
Abstract
PURPOSE Peer support intervention trials have shown varying effects on glycemic control. We aimed to estimate the effect of peer support interventions delivered by people affected by diabetes (those with the disease or a caregiver) on hemoglobin A1c (HbA1c) levels in adults.
METHODS We searched multiple databases from 1960 to November 2015, including Ovid MEDLINE, the Cochrane Central Register of Controlled Trials, CINAHL, and Scopus. We included randomized controlled trials (RCTs) of adults with diabetes receiving peer support interventions compared with otherwise similar care. Seventeen of 205 retrieved studies were eligible for inclusion. Quality was assessed with the Cochrane risk of bias tool. We calculated the standardized mean difference (SMD) of change in HbA1c level from baseline between groups using a random effects model. Subgroup analyses were predefined.
RESULTS Seventeen studies (3 cluster RCTs, 14 RCTs) with 4,715 participants showed an improvement in pooled HbA1c level with an SMD of 0.121 (95% CI, 0.026–0.217; P = .01; I2 = 60.66%) in the peer support intervention group compared with the control group; this difference translated to an improvement in HbA1c level of 0.24% (95% CI, 0.05%–0.43%). Peer support interventions showed an HbA1c improvement of 0.48% (95% CI, 0.25%–0.70%; P <.001; I2 = 17.12%) in the subset of studies with predominantly Hispanic participants and 0.53% (95% CI, 0.32%–0.73%; P <.001; I2 = 9.24%) in the subset of studies with predominantly minority participants; both were clinically relevant. In sensitivity analysis excluding cluster RCTs, the overall effect size changed little.
CONCLUSIONS Peer support interventions for diabetes overall achieved a statistically significant but minor improvement in HbA1c levels. These interventions may, however, be particularly effective in improving glycemic control for people from minority groups, especially those of Hispanic ethnicity.
INTRODUCTION
The global burden of diabetes is expected to increase from 381.8 million people affected in 2013 to an estimated 591.9 million by 2035.1 Despite increasing evidence of benefits from self-management education, only 5% of Medicare-insured and 7% of privately insured people with diabetes receive this intervention within 1 year of diagnosis.2–4 Diabetes self-management education improves hemoglobin A1c (HbA1c) levels, and longer duration of education further lowers levels; however, the benefits decline 1 to 3 months after education ends.5
The World Health Organization (WHO) has stated that peer support appears to be a promising approach to improving and sustaining diabetes self-management behaviors.6 Randomized controlled trials (RCTs) using peer support interventions delivered by people affected by diabetes have shown varying results on glycemic control, however. A 2012 narrative review examined the effect of peer support interventions on diabetes outcomes, but several additional studies with these interventions have been published in the last 3 years.7 One recent meta-analysis looked at peer support for improving glycemic control, yet this analysis included trials with community health workers and bilingual clinic employees as peer health coaches and was missing a few intervention trials that used people affected by diabetes as peer supporters.8 Hence, to date, there has not been an adequate systematic review and meta-analysis of the overall effectiveness of peer support interventions delivered by people affected by diabetes to inform policy or potential health care delivery changes.
We therefore performed a systematic review and meta-analysis of RCTs to assess the effectiveness of peer support interventions on improving glycemic control in adults with diabetes as measured by HbA1c levels compared with counterparts who received otherwise similar care except for the peer-delivered interventions. The American Academy of Family Physicians (AAFP) program Peers for Progress defines peer support as “support from a person who has knowledge from their own experiences with diabetes, a person with diabetes, or a person affected by diabetes (eg, immediate family member or caregiver).”9 We used this definition in our study as our goal was to estimate the effect of training and engaging people affected by diabetes to improve glycemic control of others affected by the disease. Qualitative evaluations have suggested that being a peer supporter makes people feel more empowered to manage their own diabetes.10 Hence, peer support interventions delivered by affected individuals seems like a promising method to engage primary stakeholders in their diabetes self-management.
METHODS
We used the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement along with the PRISMA explanation and elaboration document to report our findings.11 Methods of analysis, inclusion criteria, outcome of interest, and data extraction were predefined.
Search Strategy and Study Selection
We included only RCTs that compared peer support interventions with otherwise similar care in adults with diabetes that measured HbA1c level as a primary or secondary outcome. We allowed any duration of follow-up. As noted above, the AAFP Peers for Progress definition was used to define peer support as support from a person with or affected by diabetes.9 Any peer-delivered interventions designed to improve self-management or health behaviors, or to provide emotional or social support with the goal of improving overall health were eligible. We included studies if both the peer intervention group and the control group received similar baseline education from diabetes educators and similar baseline care management from health care professionals.
To avoid contamination of the peer support intervention effect, we excluded studies providing additional health professional–delivered intervention or education other than that provided by peers in the intervention group compared with the control group; also excluded were studies of support groups or peer interactions facilitated by professionals other than peer supporters. We additionally excluded studies comparing a peer-delivered intervention with an identical one delivered by other community or health professionals, as the goal of this analysis was to look at the additional effect on glycemic control of peer-delivered interventions compared with otherwise similar care.
Data Sources
We searched English and non-English articles from January 1960 through November 2015 using Ovid MEDLINE, the Cochrane Central Register of Controlled Trials, the Cochrane Database of Systematic Reviews, CINAHL, PsycINFO, Scopus, OCLC First Search, ProQuest Dissertations & Theses A&I, BioOne Abstracts and Indexes, Social Service Abstracts, and Sociological Abstracts. Groups of search terms included diabetes mellitus; HbA1c; peer support, peer educator, peer coach; promotora; and RCT. (See Supplemental Appendix A1 for the detailed search strategy for MEDLINE, http://www.annfammed.org/content/14/6/540/suppl/DC1.)
We also conducted searches of Scopus, CINAHL, PsycINFO, and Google Scholar for eligible studies by authors with known expertise in peer support research. We reviewed the AAFP Peers for Progress website, the WHO statement on peer support in diabetes management, and references in published articles for any additional studies. Authors of eligible conference submissions identified through the OCLC PapersFirst database were contacted for further information to ascertain whether their study met our inclusion criteria. Two reviewers (S.J.P. and R.J.K.) independently screened citations, and all selections were reviewed by 2 additional reviewers (T.R. and V.S.C.) to confirm their suitability.
Quality Assessment
Two authors (S.J.P. and E.J.L.) assessed study quality independently using the Cochrane Collaboration’s risk of bias tool and checked for interrater comparability.12 Only trials reporting HbA1c level as an outcome were included in this review; hence, the risk of selective data reporting was considered minimal.
Data Extraction
A codebook was created before data extraction to include all variables of interest and predefined subgroups by 1 author (S.J.P.) and was reviewed by 3 other authors (E.J.L., T.R., and V.S.C.). Data were extracted independently by 2 authors (S.J.P. and E.J.L.) who discussed all disagreements and resolved them to achieve 100% consensus. One additional author (T.R.) confirmed the extraction accuracy of numerical outcome data.
We extracted data on study setting and multiple participant and peer characteristics. For intervention characteristics, we extracted method of intervention, planned sessions, number of successful intervention contacts, hours of training for peer supporters, and components of the peer support intervention. We coded peer supervision as present if the peer-delivered sessions were observed or recorded, if participants’ knowledge was assessed after peer supporters delivered education sessions, if a contact log between peer supporters and participants was maintained, if calls were recorded, or if participants were contacted to determine whether peer supporters had been in contact with them. Support and guidance for peer supporters was not coded as peer supervision. If necessary information was not reported in published articles, we contacted authors to obtain it. We extracted HbA1c values and measures of statistical variation at baseline and at study conclusion.
Data Synthesis and Analysis
Statistical analysis was performed using Comprehensive Meta-analysis Software version 3 (Biostat Inc). We calculated the standardized mean difference (SMD) in changes from baseline HbA1c level to end-of-study level between the peer support intervention and control groups to adjust for varying baseline HbA1c level. If reported, intention-to-treat data were used without adjusting for missing data or losses to follow-up. To compute effect sizes, we used the random-effects model of DerSimonian and Laird,13 as it provides more conservative estimates by incorporating both within- and between-study variation. We calculated an SMD effect size (Cohen d), which reflects the difference in means between treatment and control participants in terms of their shared SD.14 We calculated 95% CIs, and we considered a P value of <.05 statistically significant for all analyses other than the Q statistic. Corrected sample size was calculated for cluster randomized trials using the documented intracluster coefficient.15 We assumed a correlation coefficient of 0.5 between initial and final values as recommended by Follmann and colleagues.16 Heterogeneity among studies was evaluated by the Q statistic with a P value of <.10 indicating heterogeneity and by the I2 statistic. I2 values of less than 40% may indicate insignificant heterogeneity; 30% to 60% may indicate moderate heterogeneity; 50% to 90% may indicate substantial heterogeneity; and 75% to 100% indicates considerable heterogeneity.17
Using analysis of variance (ANOVA) for mixed effects analysis to assess effect sizes, we performed predefined subgroup analyses for studies grouped by predominant participant ethnicity (that seen in ≥50% of participants), predominant participant minority status, peer intervention methods, control group interventions, and presence of peer supervision. The fixed effect Q statistic was used to determine statistical significance of the difference of effects between subgroups.18 We performed metaregression analyses to assess effects of baseline HbA1c level, duration of peer training in hours, and duration of observation on study effect sizes. Publication bias was assessed using a funnel plot and using the Egger regression test.19
RESULTS
Study Selection
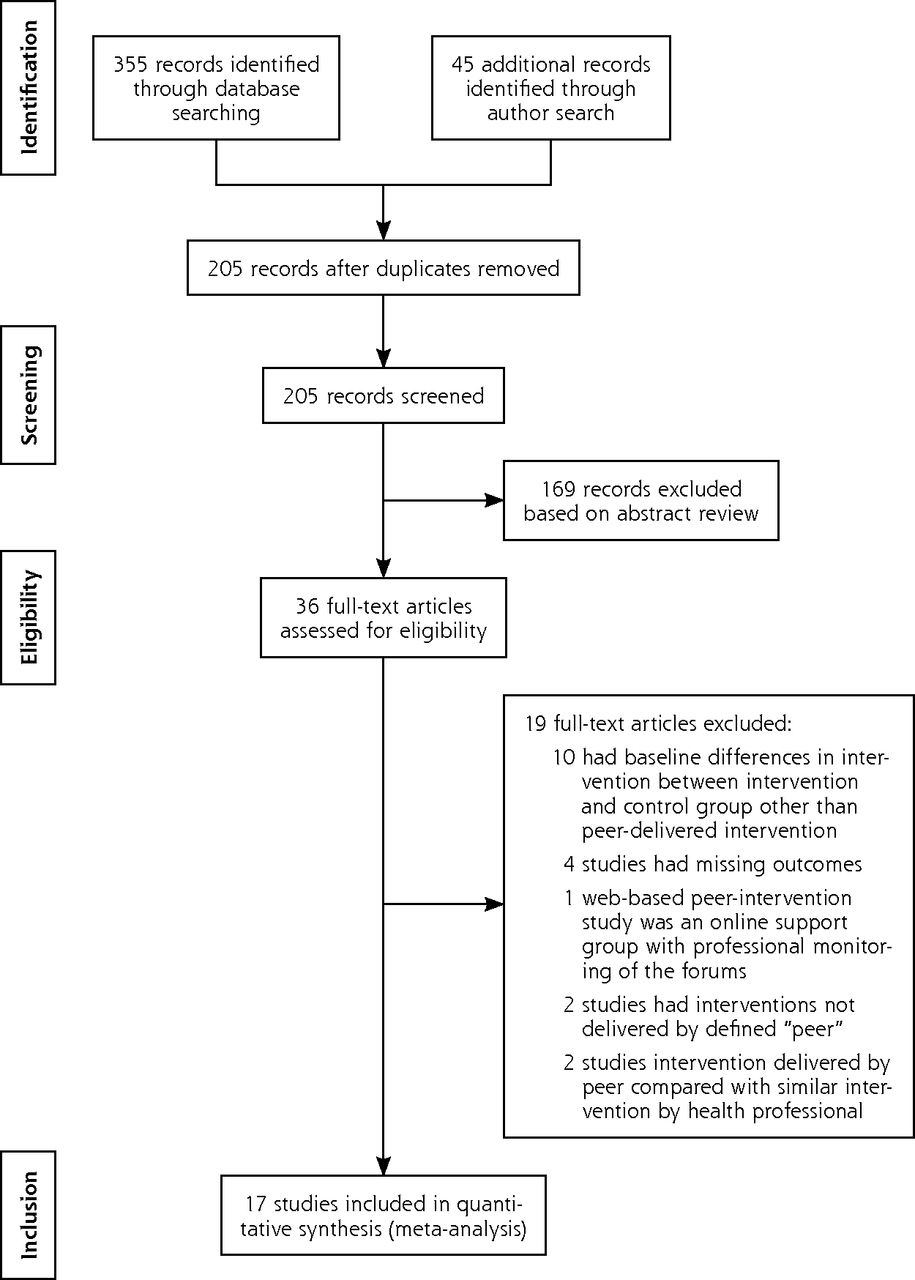
We retrieved 400 citations from our database searches and database author searches. After removing duplicates and reviewing abstracts, we examined 36 full articles. Figure 1 shows the literature search flow diagram and reasons for article exclusions.20 Ultimately, 14 articles with RCT designs and 3 cluster RCTs were eligible for inclusion in the meta-analysis, for a total of 4,715 participants. Of the 17 trials, 10 were done in the United States,21–30 4 in Europe,31–34 1 in Canada,35 1 in China,36 and 1 in Argentina.37 Study characteristics are shown in Table 1. Most of the trials included lifestyle counseling, goal setting, and behavioral and social support as peer support interventions.
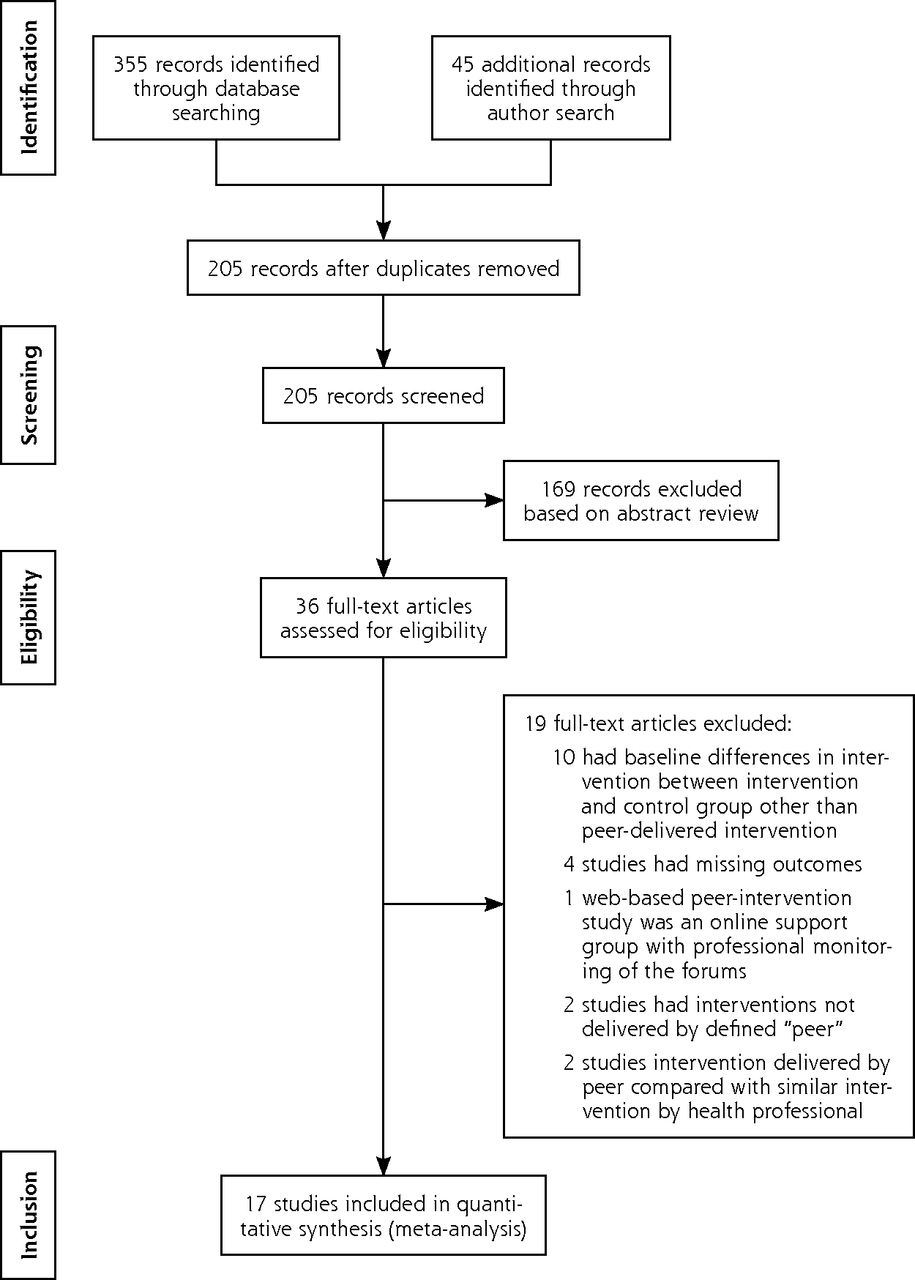
Results of the literature search.
Note: Performed according to methods outlined by Moher et al.20
Descriptive Summary of the Characteristics of Included Studies
Risk of Bias and Publication Bias
An assessment of quality for all included studies is shown in Table 2, with details given in Supplemental Appendix Table A1 (http://www.annfammed.org/content/14/6/540/suppl/DC1). In all but 4 of the 17 trials (23.5%), the dropout rate was less than 20%.21,27,33,35 None of the trials blinded participants, but 3 trials (17%) blinded outcomes assessors or investigators. Allocation concealment was not reported in 3 studies and not done in 1 study. We found no association between quality of studies and outcomes. Neither the funnel plot (Supplemental Appendix Figure A1, http://www.annfammed.org/content/14/6/540/suppl/DC1) nor the Egger regression test (P = .47) suggested publication bias.
Quality of the Included Studies Assessed With the Cochrane Risk of Bias Tool12
Effect on HbA1c Level
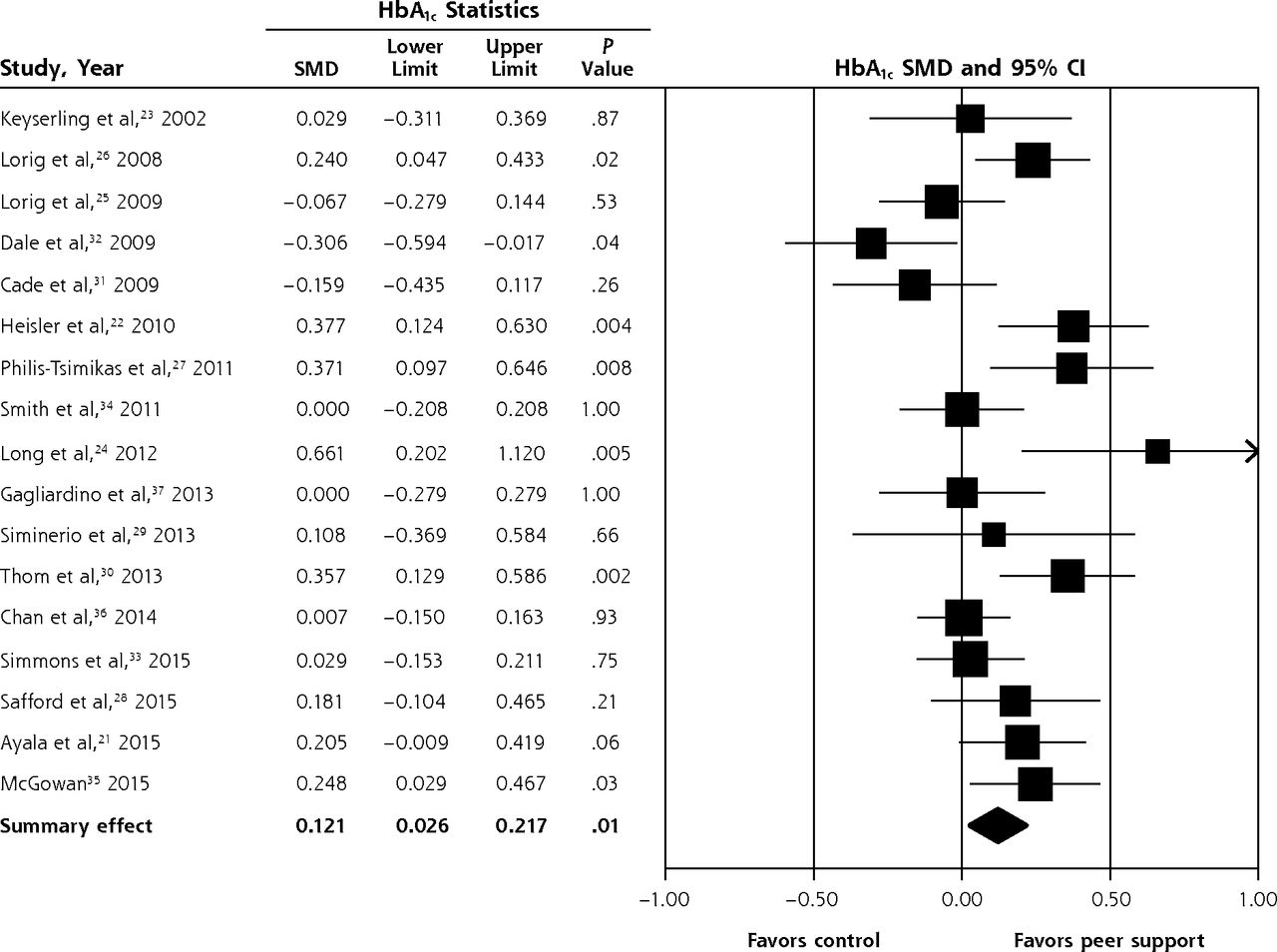
The overall pooled effect of peer support interventions on HbA1c level from the random effects model was an SMD of 0.121 (95% CI, 0.026–0.217; P = .01) (Figure 2). This difference translates to an improvement in HbA1c level of 0.24% (95% CI, 0.05%–0.43%) in peer support intervention groups compared with the control groups, where the pooled mean HbA1c level was 8%. The I2 was 60.66%, indicating moderate heterogeneity. A sensitivity analysis excluding cluster RCTs showed a similar pooled effect, with an SMD of 0.137 (95% CI, 0.021–0.254; P = .02; I2 = 66.03%), which translates to an improvement in HbA1c level of 0.27% (95% CI, 0.04%–0.5%) (Supplemental Appendix Figure A2, http://www.annfammed.org/content/14/6/540/suppl/DC1).

Effect of peer support interventions on hemoglobin A1c levels.
HbA1c = hemoglobin A1c; SMD = standardized mean difference.
Notes: Random effects model. I2 = 60.66%; P for heterogeneity = .001.
Subgroup Analyses
Studies With Ethnic or Racial Predominance
The pooled effect of peer support interventions in the subgroup of 5 studies with predominantly Hispanic participants showed a clinically relevant and statistically significant SMD of 0.241 (95% CI, 0.126–0.355; P <.001; I2 = 17.12%), which translates to an improvement in HbA1c level of 0.48% (95% CI, 0.25%–0.70%) in the peer support intervention group compared with the control group (Figure 3).21,26,27,30,37 In contrast, the pooled effect size from the 7 studies with predominantly white, non-Hispanic participants showed no improvement in HbA1c level with peer support interventions, with an SMD of −0.004 (95% CI, −0.153 to 0.144; P = .95; I2 = 59.41%).22,25,29,31–34 The pooled effect in the subgroup of 3 studies with predominantly African American participants showed a similar effect size to that seen in the Hispanic subgroup but was not statistically significant, with an SMD of 0.25 (95% CI, −0.064 to 0.571; P = .11; I2 = 58.60%).23,24,28 The differences in effect sizes between ethnicity subgroups were statistically significant, with a between-group P value of .03.
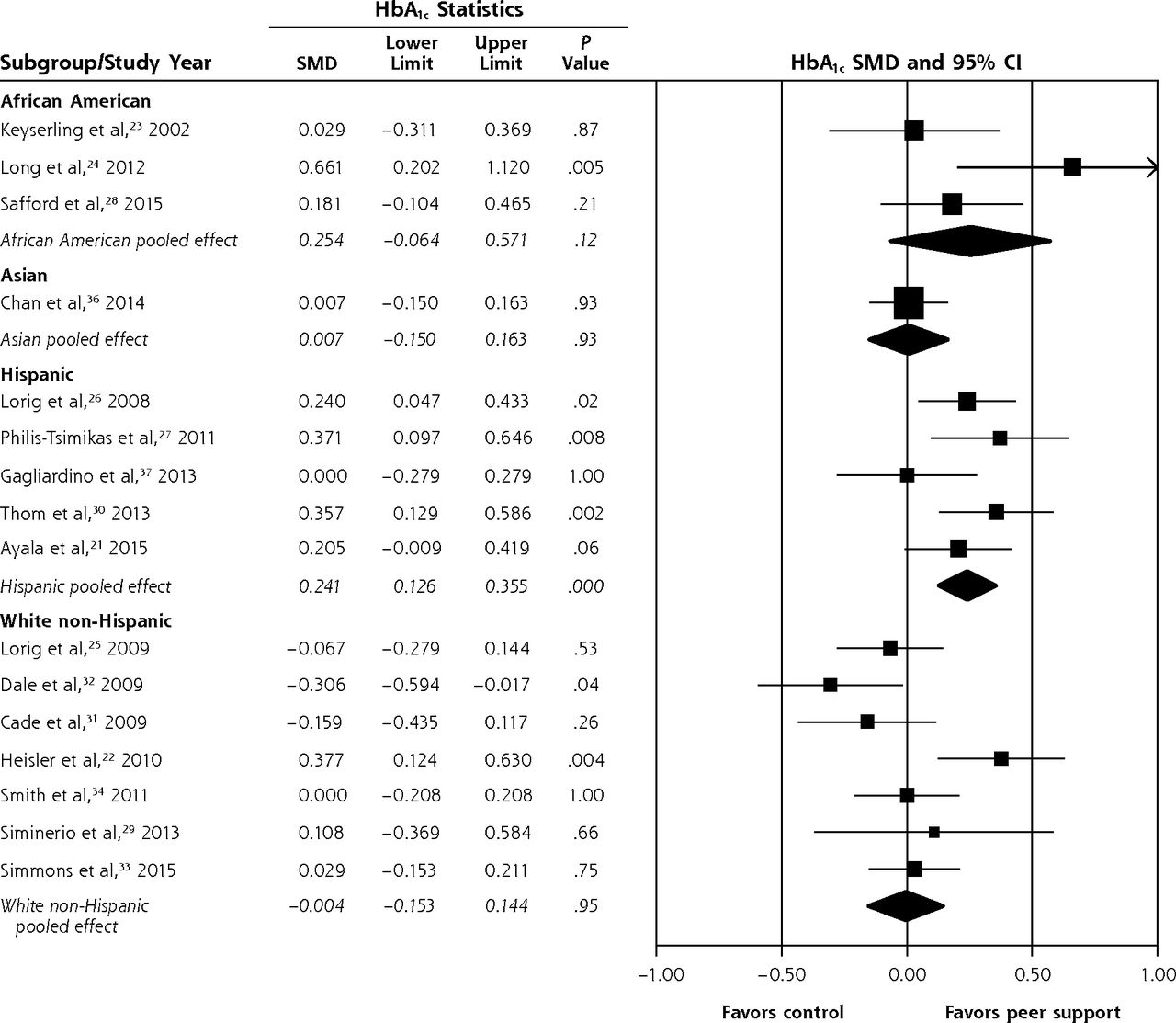
Subgroup analysis of the effect of peer support interventions on hemoglobin A1c levels in studies by predominant race/ethnicity of the participants.
HbA1c = hemoglobin A1c; SMD = standardized mean difference.
Notes: African American subgroup: I2 = 58.60%, P for heterogeneity = .08. Asian subgroup: I2 = 0.00%. Hispanic subgroup: I2 = 17.12%, P for heterogeneity = .30. White non-Hispanic subgroup: I2 = 59.41%, P for heterogeneity = .02.
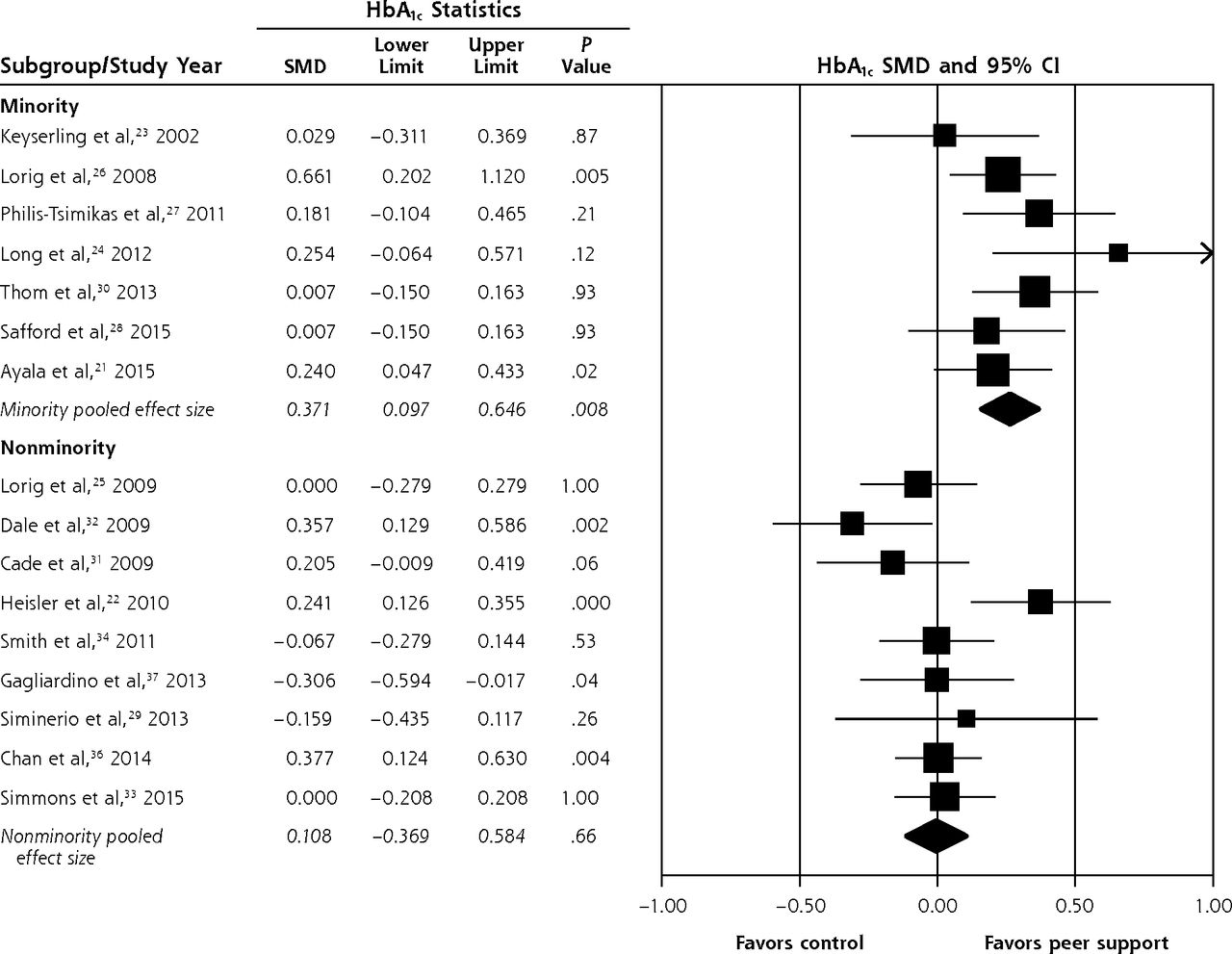
Considering together the 7 studies with predominantly minority participants (belonging to minority culture in the country of residence), the pooled effect showed a clinically relevant improvement in HbA1c level with peer support interventions, with an SMD of 0.266 (95% CI, 0.163–0.369; P <.001; I2 = 9.24%), which translates to improvement in HbA1c level of 0.53% (95% CI, 0.32%–0.73%) (Figure 4). In the 9 studies with predominantly nonminority participants, the pooled effect size showed no improvement in HbA1c level with peer support interventions, with an SMD of −0.002 (95% CI, −0.109 to 0.106; P = .97; I2 = 45.90%). The between-group difference based on minority status was statistically significant, with a P value of .001. One study did not report the ethnic distribution of its participants34 and was excluded from the ethnicity- and minority-based subgroup analysis.

Subgroup analysis of the effect of peer support interventions on hemoglobin A1c levels in studies by predominant minority status of the participants.
HbA1c = hemoglobin A1c; SMD = standardized mean difference.
Notes: Minority subgroup: I2 = 9.24%, P for heterogeneity = .35. Nonminority subgroup: I2 = 45.90%, P for heterogeneity = .06.
Studies With Baseline Education or Care Management
In 5 studies, both control and intervention groups received diabetes education classes or care management at baseline. The pooled effect from these studies showed no improvement in HbA1c level with peer support interventions, with an SMD of 0.041 (95% CI, −0.072 to 0.153; P = .47; I2 = .00%) (Supplemental Appendix Figure A3, http://www.annfammed.org/content/14/6/540/suppl/DC1). In the 12 studies in which control groups received usual care, however, peer support interventions led to a significant improvement in HbA1c level, with an SMD of 0.147 (95% CI, 0.021–0.273; P = .02; I2 = 70.53%), which translates to an improvement in HbA1c level of 0.29% (95% CI, 0.04%–0.54%). The between-group differences in subgroups by baseline intervention, however, was nonsignificant, with P = .22. There was no difference in improvement in HbA1c level among subgroups based on the method used to deliver the peer intervention (group education, telephone delivery, or a combination of both) (Supplemental Appendix Figure A4, http://www.annfammed.org/content/14/6/540/suppl/DC1). The pooled effect of 11 studies using peer supervision as defined in the data extraction section showed a significant improvement in HbA1c level with peer support interventions, with an SMD of 0.143 (95% CI, 0.050–0.237; P = .003; I2 = 43.25%), which translates to an improvement in HbA1c level of 0.28% (95% CI, 0.099%–0.47%). In contrast, the pooled effect from 8 studies without peer supervision did not show an improvement in HbA1c level with peer support interventions, with an SMD of 0.078 (95% CI, −0.157 to 0.313; P = .52; I2 = 77.09%), and there was a nonsignificant between-group P value of .61 (Appendix Figure A5, http://www.annfammed.org/content/14/6/540/suppl/DC1).
Self-Efficacy Outcomes
Six studies measured self-efficacy outcomes using diverse scales; hence, the interaction between these outcomes and HbA1c levels could not be summarized quantitatively. Two of the 3 studies that showed a significant improvement in self-efficacy outcomes with peer support interventions also showed an improvement in HbA1c level with these interventions.25,26,35 Three studies that did not show any significant improvements in self-efficacy outcomes with peer support interventions did not demonstrate improvements in HbA1c levels with the interventions.31–33
Metaregression analysis did not show any interaction between the duration of peer training in hours (Supplemental Appendix Figure A6, http://www.annfammed.org/content/14/6/540/suppl/DC1), mean participant baseline HbA1c level (Supplemental Appendix Figure A7, http://www.annfammed.org/content/14/6/540/suppl/DC1), and the duration of observation (Supplemental Appendix Figure A8, http://www.annfammed.org/content/14/6/540/suppl/DC1) on the change in HbA1c level between the intervention and control groups.
DISCUSSION
Our results show that peer support interventions delivered by people affected by diabetes are associated with a small but statistically significant reduction in HbA1c level of 0.24% (95% CI, 0.05%–0.43%). This finding is comparable to that of a recent Cochrane systematic review and meta-analysis of personalized care planning between clinicians and patients that led to a pooled reduction in HbA1c level of 0.24% (95% CI, 0.14%–0.35%).38 We found that the effect was more clinically relevant in studies with predominantly minority participants, particularly Hispanic participants. A 2014 Cochrane review showed that glycemic control and knowledge of diabetes are improved when culturally appropriate health education is provided to people with diabetes who belong to ethnic minority groups.39 Peer health coaches might be providing more culturally appropriate health education in ethnic minority populations, particularly Latino ones.
Of the 5 studies with predominantly Hispanic populations, 4 were done in the United States and 1 in Argentina. The last was the only one in the subgroup that did not show any effect of peer support interventions on HbA1c levels. This finding encouraged us to look at the subgroup of studies with predominantly minority and nonminority participants based on country of residence.
Caution is needed in interpreting results from the 3 studies done with predominantly African American participants, as these studies had diverse characteristics; 1 study showed improvement in HbA1c level with peer support interventions whereas the other 2 did not. Additional trials with African American participants may further define the effect of peer support interventions in this subgroup. In our analysis, the existing intervention approaches and dosages did not appear to be effective in white non-Hispanic populations, although with moderate heterogeneity of results. A previous subgroup analysis and secondary analysis of RCTs showed that peer support interventions for patients with diabetes are most effective for those having poor self-management skills, poor baseline diabetes support, and lower levelsof health literacy.40,41 Further innovative studies of interventions that sustain self-management behaviors in white non-Hispanic populations targeting high-risk groups with the above-noted characteristics need to be done.
Our subgroup analyses also show that peer support did not produce additional improvement in HbA1c levels when both groups received care management or group education sessions. Other studies comparing similar interventions delivered by peer supporters and other health professionals or community health workers found no significant difference in glycemic control.42–44 In resource-constrained health care settings where care management is not feasible for a larger patient population, peer support interventions might be an effective way of improving diabetes outcomes. Although we were not able to perform a quantitative assessment of the interaction of self-efficacy outcomes and HbA1c outcomes because of the heterogeneity of assessment methods, our qualitative assessment showed that most trials in which peer support improved self-efficacy, HbA1c level improved as well, and conversely, trials without a gain in self-efficacy had no improvement in HbA1c level. It may be that the peer support affects glycemic control through increased self-efficacy.
Our study has limitations. Although significant, the overall improvement in HbA1c level with peer support interventions was small in terms of clinical relevance. Additionally, HbA1c level, an intermediate biochemical marker, was the outcome assessed instead of patient-centered outcomes or clinical outcomes that take years to become apparent. We chose HbA1c level because of the lack of studies reporting those outcomes and the generally short duration of follow-up in most studies. Even though all the included studies were RCTs, participants were not blinded, but blinding would be impossible where participants had to interact with the peer supporters for intervention delivery. Our subgroup analyses showed qualitative interaction between effect sizes and directions for various subgroups; nevertheless, these comparisons were post hoc.45,46 Additionally, meta-analysis of individual patient data would be much better for understanding the subgroup differences than the group-level differences in demographics used in our analysis. Another limitation was that we could not assess the interaction of socioeconomic status with the effect of peer support interventions or estimate cost-effectiveness as there was not enough information given. The included studies were conducted in diverse settings and populations, but most took place in the United States and Europe, which may limit generalizability.
In conclusion, peer support interventions modestly improved HbA1c level, with greatest improvement in studies with predominantly minority participants. Future research should include high-quality trials assessing the effect of peer support interventions on long-term patient-centered outcomes.
Acknowledgments
The authors would like to acknowledge the editorial assistance of Gaia Guirl-Stearley while preparing the manuscript.
Footnotes
Conflicts of interest: authors report none.
Funding support: This study was funded by internal funding from the University of Missouri, Department of Family and Community Medicine.
Previous presentation: Some of the findings from this article were presented in 2015 at the North American Primary Care Research Group (NAPCRG) conference, October 24–28, 2015; Cancun, Mexico.
Supplementary materials: Available at http://www.AnnFamMed.org/content/14/6/540/suppl/DC1/.
- Received for publication February 2, 2016.
- Revision received May 26, 2016.
- Accepted for publication June 2, 2016.
- © 2016 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Investigating the sustainability of self-help programmes in the context of leprosy and the work of leprosy missions in Nigeria, Nepal and India: a qualitative study protocol
- Here for You: A Review of Social Support Research in Young Adults With Diabetes
- Peer Coaching to Improve Diabetes Self-Management Among Low-Income Black Veteran Men: A Mixed Methods Assessment of Enrollment and Engagement
- Lifestyle interventions for type 2 diabetes management among migrants and ethnic minorities living in industrialized countries: a systematic review and meta-analyses
- Task Sharing Chronic Disease Self-Management Training With Lay Health Coaches to Reduce Health Disparities
- Ontario Brain Injury Association Peer Support Program: a mixed methods protocol for a pilot randomised controlled trial
- Supported self-management for people with type 2 diabetes: a meta-review of quantitative systematic reviews
- Aspects of Multicomponent Integrated Care Promote Sustained Improvement in Surrogate Clinical Outcomes: A Systematic Review and Meta-analysis
- In This Issue: Social Context; Disease Causes
- A Meta-Analysis of Peer-Support Interventions for Adults With Diabetes