
Abstract
PURPOSE Nonspecific abdominal pain (NSAP) is a common complaint in childhood. In specialist care, childhood NSAP is considered to be a complex and time-consuming problem, and parents are hard to reassure. Little is known about NSAP in family practice, but the impression is that family physicians consider it to be a benign syndrome needing little more than reassurance. This discrepancy calls for a better understanding of NSAP in family practice.
METHODS Data were obtained from the Second Dutch National Survey of General Practice (2001). Using registration data of 91 family practices, we identified children aged 4 to 17 years with NSAP. We calculated the incidence, and we studied factors associated with childhood NSAP, referrals, and prescriptions.
RESULTS The incidence of NSAP was 25.0 (95% confidence interval [CI], 23.7–26.3) per 1,000 person years. Most children (92.7%) with newly diagnosed NSAP (N = 1,480) consulted their doctor for this condition once or twice. Factors independently associated with NSAP were female sex (odds ratio [OR] = 1.4; 95% CI, 1.3–1.5), nongastrointestinal-nonspecific somatic symptoms (OR = 1.3; 95% CI, 1.1–1.5), and health care use (OR = 1.04; 95% CI, 1.03–1.05). When NSAP was diagnosed at the first visit, 3% of the patients were referred to specialist care, and 1% received additional testing. Family physicians prescribed medication in 21.3% of the visits for NSAP.
CONCLUSIONS Childhood NSAP is a common problem in family practice. Most patients visit their doctor once or twice for this problem. Family physicians use little additional testing and make few referrals in their management of childhood NSAP. Despite the lack of evidence for effectiveness, family physicians commonly prescribe medication for NSAP.
INTRODUCTION
Abdominal pain is a common complaint in children worldwide.1 Although its effect on a child’s well-being is considerable, and it leads to substantial school absenteeism,2 childhood abdominal pain is usually not associated with organic disease.3,4 In this study, we use the expression nonspecific abdominal pain (NSAP) for abdominal pain for which the physician does not suspect an organic pathologic cause. Most studies on NSAP are carried out in specialist care and include children with chronic or recurrent abdominal pain.
Little is known about childhood NSAP in family practice. In population and school-based studies, the prevalence of NSAP ranges from 4% to 10%.1 The occurrence of NSAP in family practice has hardly been studied, nor has family physicians’ management. The impression is that family physicians consider NSAP in children to be a benign disorder needing little more than reassurance of parent and child. This view, however, contradicts the presence of psychological comorbidity,5–8 other nonspecific somatic symptoms,5,7,9 and the high prevalence of prolonged symptoms11 found in children referred to secondary and tertiary care. In specialist care, childhood NSAP is considered to be a complex and time-consuming problem, and parents of children with NSAP are found to be hard to reassure.11,12 For pediatric gastroenterologists NSAP is the most common disorder seen.13 The discrepancy between childhood NSAP described in specialist care and that described in primary care is challenging and calls for a better understanding of this condition in family practice.
The aim of our study was to offer a primary care perspective to childhood NSAP. Using registration data from the Second Dutch National Survey of General Practice, we performed an explorative study estimating the occurrence of childhood NSAP, studying associated factors and determining family physicians’ management.
METHODS
In the Netherlands, all inhabitants are registered with a family physician. A family practice is highly accessible, and the care is free. The family physician usually knows the family well. Access to a medical specialist is possible only after referral by a family physician.
The data used in the present study were derived from the Second Dutch National Survey of General Practice (DNSGP-2, conducted in 2001),14 which was designed to study morbidity in Dutch family practice. A total of 195 family physicians in 104 practices recorded for 12 consecutive months data from 394,192 registered patients (a representative 2.5% sample of the Dutch population). The study was carried out according to the Dutch legislation on privacy. All patient contacts, all referrals, and all prescriptions were registered in the patients’ electronic health records (EHRs). Morbidity was coded using the International Classification of Primary Care (ICPC),15 and prescriptions were coded according to the Anatomical Therapeutic Chemical index.17
Detailed information about the study design and methods has been reported previously.14,17 To enhance consistent and complete coding, family physicians were additionally trained in coding, and the electronic patient record–based morbidity recording systems were improved with software modules that alerted the user whenever registration was insufficient.17 The accuracy of coding was studied in a vignette study at the start of the registration period.18 The overall agreement among 161 participating family physicians and 4 ICPC coding experts for 30 written patient cases was 81%, and agreement for a written patient case about nonorganic abdominal pain (ICPC code D01, generalized abdominal pain) was 85%.18 The level of agreement indicates that the validity and consistency of coding diagnoses was adequate. Consistency and completeness of registration were checked during the data-cleaning procedure17; data from 13 practices were excluded because of poor quality of the registered data (8 practices) and because of failure to register referrals (5 practices).18
In the DNSGP-2, visits for the same health problem were clustered into 1 disease episode.16 The ICPC code of the last visit within an episode was considered to be the episode diagnosis and coded as such. For example, a patient with an episode that consisted of 2 visits for abdominal pain, in which the first visit was coded as other localized abdominal pain (D06), and the second as appendicitis (D88), the episode diagnosis was coded as appendicitis (D88) in both visits.
Study Population
To be eligible for this analysis, a child had to aged between 4 and 17 years. Age was determined at the middle of the registration year. All visits within episodes with a diagnosis of generalized abdominal pain (D01), other localized abdominal pain (D06), and irritable bowel syndrome (D93) were considered NSAP. Family physicians use these codes when they are not aware of any disorder causing the pain. A child’s health problem was considered an incident case if the first visit for NSAP during the registration year was coded as a new problem and a prevalent case if the first visit was coded as a known problem.
Factors Associated With Childhood Nonspecific Abdominal Pain
Children were labeled as having a psychological problem, a social problem, or a nongastrointestinal-nonspecific symptom whenever they had made 1 or more visits coded with a corresponding ICPC code. For a psychological problem we used ICPC chapter P (psychological and psychiatric problems: for example, P01 for feeling anxious, P02 for transient stress reaction, P03 for feeling down). For a social problem we used ICPC chapter Z (social problems: for example, Z20 for relationship problems with parents, Z21 and Z23 for problems with disease or death of parents/family, Z24 for problems with friends, Z25 for problems with assault or violence). We considered the following codes as nongastrointestinal-nonspecific somatic symptoms: N01 for headache, pain, A01 for general/ multiple sites, A04 for general weakness/tiredness, A06 for fainting/syncope, and A11 for chest pain not otherwise specified.
Management by Family Physicians
First, the percentage of prescriptions and referrals during visits for NSAP was compared with percentage of prescriptions and referrals during visits for other problems. Second, we analyzed additional testing, kind of referrals, and type of prescriptions in consecutive visits for NSAP of incident cases. All referrals were analyzed. Referrals could be coded to the following mental health care specialists: social worker, physiotherapist, primary care psychologist, psychotherapist, and psychiatrist.
Analyses
The incidence rate was calculated by dividing the total number of newly diagnosed cases (numerator) by the total number of person years of the population at risk (denominator). The number of person years was calculated by using the mid-time population. As the registration period was 1 year, the mid-time population was calculated by taking the mean of the number of listed patients at the beginning of the registration period and the number of listed patients at the end of the registration. Incidence rates were expressed per 1,000 person-years. The 95% confidence intervals (CIs) were computed around incidence rates assuming a Poisson distribution using Stata 11.0 (StataCorp LP, College Station, Texas). The prevalence rate was calculated with the total number of children with a visit for NSAP as numerator. We stratified the incidence rate for boys and girls by year of age.
We compared children who had NSAP with children who did not have NSAP (aged 4 to 17 years) with respect to age; sex; the number of children with psychological, social, and nongastrointestinal-nonspecific symptoms; and health care use. Health care use was calculated as the number of visits for reasons other than NSAP per child per year. Using univariate logistic regression analyses, we assessed the association between the above-enumerated factors and NSAP. Factors that during univariate analysis were significantly associated with NSAP (P <.05) were entered into a multivariate logistic regression analysis. The statistical package SPSS 15.0 was used for these regression analyses (SPSS Inc, Chicago, Illinois).
RESULTS
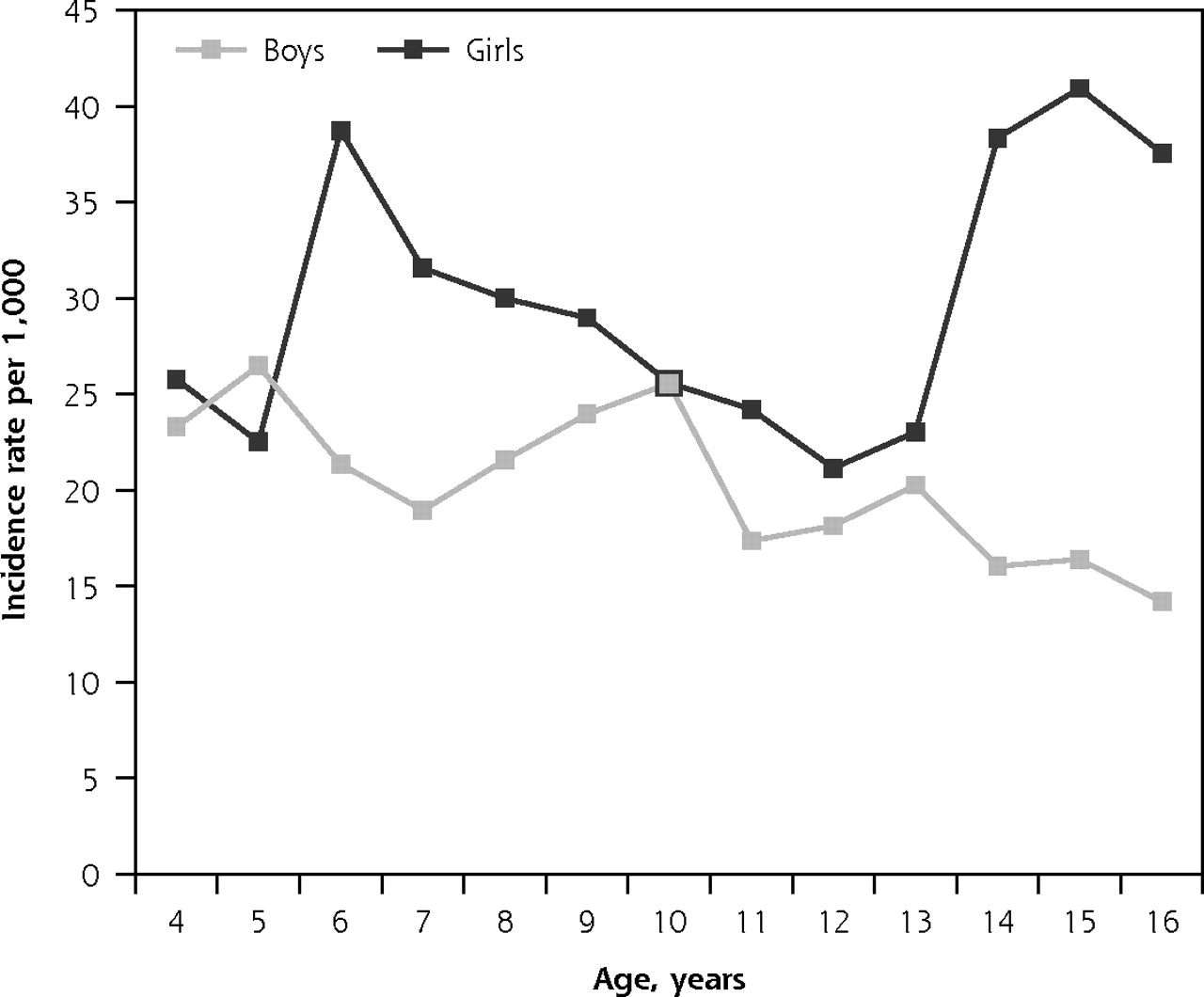
At the beginning of the registration year our study population consisted of 59,999 children aged 4 to 17 years, yielding 59,203 person-years. During the registration year 40,781 children (68.0%) consulted their family physician (range per practice, 129–1,486, median: 349), and 1,978 children did so for NSAP (4.9% of all consulting children). The control group consisted of 38,803 children. In total, 1,480 children consulted their family physician for the first time with NSAP. Table 1⇓ shows the incidence and prevalence rates for NSAP in girls and boys. Of the incident cases 1,372 (92.7%) patients consulted only once or twice for NSAP. Figure 1⇓ shows that the incidence rate for girls peaked around 6 years and again around 15 years. The incidence rate for boys decreased by age.
Childhood Cases of Nonspecific Abdominal Pain per 1,000 Person Years
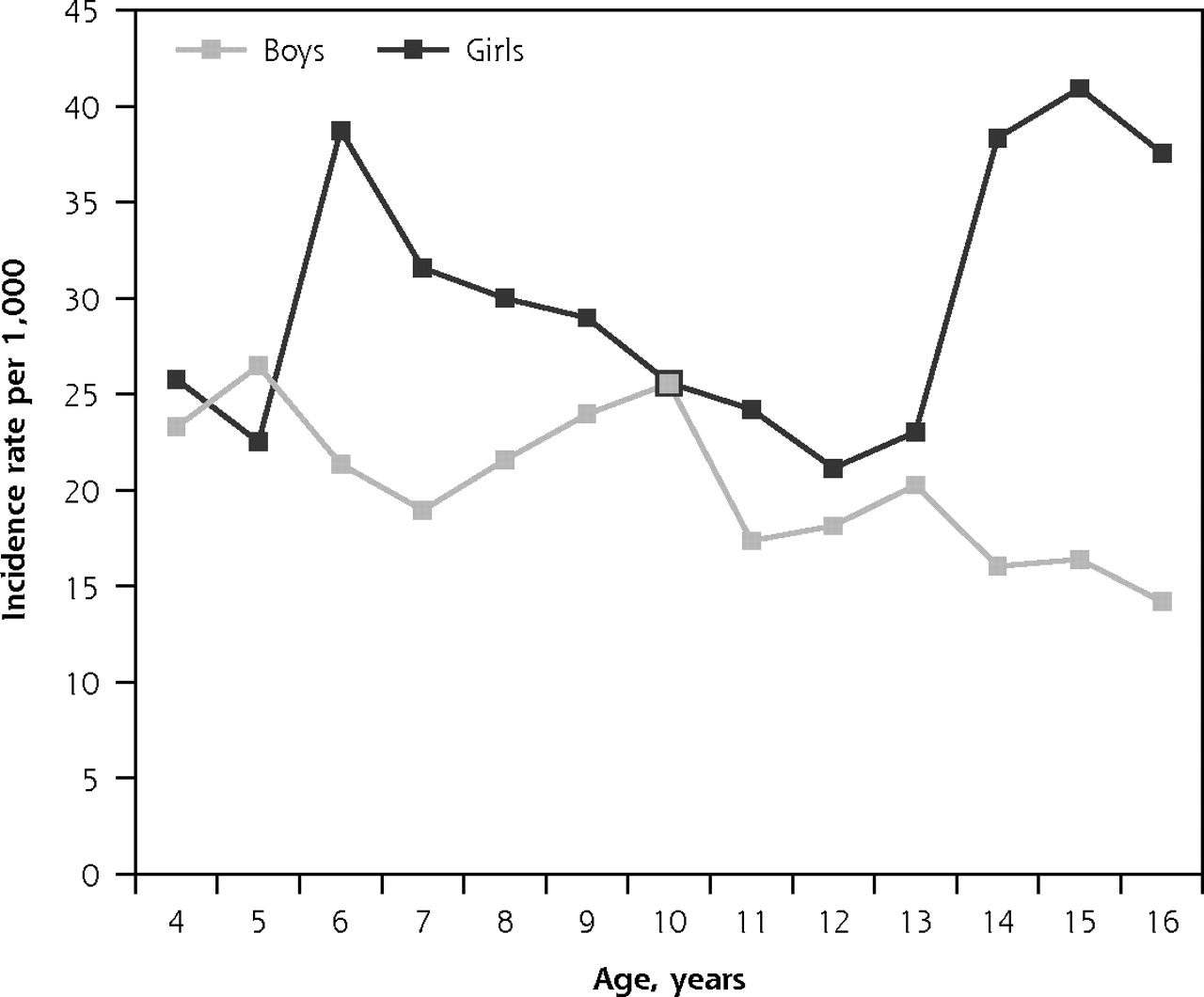
Incidence of nonspecific abdominal pain in children ages 4 to 17 years by sex in family practice.
Factors Associated With Nonspecific Abdominal Pain
Children with NSAP were more often girls, consulted more for psychological and social problems and nongastrointestinal-nonspecific somatic symptoms, and had more visits for other reasons (Table 2⇓). In the multivariate analysis female sex, health care use, and nongastrointestinal-nonspecific somatic symptoms were independently associated with NSAP.
Characteristics Associated With Childhood Nonspecific Abdominal Pain
Management by Family Physicians
Family physicians referred in 5.0% of the visits for NSAP. This percentage was comparable to that with visits for other problems (5.1%; Table 3⇓). During the first visit of new patients, family physicians referred 3.0% to secondary care and ordered additional testing for 1.1% of these patients (n = 16; Table 4⇓). The percentage of visits with a referral increased during the second visit to 5.6%, but decreased again and stabilized during the third and subsequent visits (2.7%). Most children who were referred were so at their first visit (cumulative percentage, 65.2%). During the first visit 39.3% of the referred children were referred to a surgeon (n = 24); in later visits most of the children were referred to a pediatrician. Only 1 child was referred to a psychiatrist.
Family Physician Management of Nonspecific Abdominal Pain in Children
Family Physicians’ Management During Consecutive Visits for Incident Cases of Nonspecific Abdominal Pain
In 21.3% of the visits for NSAP, family physicians prescribed medication at a rate that was significantly less than they prescribed medications in visits for other reasons (45.3%, P <.001) (Table 4⇑). During subsequent visits for NSAP, the prescription rate increased (from 17.6% to 40.8%). Approximately one-third of the total number of prescriptions were laxatives, (25.0% to 37.3%) and another one-third were antispasmodics (24.0% to 29.2%). Family physicians did not prescribe antidepressants or benzodiazepine derivatives for NSAP.
DISCUSSION
With an incidence rate of 25.0 per 1,000 person years (95% CI, 23.7–26.3) NSAP is one of the 10 most commonly seen complaints of children in Dutch family practice.15 Annually, a Dutch family physician with a practice of average size will see approximately 21 children aged 4 to 17 years with NSAP. Only a few (less than 7%) new patients with NSAP consult more than twice for this problem. In the present study, female sex, health care use, and other nongastrointestinal-nonspecific somatic symptoms were independently associated with NSAP. Family physicians referred in 5.0% of the visits for NSAP and prescribed medication in 21.3%.
The results of the present study show that childhood NSAP is a common problem in family practice. It is therefore remarkable that it has rarely been studied in this setting. We are aware of only one study that reported the frequency of visits for NSAP in primary care. In Australia, 1.4 of every 100 visits of children and adolescents aged 0 to 24 years were due to NSAP.19
In the present study, the incidence of girls consulting for NSAP showed 2 age peaks, and for boys the incidence decreased by age. The incidence rate for NSAP in family practice has not been reported before. Open-population studies have reported a prevalence rate of childhood chronic or recurrent abdominal pain by age.3,20,21 All studies show a peak in the occurrence of NSAP around 3–6 years of age. Although not studied yet, explanations for this age peak might be school attendance and its associated anxieties. The observed age peak of 12 to 16 years for girls in our study might be explained by menarche or dysmenorrhea.
In the medical literature a variety of expressions are used for childhood nonorganic abdominal pain: recurrent abdominal pain;1,3,20,22 chronic abdominal pain;23,24 functional abdominal pain;25 and nonspecific abdominal pain.26,27 Most of these terms include a minimal duration of abdominal pain, usually 3 months. This time criterion was arbitrarily set by Apley et al, who were the first to describe the pain syndrome in 1958.3 The time criterion was meant to reduce the risk of organic causes, because they will usually become manifest with time. The extent of additional testing for organic abnormalities differs among studies. Because of its comparable origin, ie, a nonorganic cause, we consider NSAP in family practice as a poorly studied part of the spectrum of the same pain syndrome.
Although in referred children it has been repeatedly found that chronic or recurrent abdominal pain is associated with psychological symptoms,5–9 Dutch family physicians did not associate childhood NSAP with psychological and social problems. We believe that family physicians almost certainly ask for psychosocial complaints in visits for childhood NSAP, but that they probably regarded these complaints as being too mild to code them using ICPC. Our finding gives room for speculation about whether the association found in referred children might be biased because of selective referral of children with NSAP and (severe) psychosocial problems. On the other hand, it has also been reported that family physicians have difficulty identifying psychological problems in children.28–30
Given the low percentages of additional testing and referrals, we assume that family physicians feel comfortable labeling childhood abdominal pain as NSAP, or nonorganic abdominal pain. That the physicians did not refer to a pediatric gastroenterologist (ie, for endoscopy) is the result of a 2-step procedure used in the Netherlands. A Dutch family physician will refer a child to a general pediatrician, who will refer to a pediatric gastroenterologist, if indicated. Few children revisited their family physician more than twice for NSAP. These findings are remarkable, because in referred children it has been shown that NSAP has a chronic course,10 and parents are found to be demanding and difficult to reassure.11,12 Maybe the family physicians successfully managed early stages of NSAP. That is the family physician reassured the child and parents that there were no severe underlying disorders and taught families how to deal with the abdominal pain of the child. This style may promote a self-limited outcome for common symptoms. If so, this finding supports the cost effectiveness of primary care.31
In contrast, however, we do not know whether the children who did not revisit would be free of abdominal pain or were able to cope with their abdominal pain. It has been reported that children look for help elsewhere, eg, complementary therapy and homeopathic products.32,33 Future research should further explore the prognosis of NSAP in family practice and the effect of the management of the family physician.
With respect to treatment, family physicians do not adhere to published evidence. Despite the lack of evidence for a positive effect of any medication in NSAP,34 in 21% of the visits physicians prescribed medication (predominantly laxatives and antispasmodics). They seemed to believe that laxatives are effective in NSAP or they hesitated between a diagnosis NSAP and constipation. The effectiveness of laxatives for NSAP is not supported by clinical evidence34,35 and should be studied first. In contrast to others, Dutch family physicians did not prescribe anxiolytics or anti-depressants to children with NSAP.36
Study Limitations
A limitation of our study is its dependence on the quality of the EHR registration by the family physicians. We believe, however, that the data give an accurate picture of childhood NSAP in family practice. In the Netherlands all family physicians electronically register health records and code morbidity using ICPC codes. The DNSGP-2 was set up to study morbidity in family practice, and the family physicians participating in the DNSGP-2 study were additionally trained in coding. Completeness of registration was assured by excluding family practices with poor registration.17,18 The content validity control of coding was restricted by a vignette study at the start of the registration period. The vignette study showed an adequate accuracy and consistency of coding with ICPC.18 The validity of individual patient records, however, has not been assessed in the DNSGP-2. The ICPC codes registered represent daily practice in family practice. ICPC codes were not compared with a reference standard. For the nonspecific symptom codes we use in our analysis, however, there is no reference standard. A systematic review recently has shown that the reliability of the diagnoses of a general practice research database very comparable to ours is good.37
There is always, however, a chance of misclassifying organic abdominal pain as nonorganic NSAP. This risk may be higher for diseases that lack an official ICPC code, such as NSAP. We assume family physicians code NSAP with the existing ICPC codes that describe abdominal pain without mentioning a specific organic abnormality. This assumption was based on our own clinical experience with ICPC and on the observation that 85% of the participating physicians (n = 161) coded a written patient case regarding NSAP with ICPC D01 (generalized abdominal pain).18 In addition, to reduce misclassification, we selected our cases by using the final diagnosis of a health problem. At the end of a health problem (a cluster of visits concerning the same complaint), the diagnostic process is completed and time has passed; therefore, at the end of a health problem, the uncertainty about the cause of abdominal pain is modest.
Another drawback of this health record registration database was that it was not possible to explore prognosis or duration of abdominal pain. We looked at children visiting for abdominal pain and found that most children visited only once or twice for this complaint. We do, however, not know that the children who did not contact more often were not suffering from abdominal pain. Recently our study group showed that 47% of children consulting a family practice with a new episode of abdominal pain had chronic complaints (3 or more months of abdominal pain) at first presentation.38 We feel we studied the same pain syndrome as previously reported from studies on recurrent or chronic abdominal pain. The differences with other studies is the time-frame studied and the probability of a nonorganic disorder.
Childhood NSAP is a common complaint in family practice. Less than 7% of children with NSAP diagnosed visit more than twice for this problem. Family physicians diagnose NSAP by using few additional tests and few referrals. Despite the lack of evidence for effectiveness, family physicians frequently prescribe laxatives and antispasmodics for childhood NSAP.
Footnotes
-
Conflicts of interest: authors report none.
- Received for publication August 23, 2010.
- Revision received March 9, 2011.
- Accepted for publication March 15, 2011.
- © 2011 Annals of Family Medicine, Inc.
REFERENCES




{kind=link}
Jump to section
Related Articles
Cited By...
- Qualitative study evaluating the expectations and experiences of Dutch parents of children with chronic gastrointestinal symptoms visiting their general practitioner
- Home-based guided hypnotherapy for children with functional abdominal pain and irritable bowel syndrome in primary care: study protocol for a randomised controlled trial
- Effect of faecal calprotectin testing on referrals for children with chronic gastrointestinal symptoms in primary care: study protocol for a cluster randomised controlled trial
- Managing nonspecific abdominal pain in children and young people
- Primary care faecal calprotectin testing in children with suspected inflammatory bowel disease: a diagnostic accuracy study
- Impact of functional somatic symptoms on 5-7-year-olds' healthcare use and costs
- Diagnostic Accuracy of Fecal Calprotectin for Pediatric Inflammatory Bowel Disease in Primary Care: A Prospective Cohort Study
- Predictors of Chronic Abdominal Pain Affecting the Well-Being of Children in Primary Care
- Prognosis of Abdominal Pain in Children in Primary Care--A Prospective Cohort Study
- Annals Journal Club: Nonspecific Abdominal Pain in Children
- In This Issue: Technology and Primary Care