
Abstract
PURPOSE Pain, a common reason for visits to primary care physicians, is often not well managed. The objective of this study was to determine the effectiveness of pain management interventions suitable for primary care physicians.
METHODS Patients from 14 rural primary care practices (47 physicians) who reported diverse pain problems with (n = 644) or without (n = 693) psychosocial problems were randomized to usual-care or intervention groups. All patients in the intervention group received information tailored to their problems and concerns (INFO). These patients’ physicians received feedback about their patients’ problems and concerns (FEED). A nurse-educator (NE) telephoned patients with pain and psychosocial problems to teach problem-solving strategies and basic pain management skills. Outcomes were assessed with the Medical Outcomes Study 36-Item Short-Form and the Functional Interference Estimate at baseline, 6 months, and 12 months.
RESULTS Patients with pain and psychosocial problems randomized to INFOFEED+NE significantly improved on the bodily pain (P = .011), role physical (P = .025), vitality (P <.001), role emotional (P = .048), and the Functional Interference Estimate (P = .027) scales compared with usual-care patients at 6 months. These improvements were maintained at the 12-month assessment even though these patients had received, on average, only 3 telephone calls. Compared with usual-care patients, at 6 months patients who received INFOFEED alone experienced minimal improvements that were not sustained at the 12-month assessment.
CONCLUSIONS For patients with pain and psychosocial problems, telephone-based assistance resulted in significant, sustained benefit in pain and psychosocial problems.
INTRODUCTION
Pain is among the most common complaints in primary care. It accounts for considerable suffering for patients, increased health care costs, and lost productivity, and pain is generally associated with low self-rated health.1–4 Psychosocial and psychiatric problems frequently are concurrent with pain and complicate its management.5,6
Pain management is most effective when it engages the patient in self-management.7,8 Cognitive-behavioral approaches to pain management have shown efficacy in decreasing pain and functional disability.9 Problem-solving therapy is an efficient, effective approach for aiding patients with symptoms of depression and psychosocial issues associated with pain and other medical problems.10–12
Many primary care physicians do not feel capable of supporting patient self-management and the delivery of problem-solving therapy or cognitive-behavioral therapies because of limited experience and resources. Telephone-based approaches, however, have been shown to be effective in the delivery of medical follow-up for patients with chronic illness, for teaching basic pain self-management skills, and treating depression.13–15 Previously, we pilot-tested an approach designed for primary care patients with diverse pain problems. We based our approach on giving patients information specifically tailored to their needs and a telephone-based nurse-educator intervention that provided basic pain self-management skills and problem-solving therapy.14 We reasoned that patients with pain but no self-identified psychosocial problems would benefit from tailored information alone, whereas patients with pain and self-identified psychosocial problems would benefit from tailored information plus the nurse-educator intervention. Based on positive results from the pilot test, we used a randomized design to determine the effectiveness of this approach on pain management in rural primary care practices.
METHODS
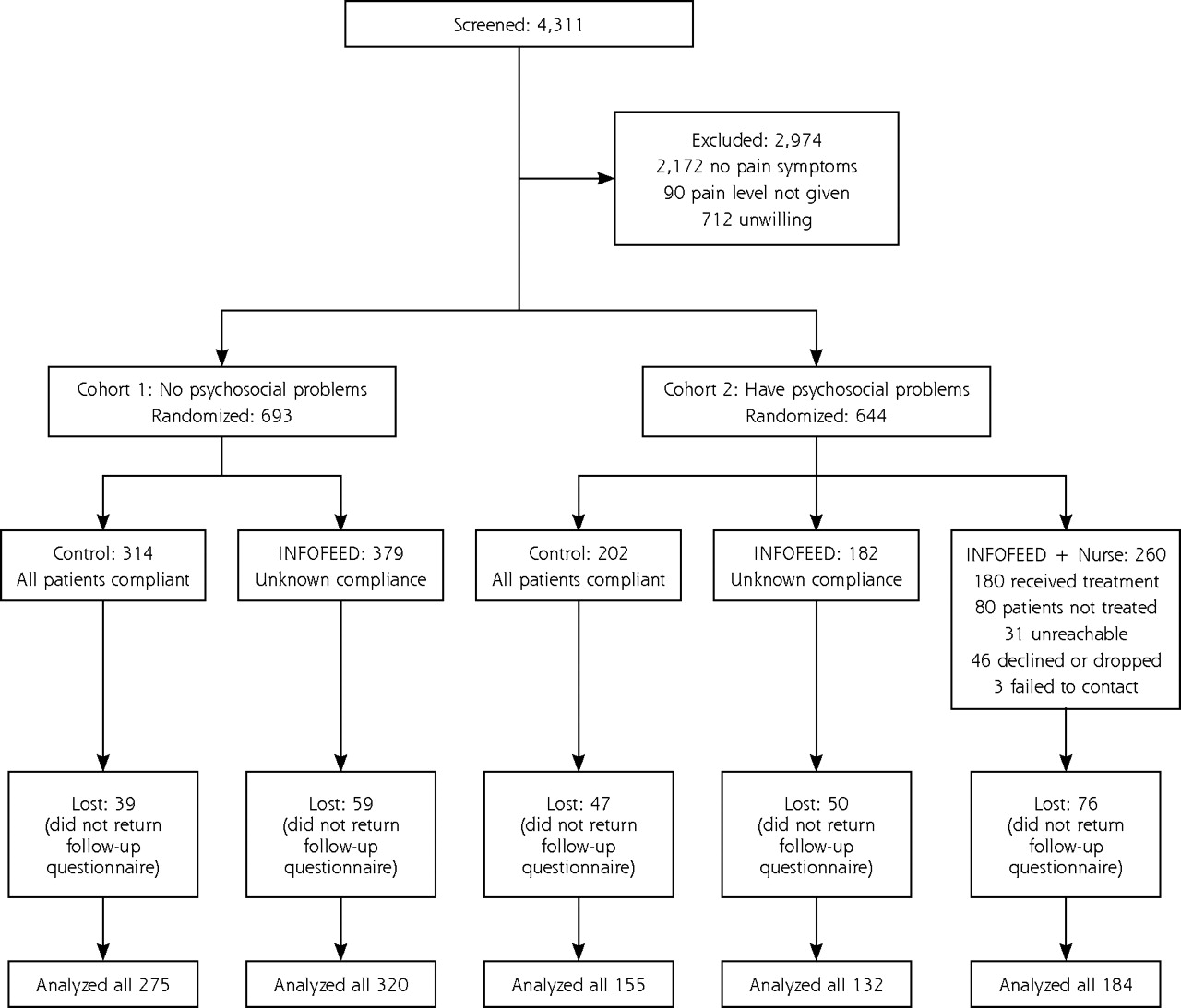
Patients were recruited from 14 rural primary care practices (47 physicians) in Vermont, New Hampshire, and Maine that volunteered in response to listing the study in the newsletter (distribution of 400) of the Dartmouth Primary Care Practice-Based Research Network (Dartmouth COOP). Three hundred adult patients aged 19 to 69 years were randomly selected (every fourth or fifth patient depending on panel size) from each physician’s panel of patients to receive a letter from their physician explaining that the practice was involved in research designed to improve treatment of pain. Figure 1⇓ displays the enrollment process for the study. All methods and procedures were approved by the institutional review boards of Dartmouth Medical School and of the participating practices.

Flow diagram of enrollment and randomization.
Patients were asked to complete a standard questionnaire that listed common medical and psychosocial problems for patients seen in primary care16,17 and return it in a stamped, addressed envelope along with informed consent for follow-up. Patients who self-reported at least 1 month’s duration of pain at a level of 3 or more on a 5-point scale (1 = no pain to 5 = severe pain) were further stratified into 2 groups: patients without (cohort 1) and patients with (cohort 2) self-reported psychosocial problems. Serious psychosocial problems were defined as endorsement of moderate to severe impairment in 1 or more of the following areas: emotional problems, social activities, social support, sexual problems, substance use, and violence or abuse in the home.
Randomization
Within each practice, cohort 1 patients were randomized to usual care or usual care with information and physician feedback tailored to their needs (INFOFEED). Within each practice, cohort 2 patients were randomized for usual care, INFOFEED, or INFOFEED with nurse-educator (NE) telephone contact (INFOFEED+NE). Randomization was initially based on random numbers printed on the baseline assessment forms, followed by computer-based assignment.
Randomization was by patient rather than physician practice because the intervention focused on the patient; therefore, although the physician received feedback regarding patients in the intervention groups, the physicians were not aware of which patients were randomly selected as controls. This method was used in our pilot study14 with no obvious confounding of intervention effects in the control group.
Interventions
Patients in the usual-care group received their care as usual. For the INFOFEED group, a computer-based algorithm generated a “prescription” letter tailored to the patient’s responses on the baseline survey questionnaire. The letter referred the patients to specific pages of self-care educational information in a health education booklet,16 and both the letter and booklet were mailed to the patient. Their physicians received a computer-generated feedback form that described the items endorsed by the patient, particularly the presence and level of pain.17 Additionally, the physicians were provided with a red sticker that said “Assess Pain,” which was placed on the patients’ charts as a reminder.18
For the nurse-educator intervention (INFOFEED+ NE), 3 nurse-educators worked out of the research office and contacted patients by telephone. The nurse-educators (1) conducted an assessment of pain and psychosocial problems; (2) established patient preferences for types of pain management strategies; (3) reviewed pain self-management strategies and provided, via mail, supplemental written material (1- to 2-page summaries of pain self-management, relaxation, activity pacing, sleep hygiene) and audiotaped relaxation exercises; (4) provided a problem-solving approach for psychosocial issues based on a problem-solving manual developed for treatment of patients in primary care19,20; and (5) provided rapid feedback to the primary care physician regarding the interventions initiated and identification of troubling symptoms or psychosocial problems.
The problem-solving material included a description of the steps of problem solving: problem definition, choice of achievable goals, brainstorming solutions, solution selection, implementation of the solution, and evaluation of success. Worksheets on which patients could define the problem, list advantages and disadvantages of potential solutions to the problem, and record the solution chosen and action plan were also provided (see http://www.howsyourhealth.org).
The nurse-educator training program was a modified version of Hegel and colleagues’ problem-solving training,19,20 which included 3 components: (1) an 8-hour training practicum that included didactics, watching a videotape demonstrating the problem-solving technique, role playing, and reading the treatment manual; (2) treatment of a minimum of 5 practice cases, each lasting at least 4 sessions; and (3) ongoing group supervision with the trainer (JLS) in which audiotapes of the sessions were reviewed for treatment protocol adherence. All nurse-educators met the criteria of at least 3 tape-recorded sessions with a satisfactory rating before treating randomized patients. Nurses were also trained in pain self-management educational modules that included standard cognitive-behavioral techniques (activity pacing, relaxation, sleep hygiene, and cognitive restructuring). During the course of the intervention, all telephone sessions were tape-recorded for weekly supervision and treatment fidelity (15% of audiotapes were randomly selected for treatment reliability and met satisfactory standards).19
The protocol allowed for up to 8 telephone calls during the active intervention phase and 1 booster call between the intervention calls and the 6-month assessment. Patients in INFOFEED+NE received an average of 3 calls (range, 0 to 8). The average duration of each call was 38 minutes.
Outcome Measures
Outcome measures included Medical Outcomes Study 36-Item Short-Form (SF-36) scores,21,22 Functional Interference Estimate scores,23 and a measure of health care utilization. Questionnaires assessing these measures were sent to participants with a stamped return envelope at baseline and at 6 and 12 months after randomization by a research assistant who was blind to treatment condition.
The SF-36 is a 36-item questionnaire that measures different health concepts (higher scores indicate a more favorable health state).21,22 For this study, the primary outcome measure was bodily pain; however, we also examined domains that could be related to pain, including physical functioning, role limitations caused by physical health problems, role limitations caused by personal or emotional problems, social functioning, and vitality.
Using the Functional Interference Estimate,23 we assessed the degree to which pain interfered with daily activities rated on a 6-point scale ranging from “pain usually or severely interferes” to “pain rarely interferes.” Data supporting the reliability and validity of the measure have been reported for both pain clinic and primary care populations.23,24
For health care utilization, at the baseline and each of the follow-up assessment points, we asked patients to self-report the number of physician visits, days the hospital, and days in bed or at home during the last 6 months.
Statistical Analysis
Two-sample t tests and analysis of variance were used to evaluate continuous baseline variables, and the χ2 test was used to evaluate categorical baseline variables for the adequacy of randomization. Mixed-effects regression analysis was used to evaluate change from baseline to 6- and 12-month follow-up and to compare intervention groups with usual care. A separate regression analysis was performed for the primary outcome measure, bodily pain, and for each of the other outcome measures. Mixed-effects regression assumes a fixed treatment effect and a random subject effect. This analytic method provides an estimate of treatment group differences that accounts for correlation within each subject’s repeated longitudinal observations. Because self-reported number of days in hospital and in bed or at home had severely skewed distributions, the Wilcoxon rank-sum test was used to analyze these variables. Unless otherwise indicated, all treatment group comparisons were based on the principle of intention to treat. All P values presented are 2-sided.
RESULTS
Table 1⇓ describes the demographic characteristics of the 1,066 randomized patients who provided follow-up data. Participants in the study tended to be in their mid 40s, educated (92% with at least a high-school education), and female (65%). Most participants were married (62%) and working full-time (50%) or part-time (16%). Consistent with the demographics of northern New England, the sample was predominately white (92%). Compared with patients without psychosocial problems, patients with pain and psychosocial problems were less educated, less-often married, less-often employed, and bothered by pain of longer duration, and they suffered a greater number of sick days and had more frequent visits to physicians.
Baseline Demographic Characteristics by Cohort and Intervention
The most common types of pain persisting for at least 1 month were joint pain (54%), back pain (48%), headaches (26%), and abdominal pain (16%). Most patients reported experiencing their pain for longer than 1 year (84%), and a substantial number (27%) reported experiencing pain for 11 years or more. Most patients had 2 or more locations of pain: 92% of cohort 1 and 96% for cohort 2. The severity of pain was associated with time lost from work, disability, and utilization of health care. For mild, moderate, and severe pain, the percentages of patients having spent at least 1 day sick at home were, respectively, 28%, 43%, and 70%; the percentages of patients hospitalized at least once in the past year were, respectively, 10%, 18% and 28%.
To evaluate for potential selection bias, we compared responses to the screening questionnaire for patients who were unwilling to be randomized (n = 712) with responses for patients who were randomized. No significant differences emerged on age, sex, pain intensity, emotional distress, or the percentage reporting that they “have enough money to buy the essentials.” There therefore does not seem to be any systematic selection bias. We also examined for potential dropout bias and found no differences in dropout rate across interventions in either cohort.
Within the cohort reporting pain but no psychosocial problems (cohort 1), 379 were randomized to receive the INFOFEED intervention, and 314 were randomized to usual care. Analysis of baseline demographic data (Table 1⇑) showed a trend for patients randomized to INFOFEED to be more educated (P = .052) and an imbalance in the number of control patients who reported serious obesity (17%) compared with patients randomized to INFOFEED (10%). Additionally, control patients tended to have lower scores on the role physical subscale of the SF-36 (P = .084, Table 2⇓).
Baseline Scores and 6-Month and 1-Year Outcomes for Cohort 1
For the cohort reporting pain and psychosocial problems (cohort 2), 260 were randomized to receive the INFOFEED+NE intervention, 182 to receive the INFOFEED intervention, and 202 to receive usual care. Analysis of baseline demographics (Table 1⇑) for cohort 2 showed a slightly lower proportion of white participants in the usual-care group (88%) compared with the INFOFEED (92%), and INFOFEED+NE (96%) groups (P = .065), a lower percentage of usual-care patients with pain duration of 4 years or more, and a higher percentage of patients in the INFOFEED group reporting a history of substance abuse (P = .005). Additionally, at baseline, patients in the INFOFEED group reported higher Functional Interference Estimate scores (P = .029) and more days in the hospital (P = .02) compared with the usual-care group, and patients in the INFOFFED+NE group reported more physician visits (P = .047) compared with the usual-care group (Table 3⇓). These factors, therefore, were used as adjustment variables in the linear mixed-effects model analyses.
Baseline Scores and 6-Month and 1-Year Outcomes for Cohort 2
Examination of the randomization scheme by practice showed that there was imbalanced randomization in 3 practices, which accounts for the variation in sample size across groups. We compared patient baseline demographic variables and outcome variables for those 3 practices with the others and found no significant differences on any variable; therefore, we combined the data for the analyses.
Finally, in a comparison of outcomes across the 3 nurses, we found no differences in outcomes for the study measures.
Impact of the Interventions
Patient Information and Physician Feedback (INFOFEED)
Linear mixed-effects models using change scores from baseline to the 6-month (intervention phase) and 12-month (maintenance phase) follow-ups for cohort 1 showed significantly greater improvement on the social functioning subscale (P = .03) for the INFOFEED group at the 6-month assessment and no group differences at the 12-month assessment (Table 2⇑). We then compared outcomes for patients randomized to INFOFEED across cohorts 1 and 2 with patients receiving usual care across both cohorts. Change scores from baseline to the 6-month follow-up showed patients in the INFOFEED group improved significantly compared with patients in the usual-care group on the social functioning subscale (P = .037) and the Functional Interference Estimate (P = .045), with a trend in the same direction on the vitality scale (P = .083). These differences disappeared by 12 months.
Patient Information and Physician Feedback Plus Nurse-Educator (INFOFEED+NE)
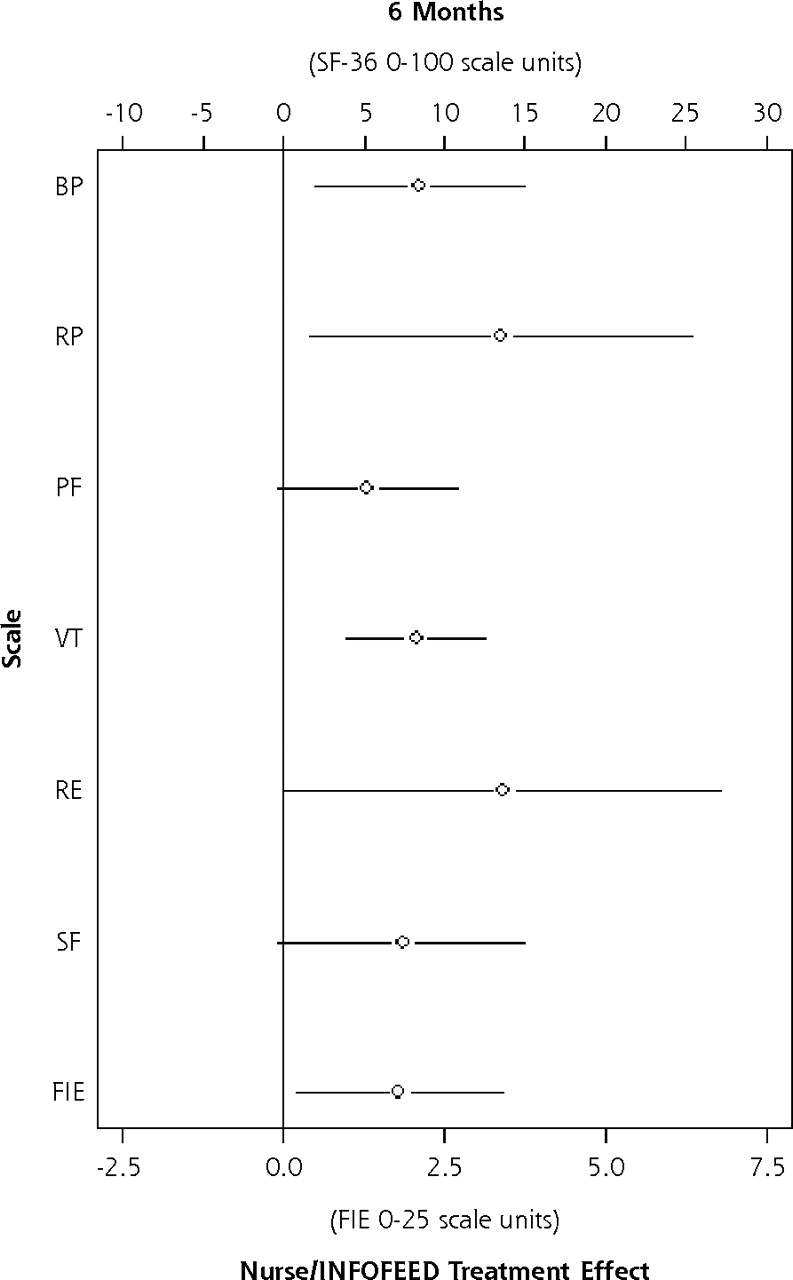
Analysis of data from the SF-36 and Functional Interference Estimate measures showed that the INFOFEED+NE intervention group patients improved significantly more than those in the usual-care group at the 6-month assessment on the following scales: bodily pain (P = .011), role physical (P = .025), vitality (P <.001), role emotional (P = .048), and the Functional Interference Estimate (P = .027), with trends in the same direction for the physical function (P = .062) and social functioning (P = .058) (Table 3⇑, Figure 2⇓). At 12 months, significant differences were sustained for vitality (P = .048), role emotional (P = .046), and the Functional Interference Estimate (P = .02) scales, with a trend in the same direction for bodily pain (P = .06). Table 3⇑ and Figure 2⇓ show that gains attained at 6 months were maintained at the 12-month follow-up. The significance level for bodily pain was somewhat attenuated because control patients, who were receiving ongoing usual care, showed slight improvement at the 12-month assessment on these scales.
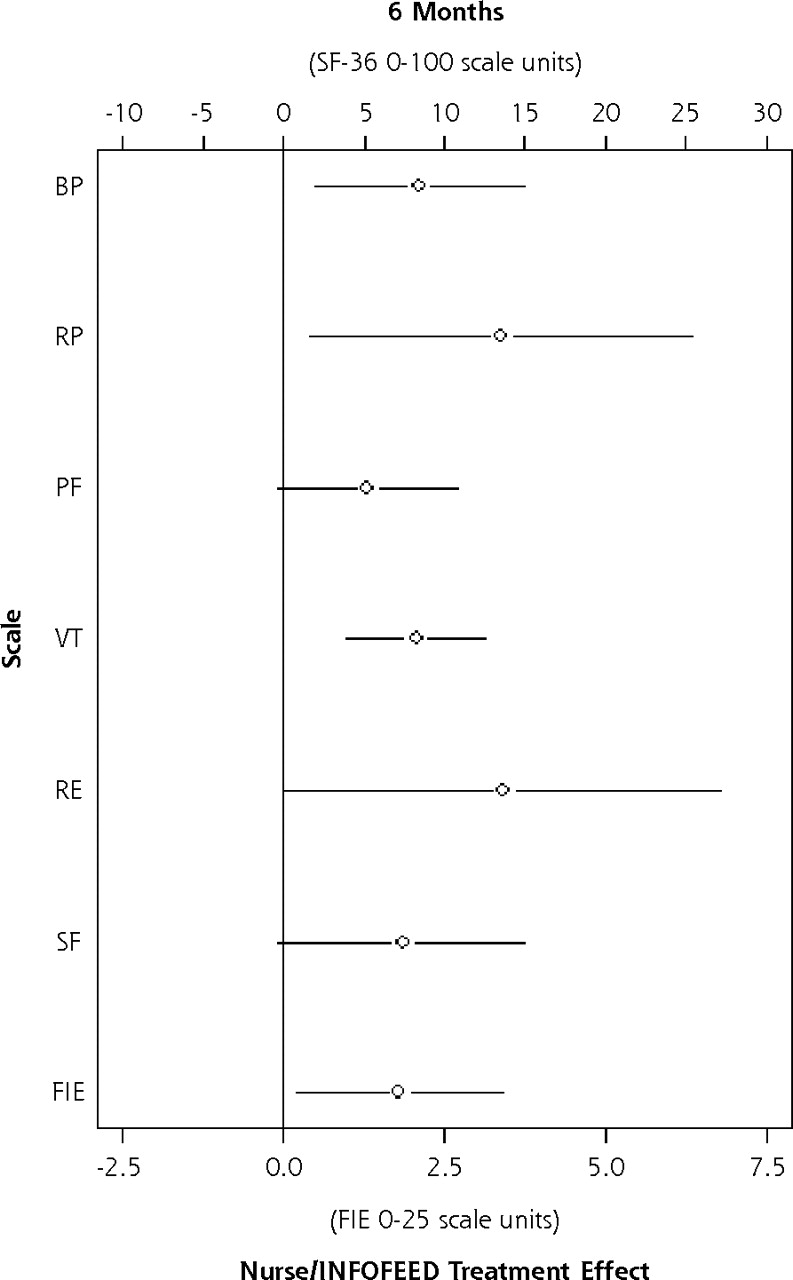
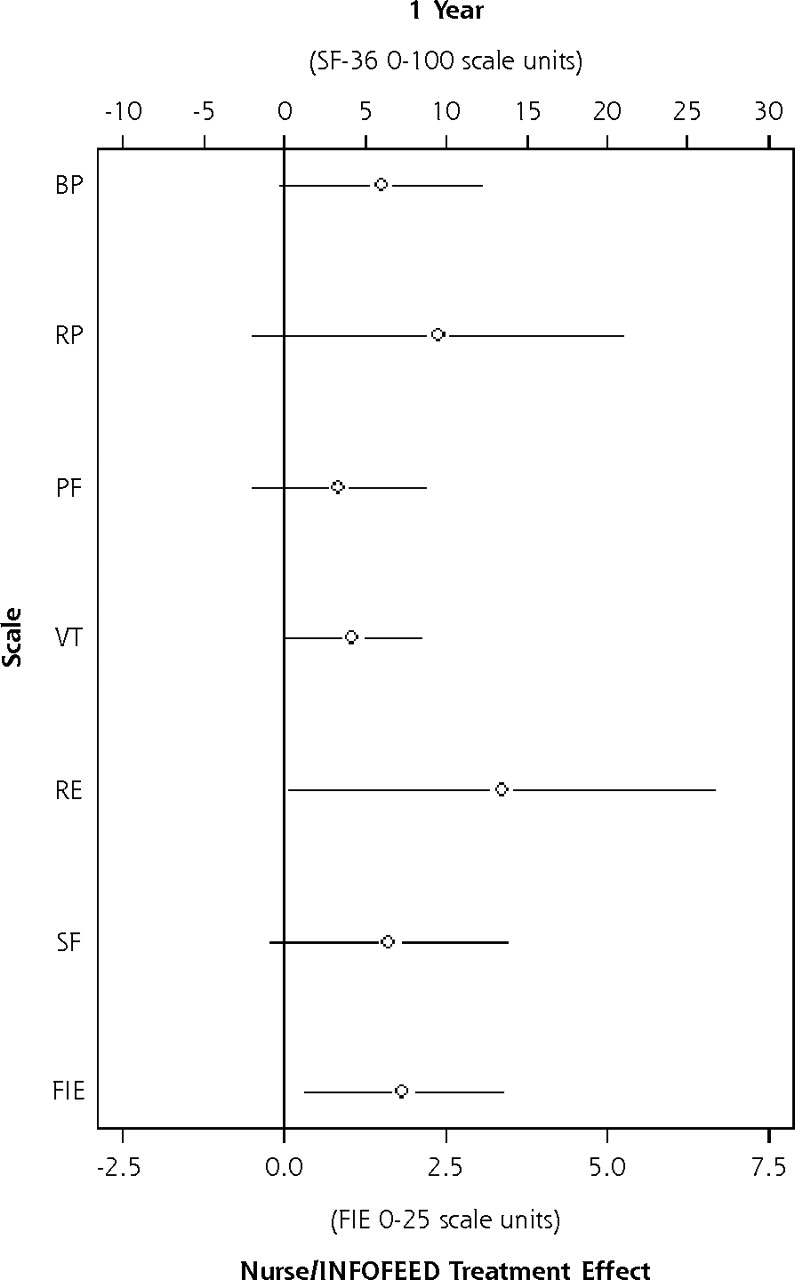
Impact of INFOFEED+NE on patient-reported functional outcomes (patients with pain and psychosocial problems).
Note: Open circles represent the difference in change scores between INFOFEED+NE and controls, and the lines represent the 95% confidence interval.
INFOFEED+NE = patient information and physician feedback plus nurse-educator, SF-36 = Medical Outcomes Study 36-Item Short-Form; BP = bodily pain; RP = role physical; PF = physical function; VT = vitality; RE = role emotional; SF = social function; FIE = functional interference estimate.
Some patients (n = 80) never received a telephone call, either because they could not be reached (n = 31), they declined the telephone calls (n = 46) after randomization, or because of administrative error (n = 3). We reexamined the impact of the intervention on cohort 2 with these patients excluded (treatment-received analysis) and observed the same pattern of results; however, improvements after the intervention were generally larger for the INFOFEED+NE group. There were no significant differences between outcomes for patients who received 1 to 2 calls and those who received 3 or more calls .
When we compared the INFOFEED intervention group with the usual-care group in cohort 2, we found less decline in Functional Interference Estimate scores (P = .042) and a trend for greater improvement in vitality (P = .059) in the INFOFEED group at the 6-month assessment. These differences disappeared at the 12-month assessment.
Because this is the first randomized trial of these interventions and because we selected a subset of scales from the SF-36 for analyses, we chose to report results that were not corrected for multiple comparisons. If a Bonferroni correction were applied, however, improvement in vitality scores for patients in the INFOFEED+NE group would be the single significant difference.
Clinically Meaningful Improvements
A 10-point change on SF-36 subscales is a marker for clinically meaningful improvements.22 We observed no difference in the proportion of patients achieving clinically meaningful improvement in this measure for the INFOFEED group compared with the usual-care group. Comparing the INFOFEED+NE group with the usual-care group at the 6-month assessment, we observed differences in the proportion of patients achieving meaningful improvement for bodily pain (53% vs 40%; P = .03), role physical (41% vs 26%, P = .01), social functioning (55% vs 37%, P = .005), and vitality (46% vs 28%, P = .002) subscales, but not for role emotional (32% vs 22%, P =.078) or physical function (36% vs 27%, P = .10). At 12 months, clinically meaningful differences were seen on the vitality (51% vs 36%, P <.02), role physical (41% vs 28%, P = .38), and role emotional (39% vs 24%, P = .12) subscales but not the bodily pain (50% vs 40%, P = .15), physical function (38% vs 37%, P = .89), or social functioning (47% vs 41%, P = .38).
Health Utilization
Patients receiving INFOFEED in cohort 1 reported a significantly fewer number of days in the hospital compared with patients in the usual-care group at the 6-month (P = .019) and 12-month (P = .05) assessments. Although significant, this difference may not be clinically meaningful since, on average, all patients reported less than 1 day in the hospital during the previous 6 months. No intervention effect was seen for cohort 2.
DISCUSSION
Based on national data using the same screening survey instruments used in the current study, more than one third of Americans aged 19 to 69 years report levels of pain similar to that studied here, and approximately 40% of these Americans also report psychosocial problems.25,26 Recent research has emphasized the need to develop pain management interventions that can be integrated into primary care.27–29 The results of this study show that, for patients with pain and psychosocial problems, a telephone-based intervention which includes cognitive-behavioral pain management strategies and problem-solving therapy can significantly reduce pain and improve both psychosocial and physical function to a clinically meaningful degree.
In the era of managed care and limited resources, development of alternative health care models is essential. The nurse-educator intervention is an interesting approach. First, operating from a central location and exclusively by telephone and through the mail, the nurses were able to intervene with patients from 14 practices distributed over a wide geographic area. Second, positive outcomes were obtained with an average of 3 telephone calls for patients who had diverse pain problems and serious psychosocial problems, indicating that the intervention does not need to be time intensive.
Although the study produced positive results, there are limitations to the study: (1) it was conducted with a primarily white population living in northern New England; (2) we were unable to ascertain how well the clinicians responded to the INFOFEED, and we did not control the interval between the intervention and the next physician appointment, so our results may underestimate the potential of INFOFEED; and (3) our utilization data were based on self-report.
Perhaps more challenging than the scientific limitations of this study are the practical questions it raises: Who would do an INFOFEED+NE intervention, and how would these interventions fit into everyday practice? For INFOFEED only, material and labor costs are small. A Web-based version of INFOFEED is available without charge, registration, or advertisement (see http://www.howsyourhealthorg).17,30
For the nurse-educator, we estimate a cost of $50 per patient treated (assuming a registered nurse earns $30/hour) and $250 to $400 per patient meaningfully improved at 6 months (assuming 12 to 15 patients improved compared with usual-care patients). There are many programs that now offer physician practices extra money for attaining quality objectives. Payment of $50 for reduced morbidity from pain and psychosocial problems using the nurse-educator intervention may be cost-effective.
In conclusion, the results of the current study support the effectiveness of the tailored information for patients with pain, combined with feedback to physicians, and telephone nurse-educator support of pain self-management. The most cost-effective method for sharing information and providing support must still be determined.
Footnotes
-
Conflicts of interest: none reported
-
Funding support: This research was supported by grants from the Agency for Healthcare Research, and Quality (HS10265) and the Robert Wood Johnson Foundation. Neither funding source was directly involved in the design or conduct of the study or with preparation or approval of this manuscript.
-
Study participants: Participating Physician Groups: Danville Health Center, Danville, Vt (Susan Fine, MD, Mariel Hess, NP, Timothy Tanner, MD); Island Pond Health Center, Island Pond, Vt (Peter Harris, MD, Jim Lontine, PA, Robert Primeau, MD); Concord Health Center, Concord, Vt (Brad Armstrong, MD, Megan Haygood, NP, Susan Taney, NP); Robert Tortolani, MD, Brattleboro, Vt (Robert Tortolani, MD); Dartmouth Hitchcock–Nashua, Internal Medicine, Nashua, NH (Sherman Baker, Jr, MD, Leslie Cook, MD, Joseph Karpicz, MD); Dartmouth Hitchcock–Nashua, Family Practice, Nashua, NH (Nanyee Keyes, MD, Jonathan Thyng, MD); Neshobe Family Medicine, Brandon, Vt (Jeffrey Wulfman, MD, William Barrett, MD, Carrie Wulfman, MD); Burlington Primary Care, Burlington, Vt (Stephanie Bellomo, MD, Cynthia Haselton, MD, Robert Penney, MD); The Hitchcock Clinic–Indian Stream, Colebrook, NH (Joseph Fothergill, MD, Joseph Capobianco, MD, Diane Zavotsky, MD, Robert Soucy, DO, Mary Judd, PA, Mary Weber, ARNP); John Kaminski, MD, Hampton, NH (John Kaminski, MD, Pam Hagan, ARNP, Janet Miller, ARNP); Evergreen Family Health, Williston, Vt (Paul Reiss, MD); Seacoast Family Practice of Exeter, Exeter, NH (Jim Bloomer, MD); Community Care Center, Lebanon, NH (Larry Lancaster, ARNP, Carol Williams-Suich, CRNP, Eric Bronstein, MD, Brian Lombardo, MD, Karuna Gupta, MD, Peter Mason, MD); White River Family Practice, White River Junction, Vt (Thomas Parrott, MD, Julie Davis, MD, Michael Lyons, MD, Angela Toms, MD); Eastern Maine Medical Center–Family Practice Residency, Bangor, Me (Kathryn Bourgoin, MD, William Breen III, MD, Eric Brown, MD, Lisa Buck, MD, Greg Carroll, DO, Alden Forrester, MD, Daniel Gott, DO, Ken Johnson, DO, Haresh Kathard, MD, Colleen McCreery, DO, Peter Millard, MD, Srinivas Nimmagadda, MD, Jeffrey Petersen, MD, Robin Prithan, MD, Georg Rymph, MD).
- Received for publication September 7, 2005.
- Revision received December 12, 2005.
- Accepted for publication January 10, 2006.
- © 2006 Annals of Family Medicine, Inc.
REFERENCES




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Patient reported outcome measures in practice
- Integrating Psychosocial Care Into Cancer Services
- Evaluative Criteria for Qualitative Research in Health Care: Controversies and Recommendations
- On TRACK: 'Allows Readers and Authors to Go One Step Further'
- In this Issue: Mixed Methods and Diverse Perspectives