Former 701 (30) 415 (29) Never 1,478 (62) 899 (63) Fruit and vegetable intake <2 servings a day 430 (18) 251 (18) 2–4 servings a day 1,546 (65) 939 (66) ≥5 servings a day 388 (17) 160 (16) Physical activity None to less than 10 min per week 82 (4) 56 (4) 1–4 times a week >10 min to <30 min each event 1,587 (69) 928 (67) 5–6 times a week at least for 30 min each event 620 (27) 397 (29) Aspirin use (<3 d/wk)a 1,608 (83) 851 (73) Blood pressure measured >1 y ago 191 (8) 99 (7) Cholesterol level measured >5 y ago 156 (7) 73 (5) Blood glucose level measured >2 y ago 794 (34) 427 (30) Behavior Change Groupsa Intervention ArmbNo. (%) Control Arm No. (%)b a The maintained category means the participants had the same behavior identified at baseline and month 6 based upon self-report. The increased category means the participants were not at goal at baseline and reported at goal for the specific behavior at month 6. b The sample size for each behavior does not equal the total study sample for each arm because of missing or incomplete data. c Subset of the study population used to determine whether the intervention was significantly more effective in moving participants to at goal compared with the control intervention. d For blood pressure measurement, the goal was to have had a blood pressure reading by physician within the last year. The category “Still no measurement within past year” reported no blood pressure measurement within a year of baseline and at month 6. The category “Measurement obtained” represents participants with no blood pressure measurement within a year at baseline but who reported a blood pressure measurement within a year at month 6. e For cholesterol, the goal was a cholesterol level measurement within the last 5 years. The category “Still no measurement in past 5 y” means no cholesterol level was measured within 5 years from baseline to month 6. The category “Measurement obtained” represents participants with no cholesterol level measurement within 5 years at baseline but who reported cholesterol level measurement within 5 years at month 6. f For blood glucose, the goal was a blood glucose level measurement within the last 2 years. The category “Still no measurement in past 2 y” means no blood glucose level measured within 2 years of baseline and month 6. The category “Measurement obtained” represents participants with no blood glucose level measurements within 2 years at baseline but who reported a blood glucose level measurement within 2 years at month 6. Smoking 2,110 1,278 Maintained smokingc 129 (6) 78 (6) Quit smokingc 26 (2) 17 (2) Maintained never or former 1,944 (92) 1,177 (92) Started smoking 11 (1) 6 (1) Fruit and vegetable intake 2,111 1,278 Maintained <5 servings a dayc 1,560 (74) 973 (76) Increased to >5 servings a dayc 193 (9) 89 (7) Maintained ≥5 servings a day 261 (12) 159 (12) Moved to <5 servings a day 97 (5) 57 (5) Physical activity 2,033 1,236 Maintained physical activity <5–6 times a week for <30 min each eventc 1,249 (62) 782 (63) Increased physical activity 5–6 times a week for ≥30 min each eventc 218 (11) 99 (8) Maintained 5–6 times a week for ≥30 min each event 412 (20) 240 (20) Decreased physical activity <5–6 times a week for <30 min each event 152 (7) 114 (9) Aspirin use 1,959 1,159 Maintained <3 d/wkc 1,458 (74) 775 (67) Increased to ≥3 d/wkc 150 (8) 76 (7) Maintained ≥3 d/wk 307 (16) 251 (22) Decreased to <3 d/wk 44 (2) 57 (5) Blood pressure measuredd 2,110 1,277 Still no measurement within past yearc 16 (1) 7 (1) Measurement obtainedc 147 (7) 78 (6) Measurement within 1 y for entire study 1,896 (90) 1,155 (91) Measurement no longer within 1 y 51 (2) 37 (3) Cholesterol level measurede 2,025 1,203 Still no measurement in past 5 yc 42 (2) 13 (1) Measurement obtainedc 51 (2) 31 (3) Measurement within 5 y for entire study 1,857 (92) 1,124 (93) Measurement lapsed 75 (4) 35 (3) Blood glucose level measuredf 1,726 1,034 Still no measurement in past 2 yc 103 (6) 54 (5) Measurement obtainedc 120 (7) 51 (5) Measurement within 2 y for entire study 1,466 (85) 906 (88) Measurement lapsed 37 (2) 23 (2) - Table 5.
Contrast of Movement From Not at Lifestyle Goal to at Goal Compared With Persistently Not at Goal for Each Behavior by Study Arm
Variable OR (95% CI)a CI=confidence interval; OR = odds ratio. a Odds ratio exhibits odds of the intervention group moving in a positive direction with reference to the control group. Logistic regression model is adjusted for practice clustering and site, baseline body mass index, sex, baseline smoking status (except for quit smoking variable), frequency of moderate/strong family risks, and risk perception score for the 6 diseases. Diet and physical activity variables were further adjusted for season in which questionnaires were filled out. b Model run without site adjustment. Quit smoking 1.18 (0.47–2.95) Increased to ≥5 serving of fruit and vegetables each day 1.29 (1.05–1.58) Increased physical activity to 5–6 times a week for ≥30 min each event 1.47 (1.08–1.98) Aspirin use increased to ≥3 d/wk 0.91 (0.64–1.29) Blood pressure measured by health care professional within the last yearb 1.44 (0.29–7.16) Blood cholesterol level measured within 5 y 0.34 (0.17–0.67) Blood glucose level measured within 2 y 1.08 (0.61–1.91)
Supplemental Appendixes
Supplemental Appendix 1. Family Healthware Health Messages and Recommendations;Supplemental Appendix 2. Standard Health Message. Family Healthware Study ControlHealth Messages and Recommendations
Files in this Data Supplement:
The Article in Brief
Effect of Preventive Messages Tailored to Family History on Health Behaviors: The Family Healthware Impact Trial
Mack T. Ruffin, IV , and colleagues
Background A new online tool helps primary care practices collect and use family history to help prevent disease. This study looks at whether patients who receive a risk assessment and messages tailored to their family health history of six diseases are more likely to change their lifestyle behaviors or get health screening, compared with patients who receive a generic preventive health message.
What This Study Found Using a Web-based tool to screen for family history and tailor prevention messages to family risk improves some health behaviors. Preventive messages tailored to family risk for coronary heart disease, stroke, diabetes, and colorectal, breast, and ovarian cancers modestly increases fruit and vegetable consumption and physical activity. Specifically, intervention participants were 3 percent more likely to increase daily fruit and vegetable consumption from 5 or fewer servings a day to 5 or more servings a day and 4 percent more likely to increase physical activity to five to six times a week for 30 minutes or more compared with patients receiving a generic preventive health message. The untailored (generic) message increased the percentage of patients getting a cholesterol screening.
Implications
- Familial risk may be an important motivator of health behavior change.
- Additional research is needed to determine how to effectively implement family history assessment in primary care.
Annals Journal Club:
Jan/Feb 2011
Symbiosis Instead of Competing Demands: A Tale of 2 Preventive Services
The Annals of Family Medicine encourages readers to develop a learning community of those seeking to improve health care and health through enhanced primary care. You can participate by conducting a RADICAL journal club and sharing the results of your discussions in the Annals online discussion for the featured articles. RADICAL is an acronym for Read, Ask, Discuss, Inquire, Collaborate, Act, and Learn. The word radical also indicates the need to engage diverse participants in thinking critically about important issues affecting primary care and then acting on those discussions.1How it Works
In each issue, the Annals selects an article or articles and provides discussion tips and questions. We encourage you to take a RADICAL approach to these materials and to post a summary of your conversation in our online discussion. (Open the article online and click on "TRACK Comments: Submit a response.") You can find discussion questions and more information online at: http://www.AnnFamMed.org/AJC/.
CURRENT SELECTION
Article for Discussion
- Ruffin MT IV, Nease DE Jr, Sen A, et al. Effect of preventive messages tailored to family history on health behaviors: the Family Healthware Impact Trial. Ann Fam Med. 2011;9(1):3-11.
Discussion Tips
This cluster-randomized clinical trial assesses the effect of an automated family medical history assessment and tailored messages on preventive behaviors compared with a standard preventive message. In addition to critiquing the study, consider its larger implications for the family focus of family practice and the emerging genetic revolution.Discussion Questions
- What question is addressed by the article? How does the question fit with what already is known on this topic?
- How does a conceptual model inform the intervention design and your interpretation of the results?
- How strong is the study design for answering the question?
- How do the study methods compare with the CONSORT criteria for clinical trials?2
- What is the degree to which can the findings be accounted for by:
- The choice of the comparison intervention?
- How participants (settings, practices, clinicians, and patients) were selected? The exclusion criteria and dropouts? Are any biases likely to be important?
- How outcomes were measured?
- Confounding (false attribution of causality because 2 variables discovered to be associated actually are associated with a 3rd factor)?
- How information was interpreted?
- Chance?
- What are the main findings? How large is the effect across different outcomes?
- How transportable are the findings to your clinical setting? What factors might affect this transportability?
- Could you apply these findings to your practice using MyFamilyHealth Portrait, at https://familyhistory.hhs.gov/fhh-web/home.action?
- What are the implications of the current limited utility of most electronic health records (EHRs) for gathering, synthesizing, analyzing and using family history information? Is the growing use of EHRs affecting the family focus of family practice? What is the potential for EHRs to support a family focus to care? How might this potential be realized? How could EHRs support primary care clinicians, patients, and families in managing the forthcoming onslaught of genetic/genomic information?
- What are some next steps for applying the findings or answering other questions that this study raises?
References
- Stange KC, Miller WL, McLellan LA, et al. Annals journal club: It�s time to get RADICAL. Ann Fam Med. 2006;4(3):196-197. http://annfammed.org/cgi/content/full/4/3/196.
- CONSORT Group. CONSORT: Consolidated Standards of Reporting Trials. http://www.consort-statement.org/. Accessed Dec 23, 2010.




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Development and Validation of Lifestyle-Based Models to Predict Incidence of the Most Common Potentially Preventable Cancers
- Assessing family history of chronic disease in primary care: Prevalence, documentation, and appropriate screening
- Physical Activity, Parental History of Premature Coronary Heart Disease, and Incident Atherosclerotic Cardiovascular Disease in the Atherosclerosis Risk in Communities (ARIC) Study
- Cancer Risk Assessment Tools in Primary Care: A Systematic Review of Randomized Controlled Trials
- Prompting Primary Care Providers about Increased Patient Risk As a Result of Family History: Does It Work?
- Communicating about family health history: heredity, culture, iatrogenesis and the public good
- A Randomized, Controlled Trial to Increase Discussion of Breast Cancer in Primary Care
- Development and Validation of a Family History Screening Questionnaire in Australian Primary Care
- Development and evaluation of a brief self-completed family history screening tool for common chronic disease prevention in primary care
- In This Issue: From Apprehension to Action
- Courage and Change
- In This Issue: Clinical Decision Support
- Annals Journal Club: Symbiosis Instead of Competing Demands: A Tale of 2 Preventive Services