
Abstract
PURPOSE Understanding patients’ perspectives and readiness regarding deprescribing—a concept broader than mere drug cessation, encompassing dynamic interaction between patients and health care professionals—is essential for developing feasible and effective deprescribing interventions. The goal of our study was to qualitatively explore the perspectives of older adults regarding proactive deprescribing, as well as its barriers and enablers.
METHODS We conducted semistructured interviews with 20 patients in Japan aged 65 years or older who were receiving 5 or more regular medications to explore their perceptions and experiences related to deprescribing. The interviews were transcribed and the data were thematically analyzed to identify major concepts.
RESULTS Placing a low value on medication was an important trigger of patients’ proactive attitudes toward deprescribing. Patients were open to deprescribing conversations if they trusted the prescriber. Conversely, patients who had a positive perspective on medication or considered themselves incapable of participating in decision making preferred to defer to a physician. On the basis of medication valuation, decision-making preferences, and openness to deprescribing, we developed a new typology with 5 types of patients: indifferent (15% of study patients), satisfied and risk-averse (10%), compliant (30%), fearful but passive (20%), and proactive (25%).
CONCLUSIONS Patients’ attitudes toward deprescribing varied considerably according to their medication valuation, preference for involvement in decision making, and openness to deprescribing. Focusing on patients’ proactiveness and understanding these barriers and enablers is essential for patient-centered decision making and for developing strategies to optimize the appropriateness of medication.
- polypharmacy
- deprescribing
- potentially inappropriate medication
- chronic illness
- aged
- patient-centered care
- decision making
- physician-patient relationship
- primary care
INTRODUCTION
The concept of deprescribing is broader than simply drug cessation and encompasses a dynamic interaction between patients and health care professionals.1,2 A recent qualitative study demonstrated that patients reported a lack of clarity about the reasons and goals of deprescribing and a poor understanding of the seriousness of adverse events.3 In addition, in a recent meta-analysis, 87.6% of patients and 74.8% of caregivers were willing to deprescribe if their physicians suggested doing so.4 It is therefore important for prescribers to be aware of interest in deprescribing and the need to initiate conversations with patients and families.
Nevertheless, deprescribing is still an event that occurs in the interaction between the patient and the health care professional, and the patient has the right to make final decisions. Understanding the perspectives of patients toward deprescribing, as well as the barriers to and enablers of deprescribing in day-today practice is therefore essential to develop feasible and effective deprescribing interventions.
Previous studies have illustrated several barriers to and facilitators of deprescribing among patients and their caregivers.5-12 Among these studies, Weir et al8 classified patients into 3 types according to their attitudes toward medicines, preferences for involvement in decision making, and openness to deprescribing. Although this typology includes the concept of patients’ proactiveness, the focus is primarily on patients’ willingness to deprescribe when guided by health care professionals, with less focus on proactively initiating such conversations. A specific focus on patient proactiveness—characterized by active involvement and readiness to initiate deprescribing—remains underexplored. Understanding the factors that shape proactiveness could provide valuable insights into its role in patient-centered decision making and optimizing deprescribing practices.
In addition, understanding what makes patients proactive may be vital in optimizing medication management. Little is known, however, about the specific characteristics that drive proactiveness or whether approaches to deprescribing should be tailored to such characteristics. To address this gap, this study aimed to qualitatively explore the experiences and perspectives of older adults on proactive deprescribing, as well as barriers to and enablers of proactive deprescribing.
METHODS
Study Design, Setting, and Participant Selection
From March 2023 to March 2024, we conducted a qualitative study with outpatients aged 65 years or older who visited either a primary care group practice or a community hospital in Kanagawa, Japan, and had prescriptions for at least 5 regular medications. Patients were recruited in person by research staff not involved in the direct clinical care of the patients. The study was approved by the Institutional Ethical Committee of St Marianna University School of Medicine (No. 5593; date of approval: June 1, 2022).
Data Collection
A research coordinator or the principal investigator (K.I.) assessed the eligibility of patients who visited the study sites and obtained written consent. Before the interview, we collected participants’ age, sex, activities of daily living, number of regular medications, and number of potentially inappropriate medications (PIMs) based on the 2023 Beers Criteria of the American Geriatrics Society.13 For medications, we included only prescribed oral medications with a documented prescription duration of 28 days or longer.
Two authors previously unknown to the patients (K.I. and R.M.) conducted semistructured in-depth interviews in Japanese, following an interview guide specifically developed for this study (Supplemental Appendix). The guide was based on previous studies7,9,10 and on research team discussions regarding relevant views and experiences of patients: (1) their thoughts on their health problems and prescriptions, (2) their experience with deprescribing interventions and their degree of involvement in the decision making, and (3) how the experience of deprescribing has affected their subsequent life, health, and perspectives.
We conducted individual interviews in private spaces at the research sites. The semistructured interviews were recorded and lasted approximately 20 to 30 minutes, with a mean (SD) duration of 22.6 (11.0) minutes. Verbatim transcripts were prepared and personally identifiable information was removed.
Analysis
The qualitative analysis in this study applied a deductive-inductive approach following methods used by Hahn et al3 and Heser et al.5 Thematic analysis was conducted following the framework of Braun and Clarke,14 which provides a systematic process for identifying, analyzing, and reporting patterns within data. The structure of the codebook, which guided the thematic analysis, included categories, themes (divided into enablers and barriers), and subthemes to provide clarity and organization. The interview transcripts were independently read and coded by 2 authors (K.I. and R.M.), focusing on salience, frequency, and elaboration of themes. The same authors collaboratively developed the codebook in Japanese through iterative discussions after each round of interviews. During initial codebook development, concordance between these 2 authors was assessed, yielding a rate of 78.3%. Disagreements among coders were discussed to reach consensus, and any discrepancies were resolved through group discussions.
After consensus on the codebook was reached, a native Japanese speaker with advanced proficiency in English (K.I.) translated the themes, subthemes, and quotations into English. The translated content was reviewed by the research team. Enrollment continued until theoretical saturation was reached, consistent with the emphasis of LaDonna et al15 on theoretical sufficiency as a marker of rigor in qualitative research, which we ensured by defining a focused aim, conducting iterative analysis, and refining codes through ongoing discussions.
Through inductive conceptualization, participants were categorized according to their medication valuation (positive, negative, or indifferent), decision-making preference (proactive or passive), and openness to deprescribing (open or cautious), partly referring to the typologies developed by Crutzen et al6 and Weir et al,8 which classify patients based on their attitudes and behavior toward medications. Two authors (K.I. and R.M.) independently conducted this categorization, and consensus was reached through discussion among the research team. Another author (S.M.A.), who has expertise in anthropology and public health, repeatedly reviewed the study process and the conceptual model for triangulation.
RESULTS
We conducted in-depth interviews with 20 patients. Their characteristics are shown in Table 1. Eleven were female. The mean (SD) age was 80.2 (6.2) years. The mean (SD) number of medications was 7.9 (2.7), and the mean (SD) number of PIMs according to the 2023 Beers Criteria13 was 1.0 (0.8).
Characteristics of Patient Participants (N = 20)
The interviews revealed varying levels of familiarity with deprescribing among the patients. They uncovered 3 enablers and 3 barriers with respect to patient perspectives regarding medicines and attitudes toward deprescribing (Table 2), which were organized under headings informed by the categories proposed by Weir et al.8 These categories provided a framework for structuring the results.
Barriers to and Enablers of Proactive Deprescribing Among Adults Aged ≥65 Years
Category 1. Medication Valuation
Theme 1-1. Negative Valuation of Medication (Enabler)
A positive attitude toward deprescribing was driven by patients’ awareness of the burden of polypharmacy, the potential risks associated with medications, and previous successful experiences with stopping medications. Placing a negative value on medication was an important factor in fostering these patients’ consideration of deprescribing.
There were 4 subthemes pertaining to the theme of negative valuation of medication: perceived burden of polypharmacy, fear that medication may cause harm, lack of perceived benefits, and experience of successful deprescribing.
Theme 1-2. Positive Perspective on Medication (Barrier)
Patient satisfaction with the status quo hindered deprescribing, as patients were content with their current medications. Others felt distressed by their multiple illnesses but still saw medication adherence as part of their health-promoting behavior. The fact that a health care professional supervised the drug therapy reassured these individuals. Consequently, patients who had a positive medication valuation or concerns about symptom deterioration due to deprescribing were more cautious about a medication change. This theme aligns with prior typologies, including “attached to medicine” as described by Weir et al8 and “positive opinion about medication and unwilling to stop” as described by Crutzen et al,6 reflecting patients’ reliance on prescriber recommendations and satisfaction with current treatments.
There were 2 subthemes pertaining to the theme of a positive perspective on medications: acceptance of the current situation through trust in the prescriber and high expectations for medications.
Category 2. Decision-Making Preference
Theme 2-1. Proactive Decision-Making Involvement Preference (Enabler)
A few patients who demonstrated high levels of proactiveness not only sought to understand their health status and treatment options through conversation with their prescribers, but also took the initiative to discuss deprescribing, reflecting their active engagement in decision making. These patients were motivated to improve their health by taking control of modifiable factors, for example, through lifestyle modifications.
There were 2 subthemes pertaining to the theme of a preference for proactive decision-making involvement: a preference for patient-centered decision making about medicines and motivation for disease control through lifestyle modification.
Theme 2-2. Passive Patient Involvement and Perceived Lack of Capability (Barrier)
In contrast to the proactive patients, a larger group of patients had a passive attitude toward deprescribing. They preferred to defer decision making to their physicians, even if they remained on multiple medications, and were content to take their medications as prescribed without question. Several patients believed it was wrong for a patient to ask their physician to deprescribe, based on the notion that prescribing is the physician’s job and that patients have no expertise in the medical field. This theme corresponds to “defers to others” as described by Weir et al8 and “negative/ambivalent opinion about medication and willing to stop” as well as “indifferent towards medication and stopping” as described by Crutzen et al,6 highlighting patients’ preference to defer decisions to physicians and a perceived lack of capability to initiate deprescribing.
There were 3 subthemes related to the theme of passive patient involvement and perceived lack of capability: preference of deferring decision to the prescriber, difficulty in expressing opinions due to reticence toward the physician, and perceived lack of capability to deprescribe.
Category 3. Openness to Deprescribing
Theme 3-1. Openness to a Deprescribing Proposal Based on Trust in Prescriber (Enabler)
Trust in prescribers played a considerable role in shaping older adults’ medication beliefs. Some patients were receptive to deprescribing when their physicians supported it. This attribute could also be a barrier, however, because the patient may not have been interested in deprescribing if his or her physician continued the current prescription. This theme partially overlaps with the “would consider deprescribing” of Weir et al8 and the “positive opinion about medication but willing to stop” of Crutzen et al,6 emphasizing the role of trust in prescribers in shaping openness to deprescribing.
There were 2 subthemes related to the theme of openness to a deprescribing proposal based on trust in one’s prescriber: trust in the prescriber and openness to deprescribing if suggested by prescriber.
Theme 3-2. Caution Due to Fear of Change or Satisfaction With the Status Quo (Barrier)
Some patients were not receptive to their physician’s deprescribing suggestions because they were satisfied with their current condition and they had concerns about symptoms worsening if they discontinued their medications.
There were 2 subthemes related to this theme: fear of changing current medications and satisfaction with the status quo.
Typology
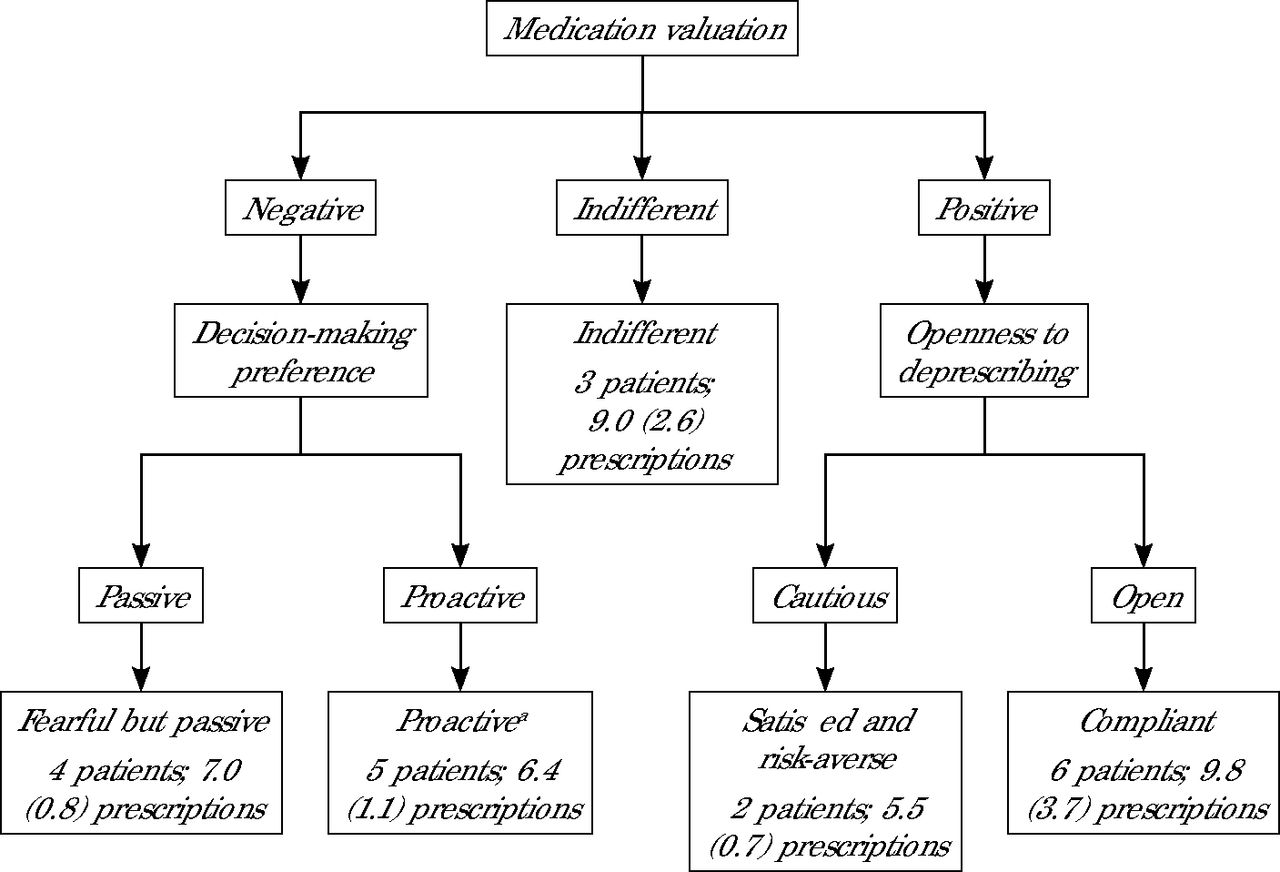
On the basis of the main themes identified from the interviews, we focused on patients’ medication valuation, decision-making preference, and openness to deprescribing, which resulted in 5 typologies partly related to those of Weir et al8 and Crutzen et al6: indifferent (3 patients, 15%), satisfied and risk-averse (2 patients, 10%), compliant (6 patients, 30%), fearful but passive (4 patients, 20%), and proactive (5 patients, 25%) (Figure 1 and Supplemental Table 1).

Patient Typology Based on Attitudes Toward Medication, Willingness to Deprescribe, and Proactiveness to Initiate a Conversation About Deprescribing
Note: Number of prescriptions is the mean (SD) number per patient.
a All proactive patients had a negative medication valuation and an openness to deprescribing.
These 5 patient types represent a synthesis of our findings on enablers and barriers. Although they draw partly on the classifications by Weir et al8 and Crutzen et al,6 the inclusion of a proactive type is an original contribution to the understanding of patient perspectives on deprescribing. All patients who were categorized as proactive placed a negative value on medication, suggesting that unfavorable perspectives on medication may be an essential trigger of patients’ proactive attitudes toward deprescribing, and also had an openness to deprescribing.
The most frequent patient type was compliant, characterized by positive attitudes toward medications but also a willingness to deprescribe if it was recommended by their prescriber (Figure 1). Although numbers of patients were too small for meaningful comparisons, the mean (SD) number of prescriptions per patient was numerically higher in the compliant group, at 9.8 (3.7), and the indifferent group, at 9.0 (2.6), and lower in the satisfied and risk-averse group, at 5.5 (0.7), and the proactive group, at 6.4 (1.1).
DISCUSSION
Overall, our older adult patients taking multiple medications had widely diverse perspectives on deprescribing. Although many described situations wherein health care professionals initiated deprescribing conversations, a subset of patients reported proactively seeking deprescribing discussions with their clinicians, reflecting varied levels of patient engagement and initiative. A minority of patients demonstrated proactiveness in understanding their health status and treatment options through dialog with their prescribers and aimed to take control of modifiable factors such as making lifestyle changes. Their positive attitudes were driven by an awareness of the medication burden, potential risks, and past successful deprescribing experiences, with trust in their physicians being crucial for their decision making. Conversely, a larger group preferred to defer decisions to their physicians, influenced by trust in their prescribers, satisfaction with current prescriptions, and a perceived lack of capability to make treatment decisions. This group was more cautious about medication change because they held a positive medication valuation or had concerns about symptom deterioration.
Findings in Context
Previous studies have suggested a potential association between patient proactiveness and views of the value of medication.6,12 In our study, all patients categorized as proactive had a negative opinion about medications. Although further studies are required to examine the associations, we hypothesize that a patient’s medication valuation may play a vital role in being proactive when it comes to decision making about deprescribing.
A perceived lack of capability to understand and participate in decision making is a known barrier to deprescribing.16 Individuals who perceived themselves as lacking decision-making capabilities, partly because of older age and multiple comorbidities, may have unrealistic expectations for medication adherence as a self-promoting behavior. Motivational interviewing, a collaborative communication style, could help address these challenges by fostering a patient’s self-efficacy and supporting informed decision making.17 Evidence shows that motivational interviewing enhances behavioral change by building confidence in taking actionable steps.18 On the basis of our findings, we hypothesize that motivational interviewing could encourage proactiveness in patients hesitant to initiate deprescribing discussions. Future research may explore the potential of motivational interviewing–based tools to strengthen a patient’s confidence and support a more patient-centered approach to deprescribing.
Positive medication valuation and satisfaction with the existing regimen were common among some patients, reflecting their comfort with prescribed medications and their trust in the current treatment plan. Antonovsky19 introduced the concepts of sense of coherence and health resources within the framework of salutogenesis. These concepts involve behaviors that form “the self” within daily routines. It is possible that satisfaction with the status quo may reflect the older adult’s sense of coherence through being adherent to prescribed medications. It is therefore likely that there is a group of older adults for whom uniform deprescribing could impact their well-being by bringing about changes in their sense of coherence.
Our results are consistent with those of prior work that emphasized the importance of the health care professional initiating the deprescribing conversation.2 Notably, even patients who are positive about their medications or reluctant to ask their prescribers to deprescribe are often willing to stop a medication if the prescriber recommends doing so. This receptiveness suggests that the prescriber should raise the topic even if the patient seems content with the current medication.
Compared with the previous typologies defined by Weir et al8 and Crutzen et al,6 our typology explicitly focuses on patient proactiveness in deprescribing decision making, extending beyond the willingness to deprescribe, which typically requires a recommendation from health care professionals. We believe that proactiveness toward deprescribing, as highlighted in our study, represents an important factor that has not been sufficiently explored. For instance, patients categorized as proactive may benefit from shared decision-making models that provide more control over medication choices, whereas patients categorized as satisfied and risk-averse or as compliant may require more prescriber-led conversations to explore deprescribing options. Future studies should focus on gaining a deeper understanding of the processes that foster proactiveness and develop interventions that effectively promote it.
Strengths and Limitations
Our results can inform deprescribing frameworks applicable across diverse health care settings. By using strategies to ensure rigor, such as triangulation across different levels—including multiple investigators, a combination of inductive and deductive methods, and a sample with representation of both clinic and hospital patients—we aimed to enhance the trustworthiness of our findings. Furthermore, we included patients with negative perspectives on deprescribing, allowing for greater variability in attitudes and abilities and thereby supporting the credibility of our interpretations.
Study limitations include the following. We used 5 or more regular medications as an inclusion criterion; hence, the perspectives of adults aged ≥65 years who are proactive in avoiding polypharmacy may not be reflected. By recruiting from both primary care and hospital settings, we aimed to enhance the diversity of perspectives; however, cultural factors unique to Japan, such as high trust in health care professionals and the societal emphasis on medication adherence, may have influenced patients’ attitudes toward deprescribing. These cultural variables should be considered when interpreting our findings and assessing their potential applicability to other regions or health care systems.
Conclusions
This study reveals that older adults’ readiness for deprescribing is influenced by their medication valuation, decision-making preferences, and openness to change, and combinations of these attributes can be used to define 5 distinct patient types. Our findings underscore the importance of tailoring deprescribing interventions to the individual patient’s perspective and level of proactiveness. Future research should investigate how patient categorization according to this typology impacts long-term health outcomes and medication adherence after deprescribing interventions. Additionally, studies examining strategies to enhance patient education and self-efficacy among those less open to deprescribing could further inform best practices for reducing polypharmacy in older adults.
Acknowledgments
The authors acknowledge the work of research assistants Junko Mita and Maki Matsui for their assistance with data collection and support of this research. We would like to thank Dr Yasuki Fujinuma for introducing important ideas related to salutogenesis in “An Introduction to Excellent Generalist Practice: Methods for Clinicians in a Complex and Challenging Era,” which provided valuable insights for our discussion. We would also like to extend our sincere appreciation to all the participants.
Footnotes
Conflicts of interest: authors report none.
Funding support: This study was funded by research grants from the Japanese Ministry of Health, Labour and Welfare (grant number 22K15678).
Disclaimer: The views expressed are solely those of the authors and do not necessarily represent official views of the authors’ affiliated institutions or the funder.
Previous presentation: This study was presented at the 2024 Society of General Internal Medicine Annual Meeting; May 17, 2024; Boston, Massachusetts.
Reporting guidelines and/or checklist: This study adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines, encompassing reporting elements including study methods, study context, findings, analysis, and interpretations [COREQ]. Detailed responses to each of the 32 items outlined in the COREQ framework are provided in Supplemental Table 2.
Related previously published research by the authors: Ie K, Machino R, Albert SM, Tomita S, Kushibuchi M, Hirose M, Matsuda T, Okuse C, Ohira Y. Deprescribing as an opportunity to facilitate patient-centered care: a qualitative study of general practitioners and pharmacists in Japan. Int J Environ Res Public Health. 2023; 20(4): 3543. doi:10.3390/ijerph20043543
- Received for publication August 1, 2024.
- Revision received December 12, 2024.
- Accepted for publication January 6, 2025.
- © 2025 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.