
Article Figures & Data
Figures
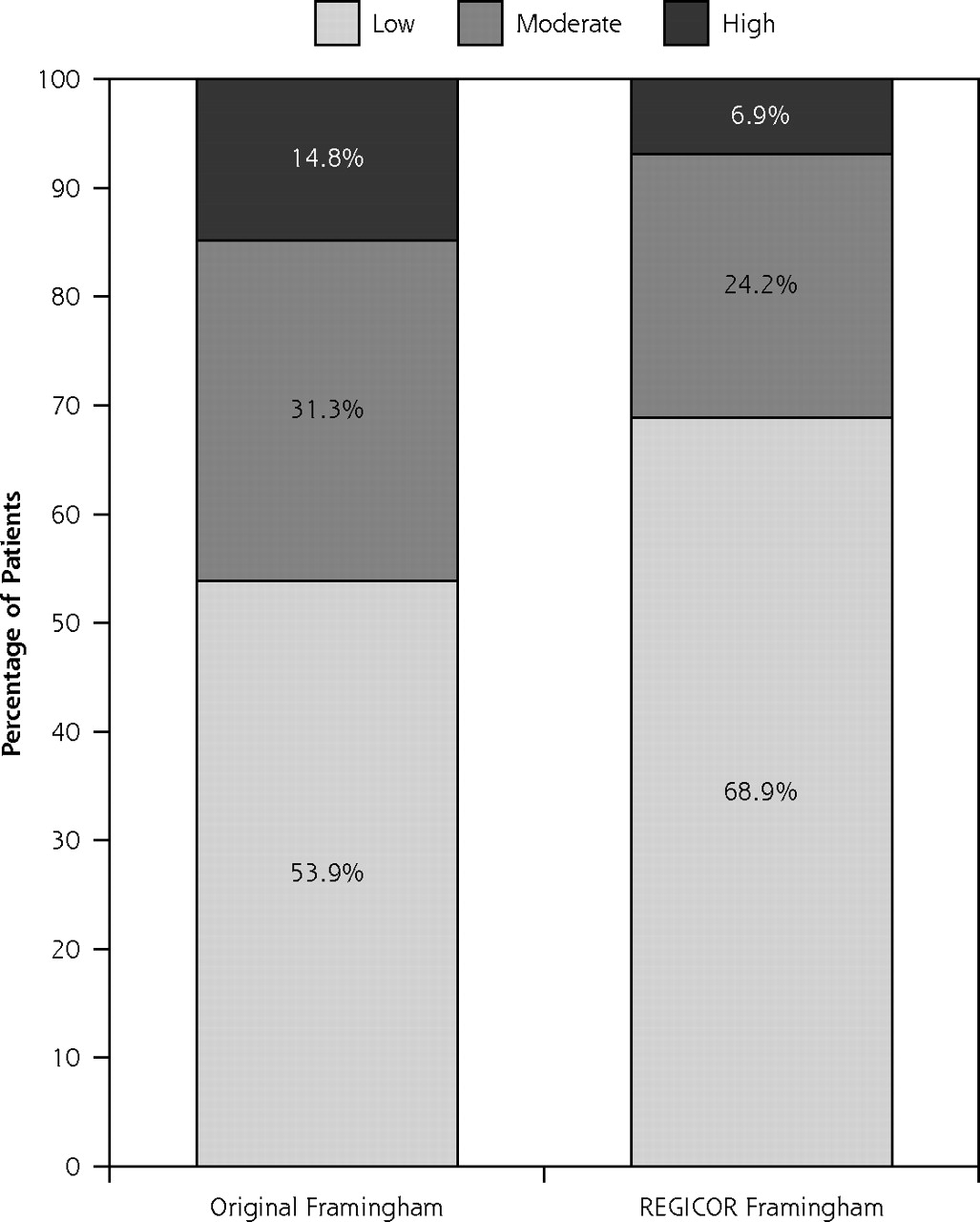
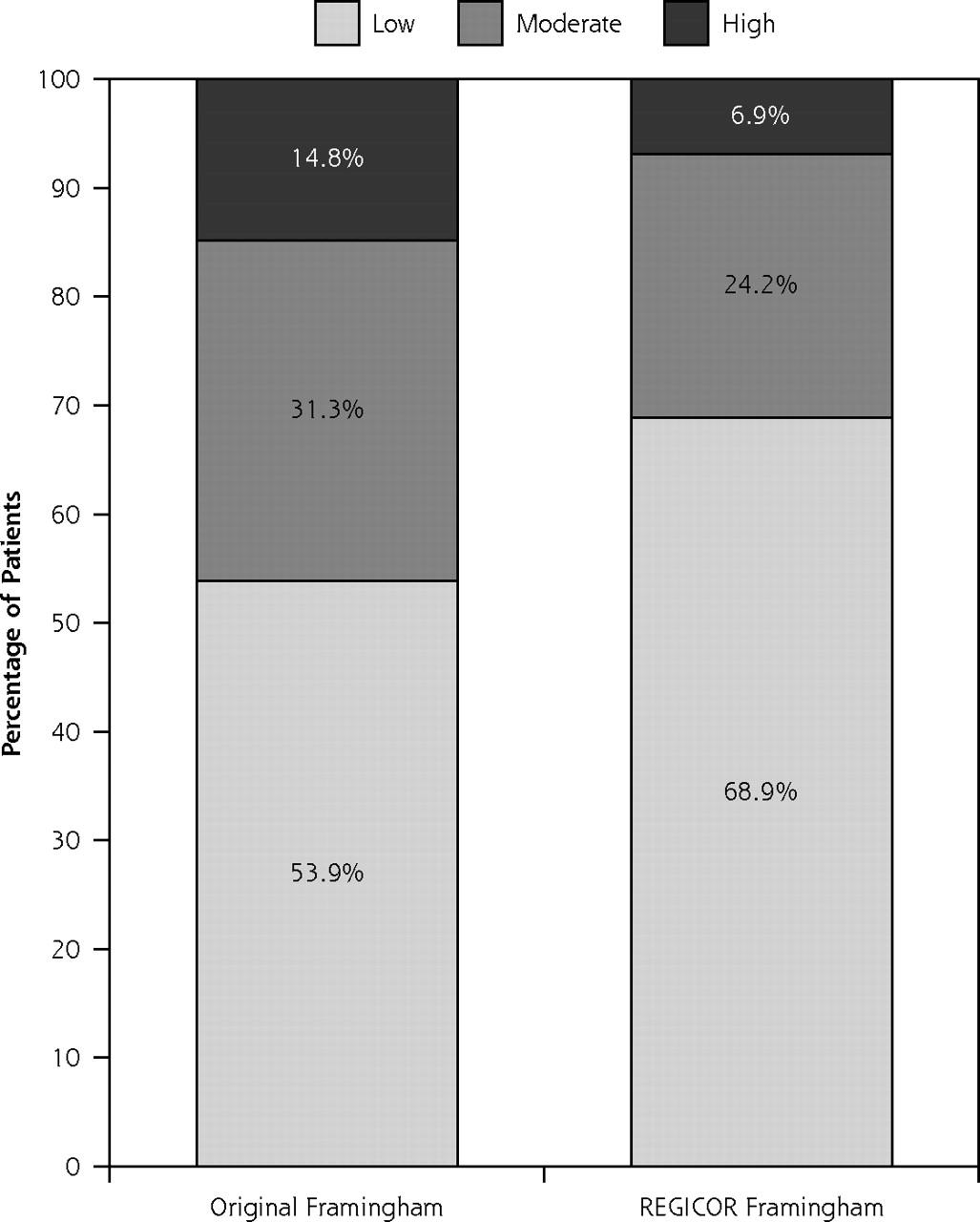
- Figure 1
Risk category distribution of the population according to the original and REGICOR Framingham risk functions.
Tables
Characteristic Overall Population (n=447) Men (n=201) Women (n=246) P Value Age, mean (SD), y 52.4 (9.6) 50.9 (9.8) 53.6 (9.2) <.01 SBP, mean (SD), mm Hg 132.0 (17.8) 130.7 (16.6) 133.1 (18.7) .147 DBP, mean (SD), mm Hg 82.1 (10.2) 82.5 (10.8) 81.7 (9.7) .466 Arterial hypertension, n (%) 122 (27.3) 51 (25.4) 71 (28.9) .410 Total cholesterol, mean (SD), mg/dL 238.9 (34.7) 239.3 (34.1) 238.7 (35.2) .861 HDL cholesterol, mean (SD), mg/dL 53.6 (15.7) 47.3 (13.2) 58.7 (15.7) <.001 LDL cholesterol, mean (SD), mg/dL 160.4 (33.2) 161.9 (31.9) 159.1 (34.2) .870 Triglycerides, median (SD), mg/dLa 107.0 (79.0–149.5) 131.0 (96.3–177.8) 96.0 (71.5–125.5) <.001 BMI, mean (SD), kg/m2 27.6 (4.1) 27.5 (3.9) 27.7 (4.3) .704 Smokers, n (%) 123 (27.5) 90 (44.8) 33 (13.4) <.001 Ex-smokers <1 y, n (%) 20 (4.5) 16 (8.0) 4 (1.6) <.01 GFR estimated by MDRD equation, mean (SD), mL/min/1.73 m2 76.8 (14.5) 80.9 (15.9) 73.4 (12.3) <.001 GFR estimated by Cockcroft-Gault formula, mean (SD), mL/min/1.73m2 86.4 (21.2) 93.4 (21.2) 80.9 (19.5) <.001 Patients with GFR <60 mL/min/1.73 m2 by MDRD equation, n (%) 30 (6.7) 8 (4.0) 22 (8.9) <.05 Patients with GFR <60 mL/min/1.73 m2 by Cockcroft-Gault formula, n (%) 28 (6.3) 9 (4.5) 19 (7.7) .158 Risk estimated by original Framingham function, mean (SD), % 11.6 16.2 7.8 <.01 Risk estimated by REGICOR Framingham function, mean (SD), % 4.3 5.7 3.3 .246 Coronary events, n (%)b 30 (6.7) 22 (10.9) 8 (3.3) <.01 -
BMI = body mass index; DBP = diastolic blood pressure; GFR = glomerular filtration rate; HDL = high-density lipoprotein; LDL=low-density lipoprotein; MDRD=Modification of Diet in Renal Disease; SBP = systolic blood pressure.
-
↵a Median of quartile 1–quartile 3, nonnormal distribution.
-
↵b Events during 10-year follow-up.
-
- Table 2
Discrimination, Calibration, and Validity Statistics for Predicted 10-year Risk of Cardiovascular Disease by REGICOR and Original Framingham Risk Functions
Original Framingham Function REGICOR Framingham Function Men Women Total Men Women Total AUROC (95% CI) 0.63 (0.52–0.75) 0.65 (0.46–0.85) 0.71 (0.61–0.80) 0.63 (0.52–0.75) 0.65 (0.46–0.85) 0.69 (0.60–0.79) Brier scorea 0.100366 0.033641 0.06364 0.097844 0.030775 0.06093 Predicted %/observed risk % (ratio) 16.9/10.9 (1.48) 7.8/3.3 (2.36) 11.6/6.7 (1.73) 5.7/10.9 (0.52) 3.3/3.3 (1.0) 4.3/6.7 (0.64) Sensitivity, % (95% CI) 40.9 (20.4–61.4) 12.5 (0.0–35.4) 33.3 (16.5–50.1) 18.2 (2.1–34.3) 14.3 (0.0–38.5) 16.7 (2.4–30.0) Specificity, % (95% CI) 72.1 (65.5–78.6) 97.5 (95.5–99.5) 86.6 (88.3–89.9) 87.2 (82.3–92.1) 98.7 (97.3–100) 93.8 (91.4–96.1) Positive predictive value, % (95% CI) 15.3 (6.1–24.4) 14.3 (0.0–40.2) 15.2 (6.5–23.8) 14.8 (1.4–28.2) 25.0 (0.0–67.4) 16.1 (3.2–29.1) Negative predictive value, % (95% CI) 90.8 (86.1–95.6) 97.1 (94.9–99.2) 94.8 (92.5–97.0) 89.7 (85.1–94.2) 97.1 (95.0–99.2) 94.0 (91.7–96.3) Positive likelihood ratio 1.5 4.9 2.5 1.4 11.2 2.7 Negative likelihood ratio 0.8 0.9 0.8 0.9 0.9 0.9 Utility 1.8 5.5 3.2 1.4 13.4 3.0 -
AUROC = Area under the receiver operating characteristic curve; CI = confidence interval.
-
↵a A lower score indicates better accuracy of risk estimates.
-
- Table 3
Characteristics of Patients Identified as of High Risk by the Original and REGICOR Framingham Functions
Characteristic High Risk by Original Framingham (n=66) High Risk by REGICOR Framingham (n=31) Age, mean (SD), y 59.2 (8.6) 61.6 (7.1) SBP, mean (SD), mm Hg 142.1 (15.7) 142.2 (11.5) DBP, mean (SD), mm Hg 86.6 (10.4) 86.1 (7.6) Total cholesterol, mean (SD), mg/dL 252.1 (32.7) 255.2 (30.5) HDL cholesterol, mean (SD), mg/dL 42.3 (12.9) 40.2 (13.4) LDL cholesterol, mean (SD), mg/dL 157.7 (32.0) 182.1 (33.7) Triglycerides, median (SD), mg/dLa 145.0 (105.0–206.8) 139.0 (106.0–205.0) BMI, mean (SD), kg/m2 28.7 (4.4) 28.7 (3.8) Smokers, n (%) 34 (51.5) 17 (54.8) Ex-smokers <1 y, n (%) 10 (15.2) 5 (16.1) Arterial hypertension, n (%) 25 (37.9) 11 (35.5) GFR by MDRD equation, mean (SD), mL/min/1.73 m2 75.7 (10.4) 72.9 (8.8) GFR by Cockcroft-Gault formula, mean (SD), mL/min/1.73 m2 85.7 (21.3) 79.9 (16.2) Patients with GFR <60 mL/min/1.73m2 by MDRD equation, n (%) 3 (4.5) 2 (6.5) Patients with GFR <60 mL/min/1.73 m2 by Cockcroft-Gault formula, n (%) 6 (9.1) 4 (12.9) Coronary events, n (%)b 10 (15.2) 5 (16.1) Coronary risk estimated by original Framingham function, % (?) 28.5 (7.9) 34.2 (8.1) Cardiovascular risk estimated by REGICOR Framingham function, % (?) 10.6 (3.4) 13.1 (3.6) Men, n (%) 59 (89.4) 27 (87.1) -
BMI = body mass index; DBP = diastolic blood pressure; GFR = glomerular filtration rate; HDL=high-density lipoprotein; LDL=low-density lipoprotein; MDRD=Modification of Diet in Renal Disease; SBP = systolic blood pressure.
-
↵a Median of quartile 1–quartile 3, nonnormal distribution.
-
↵b Events during 10-year follow-up.
-
Characteristics Patients Without Coronary Events (n=417) Patients With Coronary Events (n=30) P Value Age, mean (SD), y 52.0 (9.5) 58.3 (8.8) <.001 Male, no (%) 179 (42.9) 22 (73.3) <.01 SBP, mean (SD), mm Hg 131.9 (18.0) 133.4 (16.2) .657 DBP, mean (SD), mm Hg 82.2 (10.1) 80.9 (11.2) .519 Total cholesterol, mean (SD), mg/dL 238.9 (34.4) 239.5 (38.9) .617 HDL cholesterol, mean (SD), mg/dL 53.9 (15.8) 49.7 (13.0) .160 LDL cholesterol, mean (SD), mg/dL 160.1 (32.7) 163.9 (39.3) .558 Triglycerides, median (SD), mg/dLa 107.0 (77.0–151.5) 107.0 (87.0–133.5) .958 BMI, mean (SD), kg/m2 27.7 (4.1) 27.1 (4.1) .573 Smokers, n (%) 111 (26.6) 12 (40.0) .112 Arterial hypertension, n (%) 110 (26.4) 12 (40.0) .105 Risk estimated by original Framingham function, mean (SD), % 11.1 (8.4) 18.4 (12.0) <.01 Risk estimated by REGICOR Framingham function, mean (SD), % 4.2 (3.2) 6.9 (4.8) <.01 GFR estimated by Cockcroft-Gault formula, mean (SD), mL/min/1.73m2) 86.7 (21.2) 80.9 (19.3) .232 Patients with GFR <60 mL/min/1.73m2 by Cockcroft-Gault formula, n (%) 26 (6.2) 2 (6.7) .767 GFR estimated by MDRD equation, mean (SD), mL/min/1.73 m2 76.6 (14.3) 78.6 (16.8) .483 Patients with GFR <60 mL/min/1.73 m2 by MDRD equation, n (%) 26 (6.2) 4 (13.3) .261 -
BMI = body mass index; DBP = diastolic blood pressure; GFR = glomerular filtration rate; HDL = high-density lipoprotein; LDL=low-density lipoprotein; MDRD=Modification of Diet in Renal Disease; SBP = systolic blood pressure.
-
↵a Median of quartile 1–quartile 3.
-
- Table 5
Patients as Candidates for Drug Therapy According to the SCORE Guidelines Recommendations, With Risk Estimated by the Original Framingham and REGICOR Risk Functions
Recommended Therapy Total (n=447) Men (n=201) Women (n=246) Lipid-lowering therapy Original Framingham, n (%) 64 (14.3) 57 (28.3) 7 (2.8) REGICOR Framingham, n (%) 30 (6.7) 26 (12.9) 4 (1.6) P value <.001 <.001 .360 Antihypertensive therapy Original Framingham, n (%) 56 (12.5) 41 (20.4) 15 (6.1) REGICOR Framingham, n (%) 35 (7.8) 23 (11.4) 12 (4.9) P value <.05 <.05 .55
The Article in Brief
Original and REGICOR Framingham Functions in a Nondiabetic Population of a Spanish Health Care Center: A Validation Study
Francisco Buitrago , and colleagues
Background Risk prediction models are designed to estimate the probability of a patient developing a clinical condition based on known risk factors. This study evaluates the performance of 2 long-established risk scoring mechanisms for coronary disease: the original Framingham and REGICOR Framingham mechanisms.
What This Study Found Researchers find that one scoring mechanism overestimates risk, whereas the other underestimates it. This 10-year observational study of 447 adult nondiabetic patients in Spain finds that the Framingham risk function overestimates coronary risk by 73 percent, whereas the REGICOR Framingham function underpredicts the population�s coronary risk by 64 percent. Moreover, the original Framingham function selects a greater percentage of candidates for antihypertensive and lipid-lowering therapies than the REGICOR function. The proportion of patients included in the high coronary risk category also is doubled with the original Framingham equation.
Implications
- That both models fail to accurately predict the population�s actual coronary risk in the 10-year follow-up period is not surprising to the authors. The original Framingham study was conducted before the widespread use of effective treatment for cardiovascular risk factors, so its equation currently overpredicts cardiovascular risk when applied to populations who have their risk factors actively managed.
- The authors conclude the Framingham risk mechanisms could be improved by revising them to include additional cardiovascular risk factors and variables, such as family history of cardiovascular disease in a first-degree relative, social deprivation, body mass index, and current prescription of antihypertensive therapy.




{kind=link}