
Abstract
PURPOSE To quantify the risk of peritonsillar abscess (PTA) following consultation for respiratory tract infection (RTI) in primary care.
METHOD A cohort study was conducted in the UK Clinical Practice Research Datalink including 718 general practices with 65,681,293 patient years of follow-up and 11,007 patients with a first episode of PTA. From a decision tree, Bayes theorem was employed to estimate both the probability of PTA following an RTI consultation if antibiotics were prescribed or not, and the number of patients needed to be treated with antibiotics to prevent 1 PTA.
RESULTS There were 11,007 patients with PTA with age-standardized incidence of new episodes of PTA of 17.2 per 100,000 patient years for men and 16.1 for women; 6,996 (64%) consulted their practitioner in the 30 days preceding PTA diagnosis, including 4,243 (39%) consulting for RTI. The probability of PTA following an RTI consultation was greatest in men aged 15 to 24 years with 1 PTA in 565 (95% uncertainty interval 527 to 605) RTI consultations without antibiotics prescribed but 1 in 1,139 consultations (1,044 to 1,242) if antibiotics were prescribed. One PTA might be avoided for every 1,121 (975 to 1,310) additional antibiotic prescriptions for men aged 15 to 24 years and 926 (814 to 1,063) for men aged 25 to 34 years. The risk of PTA following RTI consultation was smaller and the number needed to treat higher at other ages and risks were lower in women than men.
CONCLUSIONS The risk of PTA may be lower if antibiotics are prescribed for RTI but even in young men nearly 1,000 antibiotic prescriptions may be required to prevent 1 PTA case. We caution that lack of randomization and data standardization may bias estimates.
- antibacterial agents
- antibiotics
- primary health care
- respiratory tract infections
- peritonsillar abscess
- decision support
INTRODUCTION
Widespread unnecessary use of antibiotics is contributing to the development of antimicrobial drug resistance with increased risk of infections from difficult-to-treat antibiotic-resistant organisms.1,2 Strategies designed to limit antimicrobial drug resistance in health care settings focus on reducing inappropriate prescribing of antibiotics,3 while ensuring antibiotics remain available for use when required.4 Reduction of antibiotic prescribing raises a concern that fewer antibiotic prescriptions might increase the risk of serious bacterial infections. In a recent study, we found evidence that peritonsillar abscess (PTA), also known as quinsy, may be more frequent at family practices which prescribe fewer antibiotics for respiratory infections.5 This is plausible because a meta-analysis of 8 clinical trials found that antibiotic treatment for sore throat reduced the risk of PTA, but the review included only 25 cases of PTA, of which 16 were from a trial reported in 1951 when quinsy was more common.6 Peritonsillar abscesses are less frequent now.7 There is often evidence of infection with multiple microorganisms8 but group A streptococcal and Fusobacterium necrophorum infections may be the most common pathogens.9 The present study aimed to quantify the risks of PTA fol-lowing a respiratory tract infection (RTI) consultation according to whether antibiotics were prescribed or not. We determined how often cases of peritonsillar abscesses arose in patients who had previously consulted for RTI and quantified the effect of antibiotic treatment on the risks of PTA. We aimed to integrate these empirical estimates into a model to inform clinical decisions.
METHODS
Study Population
A population-based cohort study was conducted using primary care electronic health records from the UK Clinical Practice Research Datalink (CPRD). The CPRD is a database of fully anonymized electronic health records from approximately 7% of UK family practices. CPRD data are broadly representative of the UK population, and the high quality of CPRD data has been confirmed in many studies.10,11 The study population was the entire registered patient population of the Clinical Practice Research Datalink, from January 1, 2002 through December 31, 2017, including nearly 10 million registered patients.
Main Measures
The primary outcome was a first diagnosis of PTA in primary care electronic health records from general practice consultations, referrals, or hospitals. Diagnoses were defined using medical codes for “peritonsillar abscess” or “quinsy”. For each participant with PTA, we evaluated consultation records before the PTA diagnosis to estimate the proportion of cases with consultations for self-limiting RTI or any consultation, and the proportion of patients prescribed an antibiotic within 7, 14, 30, or 60 days preceding a PTA diagnosis. We defined comorbidity as present or absent in each person year using the seasonal flu at-risk codes that identify groups at higher risk of infection who may benefit from an influenza vaccination. Smoking status was evaluated using records of smoking status, smoking cessation advice, and smoking cessation prescriptions to categorize patients as current smokers, ex-smokers, and non-smokers. Patients with no evidence for smoking were categorized as non-smokers.
We estimated the consultation rate for self-limiting RTIs and the proportion of RTI consultations that resulted in an antibiotic prescription from a sample of the entire CPRD database. This was because the data extract represented by all respiratory consultations in the CPRD database is unfeasibly large, and analysis of a data set of that magnitude is not permitted under the terms of our data license. We drew a random sample from the CPRD denominator file after stratifying by general practice, sex, 5-year age group, and calendar years from 2002 through 2017. This resulted in a total sample of 671,830 patients whose data was used to estimate age-standardized and age-specific consultation rates for self-limiting RTIs, and the proportion of RTI consultations which resulted in an antibiotic prescription. Self-limiting RTIs included “upper respiratory infections”, colds, sore throat, cough and bronchitis, otitis media and sinusitis, as reported previously.12,13
Statistical Analyses
Person time at risk was calculated from January 1, 2002 or the start of the patient’s record, if later; follow-up was completed on December 31, 2017 or the end of the patient’s record, if later. Incident events were first-ever diagnoses of PTA during this period that were more than 12 months after the start of the patient’s record. Incidence rates were age-standardized using the European Standard Population for reference. Age-specific incidence rates were calculated for 5-year age groups. The remaining analyses were conducted using 10-year age groups from 0 to 4 years, 5 to 14 years, then 10-year age groups, to 85 years and older. All data were analyzed in R, version 3.5.0 (Project for Statistical Computing).
Decision Tree
A decision tree was costructed.14 Among the population of patients registered in primary care, consultations for RTI lead to antibiotic prescription for some but not for others. Cases of PTA may arise with or without a prior antibiotic prescription. The probabilities that determine each transition are outlined in Table 1. A Bayesian approach was used to calculate the risk of PTA, according to whether or not patients had consulted for a RTI and whether or not they were prescribed an antibiotic on the date of a RTI consultation.15 Using the notation shown in Table 1 we calculated the probability of PTA, given that the patient had consulted for RTI and been prescribed an antibiotic or not. The number of additional antibiotic prescriptions required to prevent 1 case of PTA (number needed to treat) was calculated as the reciprocal of the difference in probabilities (Table 1). In order to optimize precision, estimates represented the average values during the period from 2002 through 2017. Uncertainty intervals for probabilities were estimated by taking 1,000 random draws from the beta distribution.16 The probability of PTA following a RTI consultation was plotted by age and sex, together with 95% uncertainty intervals.
Definition and Data Source for Probabilities
Sensitivity Analyses
In sensitivity analyses, we analyzed data for a subset of general practices in England that were eligible for linkage to hospital discharge record data (Hospital Episodes Statistics). In the linked sample, we identified cases of peritonsillar abscess from hospital admissions where PTA (ICD-10 code J36) was the primary diagnosis. We conducted analyses of cases of PTA that were recorded either in primary or hospital care, as well as hospital admissions for PTA as a separate group.
RESULTS
Incidence of Peritonsillar Abscess
There were 9,870,559 registered patients from 718 general practices, with 65,681,293 of follow-up, included in the analysis. There were 11,007 patients with a first episode of PTA from 2002 through 2017, 53% of patients were male and 75% of PTA patients were aged 15-44 years (Table 2). The age-standardized incidence of new episodes of PTA was 17.2 per 100,000 patient years for men and 16.1 for women. From 2002 through 2017, annual age-standardized incidence rates ranged from 12.7 to 19.5 per 100,000 for both men and women with no consistent trend. Age-specific incidence rates revealed that the incidence of PTA increased with age up to patients aged 15-19 years (45.3 per 100,000 patient years, 95% CI, 44.7-45.8, for men and 51.8 per 100,000 patient years, 51.3-52.4, for women) and then decreased with increasing age (Supplemental Figure 1, available at https://www.AnnFamMed.org/content/18/5/390/suppl/DC1/).
Characteristics of Patients With Peritonsillar Abscess
Proportion of Patients With PTA Who Consulted a GP or Were Prescribed Antibiotics Prior to Their First PTA Diagnosis (N = 11,007)
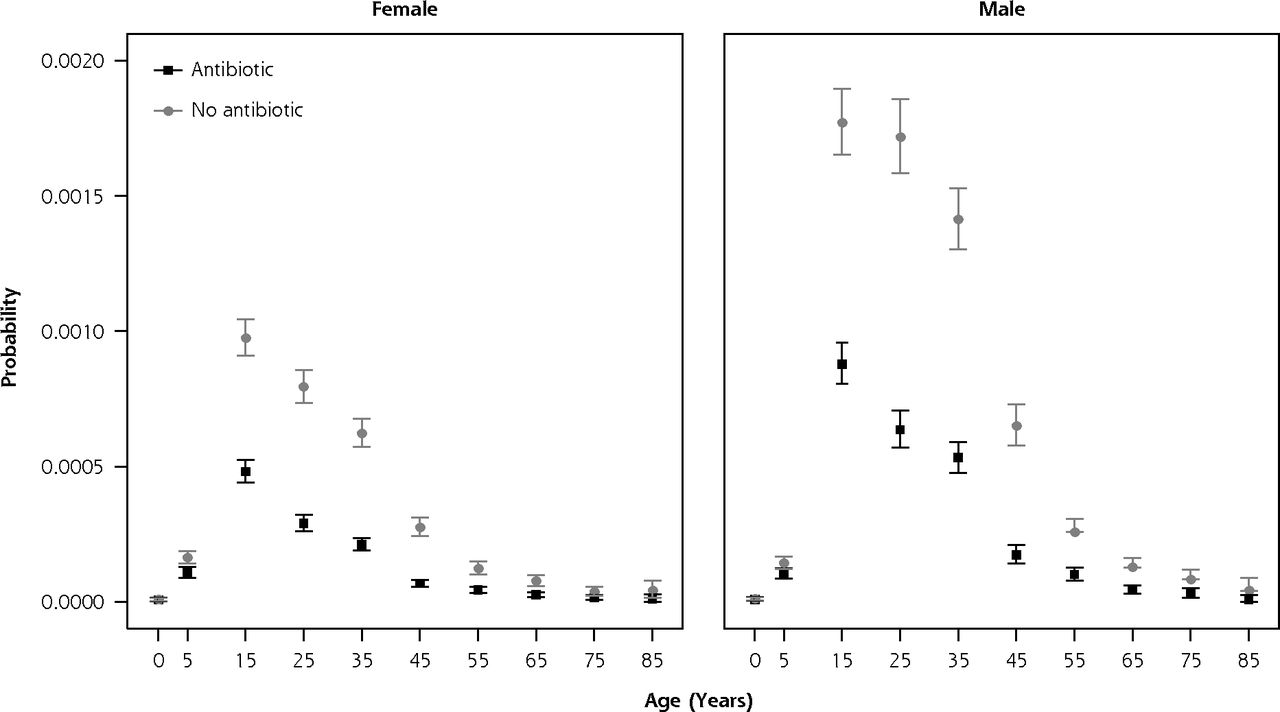
Patients with PTA were more likely to be smokers (34% of PTA patients were current smokers compared with 16% of person-time in a sample of the general population), while 12% of PTA patients and the general population sample were recorded ex-smokers. This effect was consistent when stratifying by sex and remained consistent over time. The prevalence of comorbidity was lower among PTA cases (28.6%) than in the general population (40.8% of all follow-up self-limiting RTI consultation was 0.483 (95% CI, 0.483-0.484) (Supplemental Figure 2, available at https://www.AnnFamMed.org/content/18/5/390/suppl/DC1/). Age- and sex-specific probabilities of PTA, given that patients had consulted for RTI, were also calculated (Supplemental Table 1, available at https://www.AnnFamMed.org/content/18/5/390/suppl/DC1/). The probability of PTA was higher in men than women and was greatest between those aged 15-34 years (Figure 1). In both men and women, and at all ages, the probability of PTA following a RTI was lower if an antibiotic was prescribed. The number needed to treat with an antibiotic, to prevent 1 case of PTA, was also calculated for each age-sex group. The number needed to treat was lower for patients with the highest probability of PTA. For patients aged 25-34 years, the number of patients with RTI who would need to be prescribed an antibiotic to prevent 1 PTA case was 926 (95% CI, 814-1,063) for men and 1,984 (95% CI, 1,756-2,263) women. The numbers were similar in men and women aged 15-24 and 35-44 years but were substantially greater for either younger or older patients (Table 4).
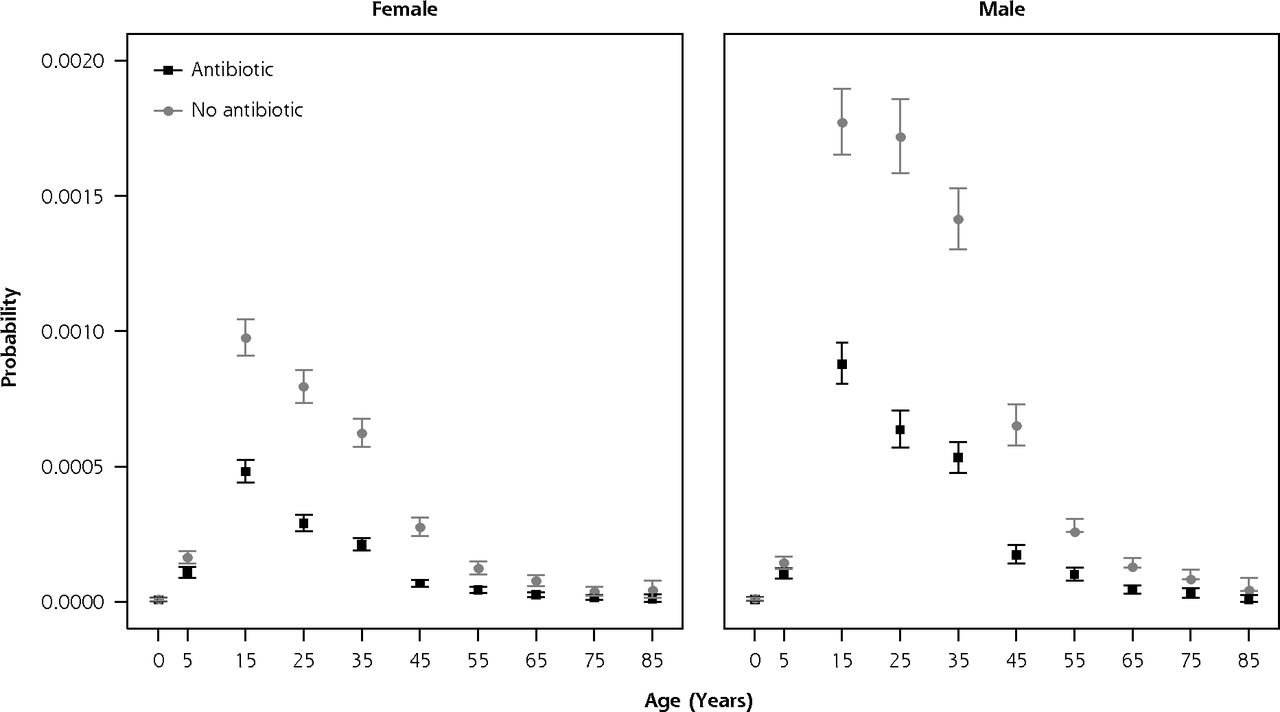
Age- and sex-specific 30-day probability of PTA in patients who consulted for self-limiting RTI, with and without antibiotic prescription.
PTA = peritonsillar abscess; RTI = respiratory tract infection.
Note: Vertical lines represent 95% uncertainty intervals.
Estimated Number of Antibiotic Prescriptions Required to Prevent 1 Case of PTA by Age Group and Sex
Linked Hospital Episodes Data
In the subset of patients with linked hospital records, the age-standardized incidence of PTA was 20.6 per 100,000 patient years for men and 19.0 per 100,000 patient years for women. The distribution of cases over time and between age groups was similar between CPRD and Hospital Episodes Statistics data (Supplemental Figure 1). Estimates of the risk of PTA with and without antibiotics were consistent with data from CPRD. The protective effect of antibiotics was also evident when considering only PTA cases resulting in hospitalization (Supplemental Figure 3, available at https://www.AnnFamMed.org/content/18/5/390/suppl/DC1/).
DISCUSSION
Principal Findings
There have been few large population-based studies This study provides precise estimates for disease incidence and shows that PTA is most frequent in young people aged 15-24 years and is more frequent in men. Nearly two-thirds of patients consulted with their general practitioner in the 30 days before PTA diagnosis, with about one-half of these consultations being recorded as self-limiting RTIs. The analyses demonstrate a protective effect of antibiotic prescribing against PTA following a RTI consultation for both men and women and in all age groups. The overall risk of PTA was low, however, and 1,000 or more antibiotic prescriptions would be required to prevent 1 PTA even in the age group at highest risk. Consultation rates for respiratory illness are considerably higher in women than men and this may account for the lower risk of PTA following a consultation for RTI in women than men.
Strengths and Weaknesses of the Study
The study benefited from a very large sample size drawn from all parts of the United Kingdom. The study population comprised almost 10 million patients, with 11,007 PTA cases over 16 years, providing precise estimates for a rare outcome. A key limitation of this study is that its nonrandomized design meant that patients were not randomly assigned to antibiotic treatment. It is likely that patients who received antibiotics had more severe illness, and a greater risk of PTA, than patients who did not receive antibiotics. Consequently, the risk of PTA in antibiotic-treated patients may have been overestimated, and the risk in untreated patients underestimated, in comparison with a random allocation. As a result, the protective effect of antibiotic treatment may have been underestimated and the true number of antibiotic prescriptions needed to prevent 1 PTA may be lower than we have estimated. It was not possible to include data on symptoms or severity of RTIs; we searched patients’ records for markers of illness severity including fever, lymphadenitis, or mention of Centor criteria,17 but these were recorded in a very small number of cases. As noted by others, not all consultations in primary care electronic records have a clinical code assigned.18 Almost one-third of PTA patients consulted their general practitioner with a self-limiting RTI in the 30 days preceding their PTA diagnosis, but this figure may be an underestimate because it is known that acute illness presentations are not always accurately coded in primary care.18 The data for the study, recorded prospectively by family physicians and other primary care professionals, was for clinical practice use, not research. Thus, standardized recording procedures were not used, leading to variability in data recording. The estimates represent values expected at an average practice, but actual values could vary depending on consultation and prescription rates or data recording procedure used at different practices. Previous studies have shown that diagnoses recorded in electronic health records have high predictive validity11 but there is evidence of differential recording in alternative data sources.19 Our analyses showed that analysis of hospital records, in addition to primary care records, did not change conclusions overall. In a clinical trial, an overall effect is usually estimated before sub-group analyses are performed, but this approach is not always desirable in epidemiological analysis of population data, especially when rates vary considerably by age.20,21 In light of the age-related variations of PTA incidence, we analyzed data by sub-group of age and sex but note that small differences across sub-groups should be interpreted with caution.
Comparison With Previous Studies
In a previous study, there was evidence that general practices with lower rates of antibiotic prescription for RTI had a higher incidence of PTA,5 estimating that there might be 1 additional case of PTA over 10 years for a general practice that reduced antibiotic prescribing for RTI by 10%.5 The present patient-level analyses show that antibiotic prescription at a RTI consultation is associated with reduced risk of PTA, consistent with the more limited evidence from randomized clinical trials. In a review of randomized controlled trials,6 the relative risk of PTA within 60 days of a sore throat was 0.15 (95% CI, 0.05-0.47) after antibiotic treatment compared with no antibiotic. Most evidence, however, was provided by 1 trial published in 1951 with a relatively small sample size.6 Previous nonrandomized studies also suggested a protective effect of antibiotics against PTA but did not quantify age- and sex-specific risks following a primary care consultation for RTI.22–24
Our estimates of PTA incidence (16-17 per 100,000 patient years) from CPRD data were consistent with that of previous studies,5 although our study spanned a wider time period. Previous studies have been limited by not including data from hospital discharge records but we found that the associations between PTA incidence and antibiotic use were consistent whether we analyzed CPRD data only, or also included Hospital Episode Statistics data. Consistent with previous studies, our data show an excess of current smokers compared with population reference data for smoking prevalence.25 Comorbidity is not usually considered as a risk factor for PTA.7 Consistent with Klug’s review,7 there was only weak evidence of seasonality.
The risk of PTA might be higher following presentations for sore throat or tonsillitis. Respiratory infections often have mixed presentation beginning with a sore throat, however, followed by symptoms of coryza and later cough.26 RTI presentations are also often indistinctly coded making analysis of sub-groups challenging.18 Clinical guidelines for the management of sore throat in the United Kingdom advocate the use of clinical risk scoring with either Centor17 or Fever-PAIN27 scores. Bacteriological testing is discouraged and is infrequent in the United Kingdom, possibly in contrast to the United States where it is endorsed in some clinical guidelines.28
Implications for Clinicians and Policy-Makers
We found that antibiotic prescriptions were protective against PTA across all age groups studied. The absolute risk of PTA was very low, however, and the number of antibiotic prescriptions needed to prevent 1 case of PTA was very high. Even among young adults, the highest risk group for PTA, 1,000 or more patients consulting with a RTI would need to be prescribed antibiotics to prevent a single PTA case. Furthermore, a considerable proportion of PTA patients had not presented to their family physician previously, suggesting that their complication would not have been preventable through medical treatment. This adds further weight to the growing body of evidence that reducing antibiotic prescribing further will not result in a substantial increase in this outcome, particularly as only one-third of PTA patients consulted with a RTI before their PTA diagnosis, one-third had nonspecific consultation codes recorded, and one-third of patients did not consult at all. The risk of PTA is greater in smokers and sore throat consultations may be an opportunity to discuss smoking cessation.
Acknowledgment:
The SafeABStudy Group also includes Dr Caroline Burgess, Dr Vasa Curcin, Dr Robin Fox (Bicester, Oxfordshire), Prof Alastair Hay (University of Bristol), Prof Paul S. Little (University of Southampton), Prof Michael V. Moore (University of Southampton), Dr James Shearer.
Footnotes
Conflicts of interest: authors report none.
To read or post commentaries in response to this article, see it online at https://www.AnnFamMed.org/content/18/5/390.
Author contributions: M.G. wrote the study protocol; J.W. conducted data analyses and drafted the paper; J.C., C.B., M.A. and M.G. provided advice on data analysis and interpretation, as well as critically reviewing the paper. All authors approved the final draft. J.W. is guarantor.
Funding support: The trial is funded by the National Institute for Health Research (NIHR) Health Services and Delivery Programme (16/116/46). M.G. was supported by the NIHR Biomedical Research Centre at Guy’s and St Thomas’ Hospitals. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health. The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The authors had full access to all the data in the study and all authors shared final responsibility for the decision to submit for publication.
Disclaimer: The lead author (J.W.) affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as originally planned (and, if relevant, registered) have been explained.
Data sources: The study is based in part on data from the Clinical Practice Research Datalink obtained under license from the UK Medicines and Healthcare products Regulatory Agency. However, the interpretation and conclusions contained in this report are those of the authors alone.
Ethical approval: The protocol for the study was approved by the CPRD Independent Scientific Advisory Committee protocol number 18_041R.
Supplemental materials: Available at https://www.AnnFamMed.org/content/18/5/390/suppl/DC1/.
- Received for publication September 9, 2019.
- Revision received January 10, 2020.
- Accepted for publication January 27, 2020.
- © 2020 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.