
Article Figures & Data
Figures
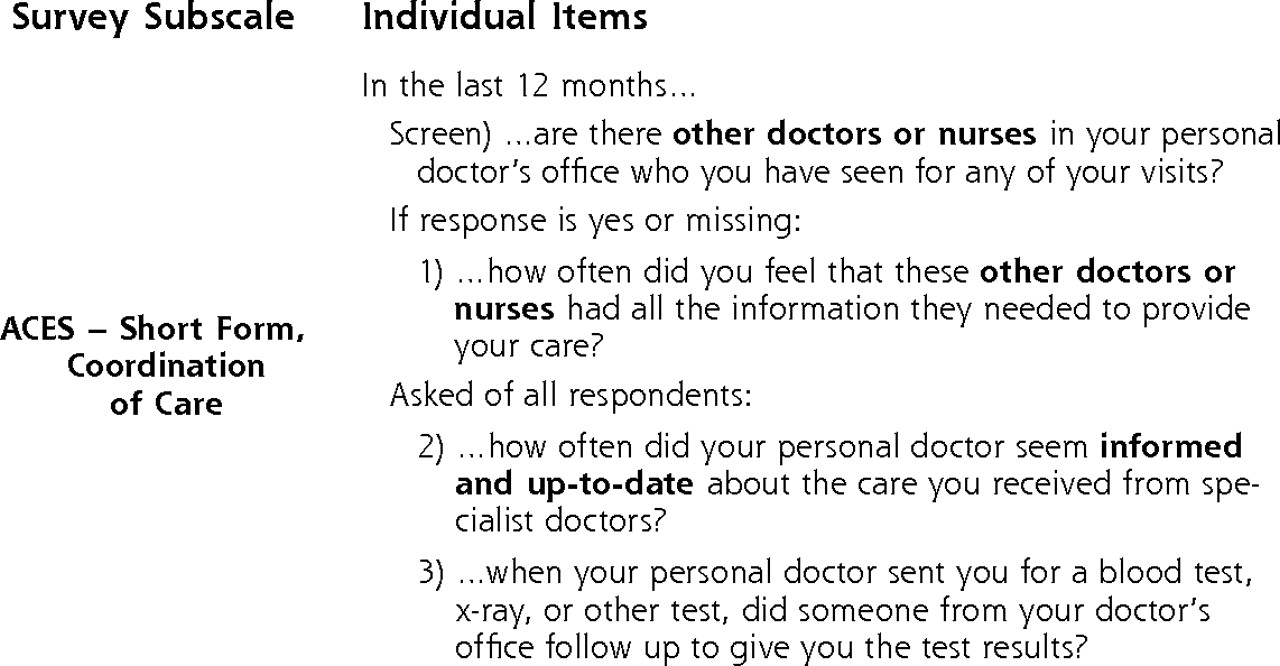
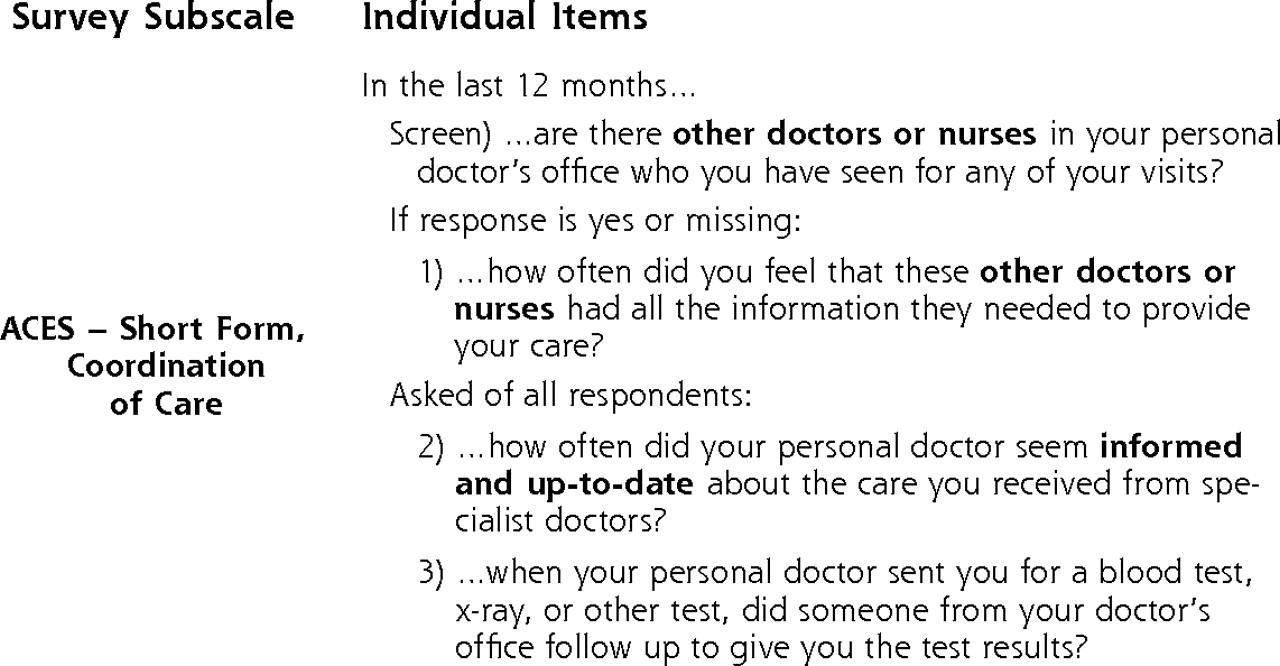
- Figure 1.
Ambulatory Care Experiences Survey (ACES) measure of care coordination.
Tables
Specialty Care Use (No. of Visits)a Characteristics Low (0–9) n (%) High (10+) n (%) Total, N (%) Coordination Score Mean (SD)b CAD = coronary artery disease; RxRisk = medication-based risk adjustment measure.36 a χ2 Test compared percentages between low and high specialty care use groups. b One-way analysis of variance compared mean coordination across covariate groups. c P <.01. d P <.001. Total 1,552 (76) 499 (24) c 2,051 (100) 77.7 (21) d Sex Female 910 (59) 259 (52) 1,169 (57) 76.2 (22) Male 642 (41) 240 (48) d 882 (43) 79.6 (19) c Race White 1,312 (85) 461 (93) 1,773 (87) 78.2 (20) Nonwhite 231 (15) 35 (7) 266 (13) 74.1 (23) Age, y 65–69 158 (10) 43 (8) 201 (10) 75.3 (22) 70–74 243 (16) 68 (14) 311 (15) 77.7 (20) 75–79 330 (21) 121 (24) 451 (22) 79.5 (20) 80–84 379 (24) 128 (26) 507 (25) 77.0 (21) 85+ 442 (29) 139 (28) d 581 (28) 77.7 (21) Chronic disease CAD only 564 (36) 231 (46) 795 (39) 77.2 (21) Diabetes only 697 (45) 132 (27) 829 (40) 78.5 (21) Both CAD and diabetes 291 (19) 136 (27) d 427 (21) 77.1 (21) d Self-rated health Excellent/very good 321 (21) 75 (16) 396 (20) 82.6 (19) Good 669 (44) 195 (40) 864 (43) 78.2 (20) Fair/poor 519 (35) 213 (44) d 732 (37) 74.4 (22) RxRisk Low 539 (35) 125 (25) 664 (33) 77.4 (21) Medium 549 (35) 148 (30) 697 (34) 77.9 (21) High 460 (30) 222 (45) d 682 (33) 77.8 (20) Any hospitalizations Yes 305 (20) 252 (51) 557 (27) 76.4 (21) No 1,247 (80) 247 (49) 1,494 (73) 78.2 (21) Variables Difference in Mean Coordination (95% CI) PValue CAD = coronary artery disease; RxRisk = medication-based risk adjustment measure.36 a Excluding 77 respondents because of missing race, self-rated health, or primary care physician data. b Interpretation: mean predicted change in coordination associated with increase of 1 SD (mean continuity=0.55; SD=0.32). Independent, unadjusteda Continuity, raw score/SDb 2.22 (1.3 to 3.1) <.001 High specialty care use 0.57 (−1.5 to 2.6) .59 Independent, adjusteda Continuity, raw score/SDb 2.21 (1.2 to 3.2) <.001 High specialty care use 1.23 (−1.0 to 3.4) .27 Covariates Female −2.71 (−4.3 to −1.1) .001 White 3.97 (1.3 to 6.7) .004 Age (referent: 65–69), y .03 70–74 3.63 (−0.1 to 7.4) 75–79 5.46 (1.6 to 9.3) 80–84 2.89 (−1.0 to 6.8) 85+ 4.67 (1.0 to 8.3) Chronic disease (referent: CAD) .27 Diabetes 1.96 (−0.4 to 4.4) Both CAD and diabetes 1.08 (−1.7 to 3.8) Self-rated health (referent: good) <.001 Excellent/very good 4.55 (2.1 to 7.0) Fair/poor −3.42 (−5.4 to −1.5) RxRisk score (referent: medium) .53 Low −1.21 (−3.5 to 1.1) High 0.03 (−2.3 to 2.4) Any hospitalizations −1.64 (−3.6 to 0.4) .11 - Table 3.
Association Between Coordination and Continuity According to Level of Specialty Care Use
Independent Variables (Adjusted)a,b Difference in Mean Coordination (95% CI) PValue CAD = coronary artery disease; RxRisk = medication-based risk adjustment measure.36 a Adjusted for sex, race (nonwhite, white), age (65–69, 70–74, 75–79, 80–84, 85+ years), chronic disease (CAD, diabetes, both), self-rated health (excellent/very good, good, fair/poor), RxRisk (low, medium, high), hospital admissions (no, yes). b Excluded 77 respondents because of missing race, self-rated health, or primary care physician data. c Interpretation: mean predicted change in coordination associated with increase of 1 SD. Continuity in low specialty care users, raw score (SD)c 2.71 (1.6 to 3.8) <.001 Continuity in high specialty care users, raw score (SD)c 0.28 (−1.6 to 2.2) .77
The Article in Brief
Patient-Reported Care Coordination: Associations With Primary Care Continuity and Specialty Care Use
David T. Liss , and colleagues
Background There is a growing need to coordinate medical care between primary care clinicians and specialists, patients, payers, and professional organizations. This study investigates the association between primary care continuity (the concentration of visits to primary care clinicians) and coordination by primary care clinicians.
What This Study Found When elderly patients with chronic conditions receive large amounts of outpatient specialty care, the ability of primary care clinicians to coordinate care in the traditional office setting seems to diminish. Analyzing data on 2,051 Medicare enrollees with select chronic conditions, researchers find a positive association between continuity and coordination for patients with low levels of specialty care use, but not for patients who utilize specialty care at high levels.
Implications
- Coordinating care for an aging population with high levels of specialty care use entails additional work for primary care practices and strains their ability to effectively coordinate patient care.
- The authors call for new methods of care provision that preempt gaps in continuity and coordination that may result from high specialty use.




{kind=link}
Jump to section
Related Articles
Cited By...
- Identifying patterns of health care utilisation among physical elder abuse victims using Medicare data and legally adjudicated cases: protocol for case-control study using data linkage and machine learning
- What does integrated care mean from an older persons perspective? A scoping review
- Regional Variation in Primary Care Involvement at the End of Life
- Effect of Continuity of Care on Hospital Utilization for Seniors With Multiple Medical Conditions in an Integrated Health Care System
- Validation of 2 New Measures of Continuity of Care Based on Year-to-Year Follow-up With Known Providers of Health Care
- Priming Primary Care Physicians to Treat Osteoporosis After a Fragility Fracture: An Integrated Multidisciplinary Approach
- In This Issue: Technology and Primary Care