
Abstract
PURPOSE Use of the electronic health record (EHR) during face-to-face clinical encounters affects communication, and prior research has been inconclusive regarding its effect. This survey study assessed health care practitioner use of EHR-specific communication skills and patient and practitioner experiences and attitudes regarding EHR use during clinical encounters.
METHODS For this US-based study, we distributed previously validated surveys to practitioners and adult patients (aged >18 years) at academic primary care practices from July 1, 2018 through August 31, 2018. The electronic practitioner survey was completed first; a paper survey was administered to patients after appointments. Descriptive statistics were calculated, and the Cochran-Armitage test was used to assess for associations between key variables.
RESULTS The practitioner response was 72.9% (43/59); patient response, 45.2% (452/1,000). Practitioners reported maintaining less eye contact (79.1%), listening less carefully (53.5%), focusing less on patients (65.1%), and visits feeling less personal (62.8%). However, patients reported that practitioners provided sufficient eye contact (96.8%) and listened carefully (97.0%); they disagreed that practitioners focused less on them (86.7%) or that visits felt less personal (87.2%). Patients thought EHR use was positive (91.7%); only one-third of practitioners (37.2%) thought that patients would agree with that statement. Practitioners reported stress, burnout, and a lack of sufficient time for EHR documentation.
CONCLUSIONS A discrepancy existed in this study between patient and practitioner experiences and attitudes about EHR use, which appeared to negatively affect the experience of health care practitioners but not patients. Organizations should adopt formal strategies to improve practitioner experiences with EHR use.
INTRODUCTION
The electronic health record (EHR [computer implied throughout]) is intended to promote safe, efficient, and high-quality medical care.1,2 However, use of the EHR during face-to-face clinical encounters affects communication, and prior research is inconclusive regarding its effect on patient and health care practitioner experiences.3-7 Previously described as a “third person” in the examination room, EHR use during patient visits changes a health care practitioner’s eye gaze and posture and can decrease attention given to patients.3,7-10 Entering health information, placing electronic orders, and retrieving results can be distracting to patients and practitioners.11,12 When practitioners focus on their computer, dialog is easily disrupted and can lead to gaps in communication and patients feeling unheard.13,14 For practitioners, the EHR has also been associated with work-related dissatisfaction and burnout.15
Experts have suggested that practitioners can mitigate the potentially negative effects of EHR use during clinical encounters by learning and using EHR-specific communication skills.4,11,16-23 To improve patient and practitioner experiences with the EHR, we sought to conduct an assessment of practitioner use of EHR communication skills, as well as patient and practitioner experiences and attitudes regarding EHR use during clinical encounters. In addition, we sought to determine whether suggested EHR-specific communication skills were associated with better patient and practitioner experiences. We hypothesized that practitioners do not routinely use EHR-specific communication skills and anticipated that patients and practitioners would express some relative dissatisfaction with the EHR.
METHODS
Setting
For this US-based study, the Mayo Clinic Institutional Review Board deemed the study exempt from further review. We conducted the study in the family medicine and internal medicine primary care practices at the Mayo Clinic in Scottsdale, Arizona, with a total of 59 practitioners (physicians, physician assistants, and nurse practitioners). Practitioners all used the same EHR and had computers with monitors that could be positioned to face the patient. We followed the Standards for Quality Improvement Reporting Excellence (SQUIRE) 2.0 guideline.
Surveys
The authors created separate, deidentified practitioner and patient surveys from existing tools in published research.11,24-26 The authors collected demographic data via survey. Practitioners self-reported how frequently (never, rarely, occasionally, fairly often, very often, always) they used the following 8 EHR-specific skills thought to be associated with better patient experience: (1) ask the patient the reason for the visit before turning to the computer, (2) explain how the computer can help care for the patient, (3) ask the patient permission to use the computer during the visit, (4) position the computer so the patient could see the screen, (5) explain to the patient what you are doing on the computer, (6) let the patient look on to see what you are doing on the computer, (7) show the patient results or information on the computer, and (8) express to the patient that you think the computer is a positive thing. Practitioners completed the Mini Z burnout survey and self-reported their confidence with the EHR and how much time out-of-office they spend documenting EHRs.15 Practitioners could provide optional narrative comments.
Patients self-reported their level of agreement with whether the practitioner they saw that day used the 8 EHR-specific skills (strongly disagree, disagree, strongly agree, agree, not applicable). Patient attitudes regarding the effect of the EHR on communication and their overall experience were assessed using a 5-point Likert scale (strongly disagree, disagree, agree, strongly agree, not applicable). Patients could provide optional narrative comments.
Data Collection
The practitioner survey was distributed first to physicians, physician assistants, and nurse practitioners from July 1, 2018 through July 12, 2018. An e-mail invitation was sent with a secure link to a Research Electronic Data Capture (REDCap) survey. Once practitioner-response saturation was reached (no additional responses after a third reminder e-mail), patient surveys were distributed. From July 15, 2018 through August 31, 2018, patients with internal medicine or family medicine outpatient office visits were invited to complete a paper survey (English only) immediately after their appointment. Surveys were deposited in a secured lockbox in the patient waiting area; data were entered by statisticians into a REDCap database.
Statistical Analyses
We calculated descriptive statistics and used the Cochran-Armitage test to assess for the following associations between key variables in the practitioner survey: (1) the association between frequency (occasionally and fairly often/very often/always) of documenting or entering orders in front of patients and weekly time (<1, 1 to <2, ≥2 hours) working on EHRs outside of office hours, and (2) the trend of practitioner’s reporting working <2 hours outside of office hours across all levels of burnout. We performed data analyses using SAS version 9.4 (SAS Institute Inc). All tests were 2-sided, and P values <.05 were considered statistically significant.
RESULTS
The practitioner response rate was 72.9% (43/59). Of the respondents, 64.3% were physicians, 23.8% were nurse practitioners, and 11.9% were physician assistants (Table 1). Approximately 63% of respondents identified as female. The patient response rate was 45.2% (452/1,000). Of the respondents, 51.7% identified as female (Table 2).
Demographic Data for Practitioners
Demographic Data for Patients
Report of EHR-Specific Communication Skills
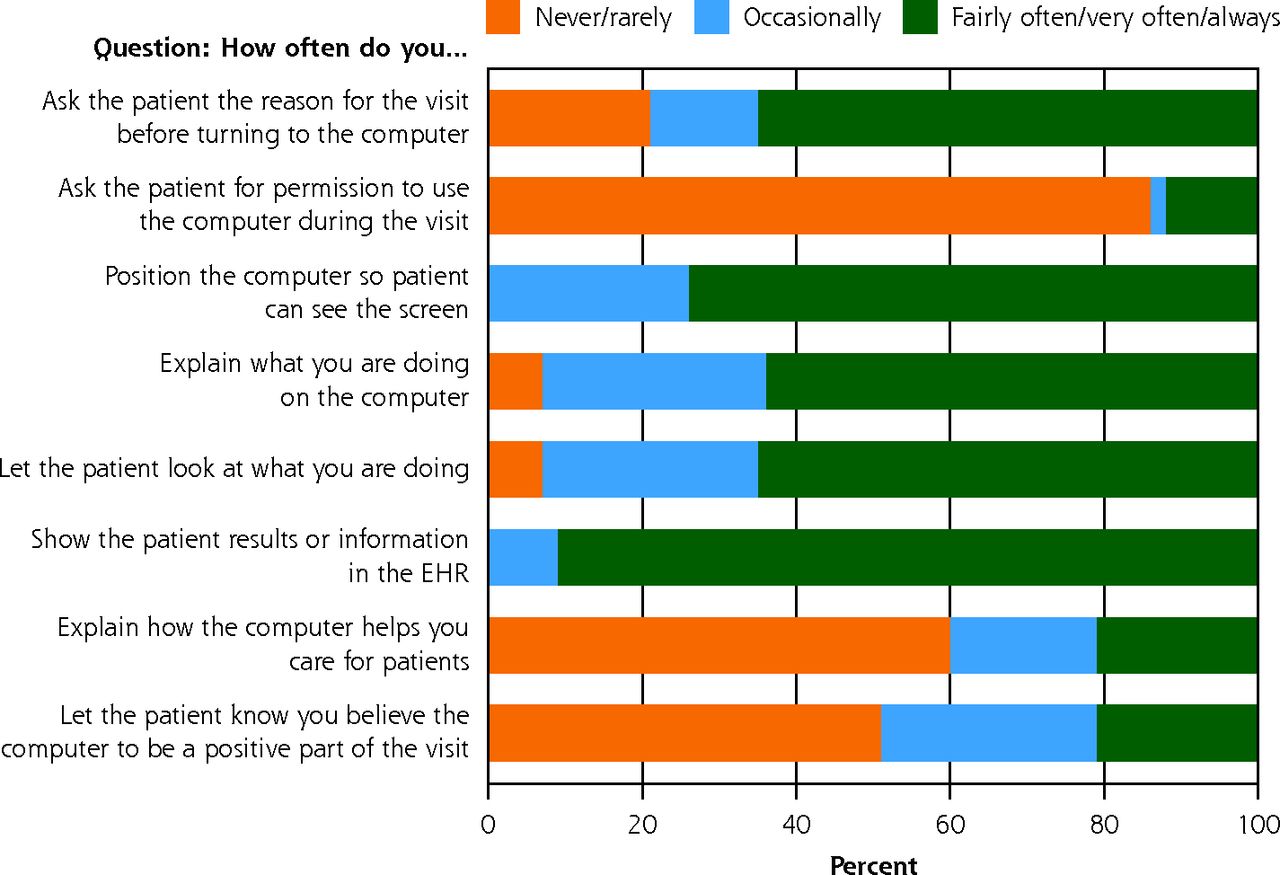
Practitioners’ self-reporting of how frequently they used the 8 EHR-specific communication skills is shown in Figure 1. Practitioners reported that they never/rarely explained how the computer helps them take care of the patient (60.5%) or asked the patient permission to use the computer (86.0%), although they fairly often/very often/always asked patients the reason for their visits before turning to the computer (65.1%) and positioned the computer so the patient could see the screen (73.8%). Nearly all practitioners showed patients results or information on the computer (90.7%). Less than one-half (48.8%) thought the computer was a positive factor in the visit.

Practitioner reports of 8 behaviors specific to use of the electronic health record.
EHR = electronic health record.
Note: A Likert scale was used to stratify answers for the EHR-specific communication skills. Like categories were combined for the graph (n = 43).
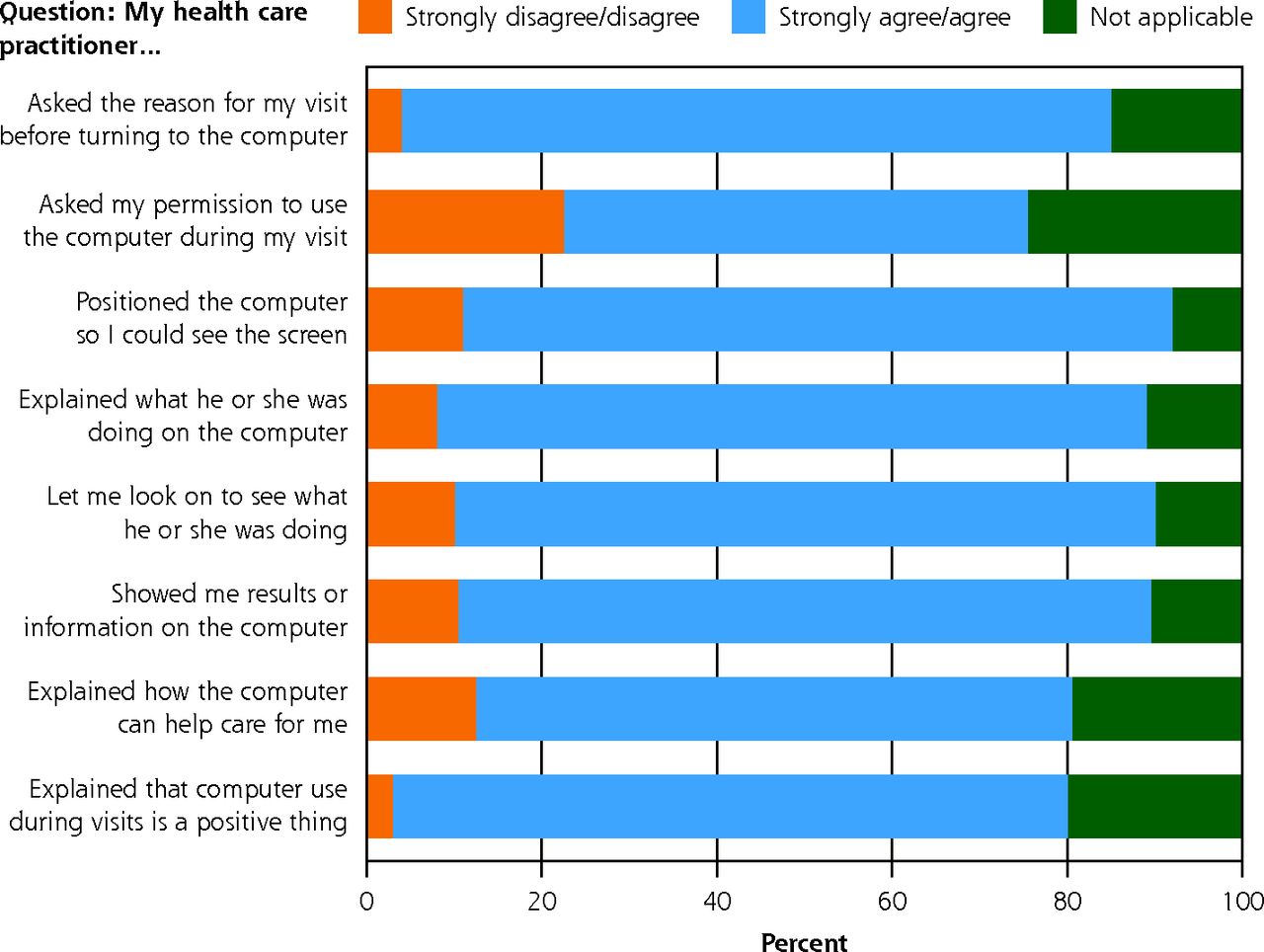
Patient reports of use of the 8 EHR-specific communication skills by the practitioner are shown in Figure 2. Patients agreed or strongly agreed that practitioners explained how the computer could help in their care (67.6%) and felt that computer use during the visit was a positive thing (76.9%). Overall, they had very positive thoughts about the computer and the visit in general.
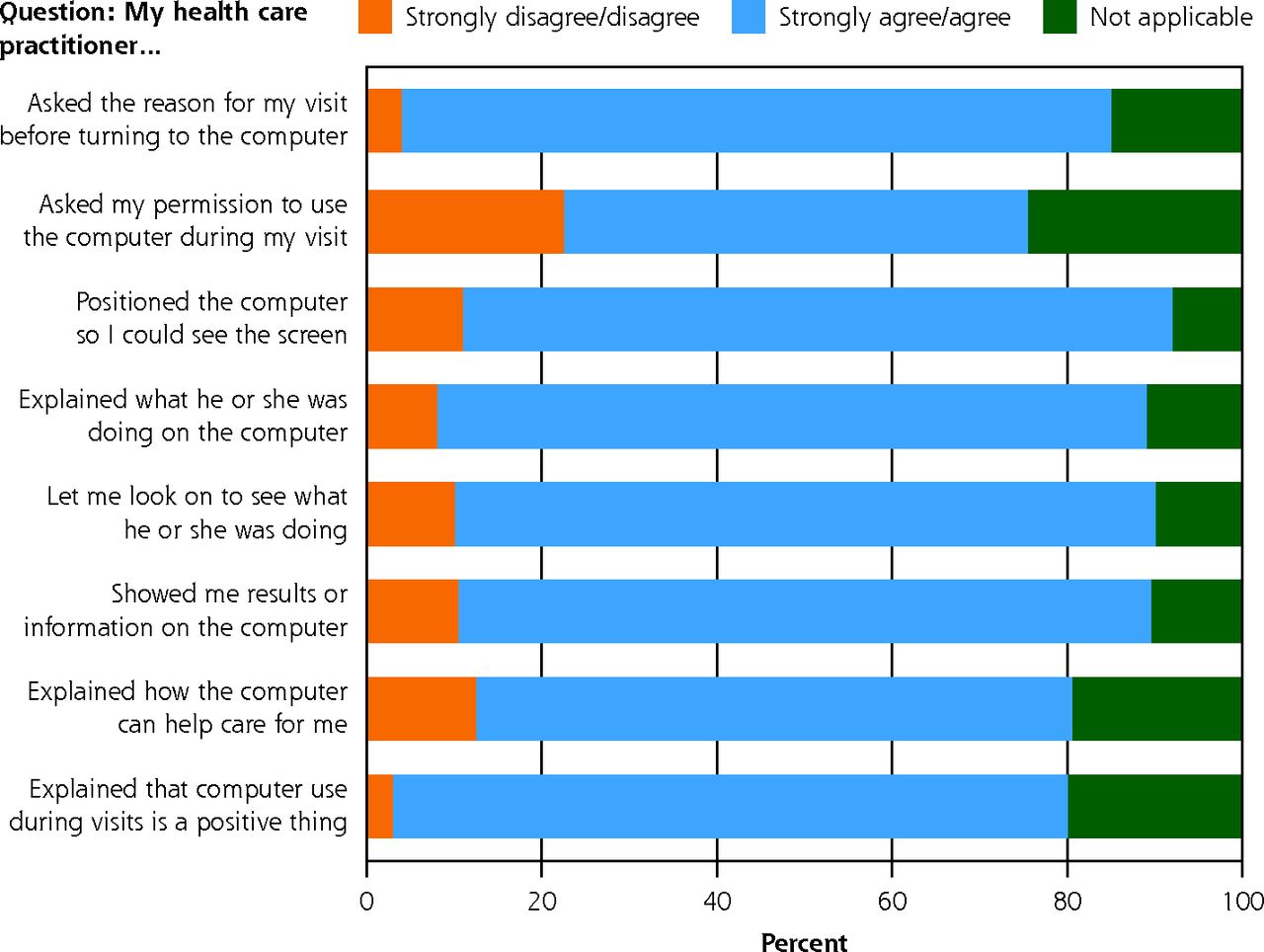
Patient reports of EHR-specific physician behaviors.
EHR = electronic health record.
Note: A Likert scale was used to stratify answers to the 8 EHR-specific communication skills. Like categories were combined for the graph (n = 452).
EHR Use During the Clinical Encounter: Practitioner and Patient Experiences
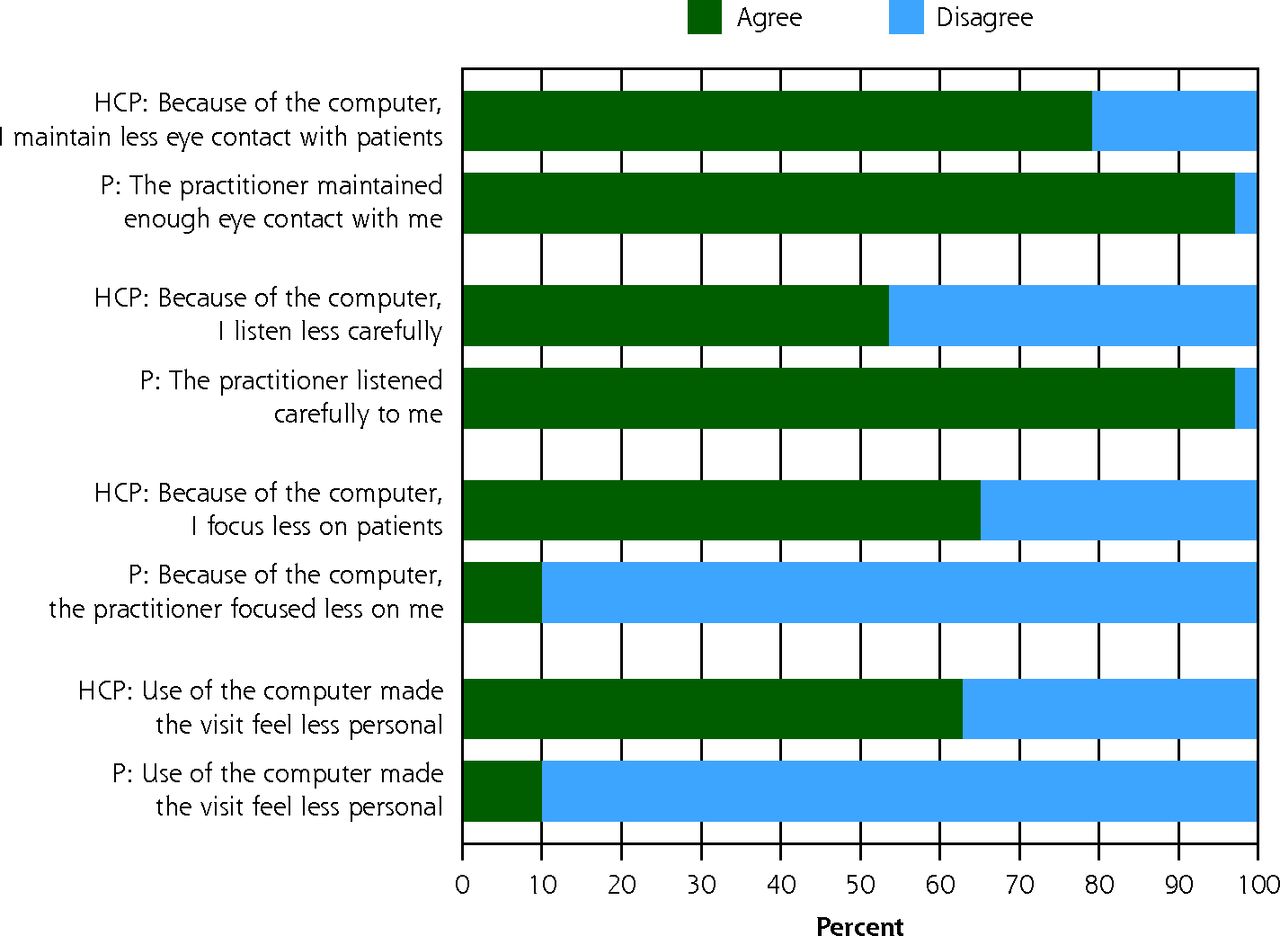
Practitioner and patient experiences with EHR use during clinical encounters varied (Figure 3). Practitioners reported maintaining less eye contact (79.1%), listening less carefully (53.5%), focusing less on patients (65.1%), and visits feeling less personal (62.8%). Patients reported that practitioners provided sufficient eye contact (96.8%) and listened carefully (97.0%); they disagreed that practitioners focused less on them (86.7%) and visits felt less personal (87.2%). Practitioners largely believed that the EHR detracted from the visit experience, whereas patients disagreed. Nearly all patients (91.7%) agreed that use of the EHR was a positive part of their visit. Only one-third of practitioners (37.2%) thought that patients would agree with this statement.
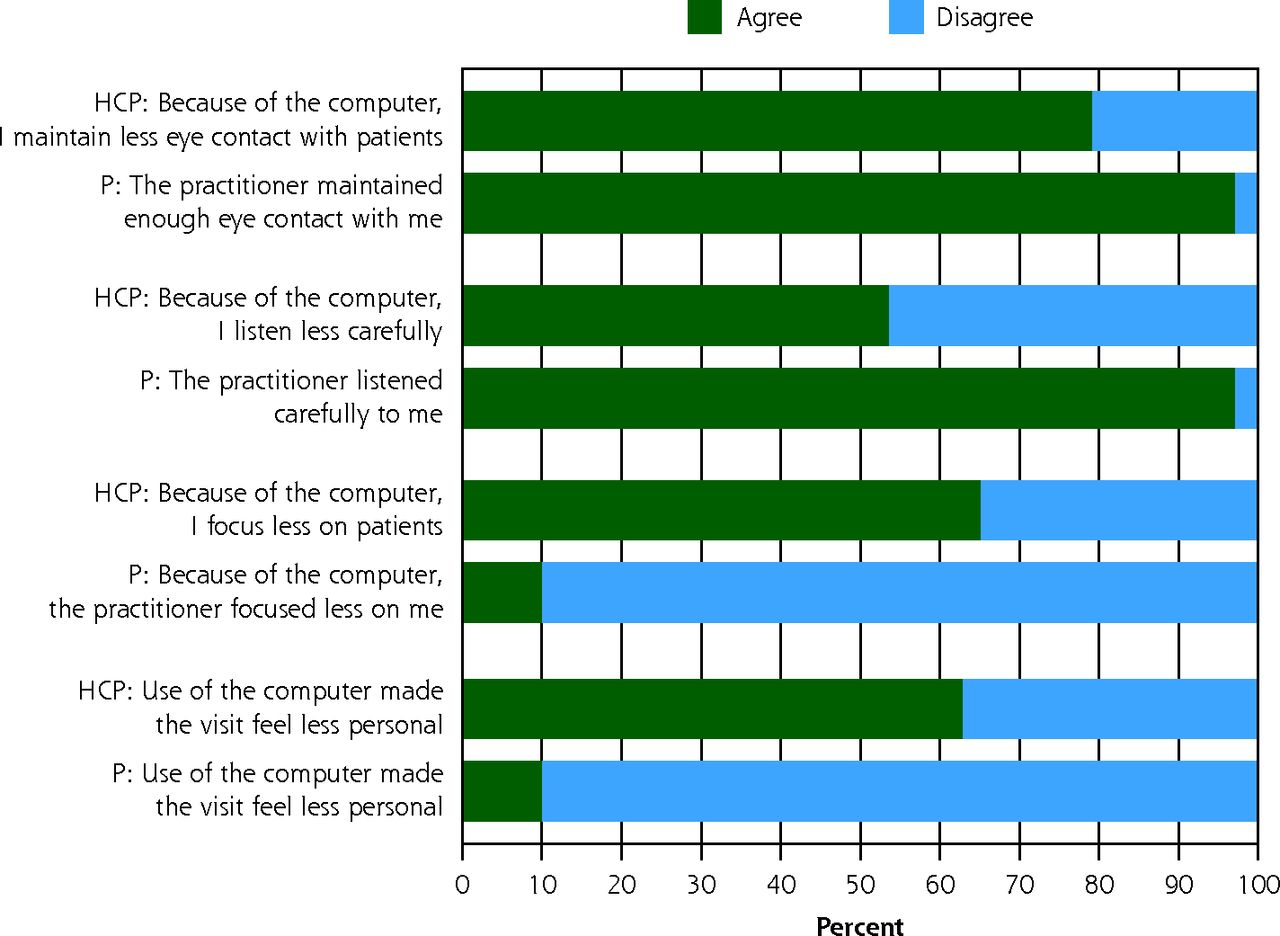
Practitioner and patient experiences with electronic health record use during clinical encounters.
HCP = health care practitioner; P = patient.
Practitioner EHR Practices and Work Experiences
Regarding EHR practices, 95.4% of practitioners reported entering orders and documenting in the EHR in front of patients and feeling confident in their ability to do so (97.7%), and 72.1% completed patient orders before the end of the visit. On average, practitioners reported spending 3 out-of-office hours per week working on EHRs.
Regarding the Mini Z burnout survey, most practitioners reported feeling a great deal of stress because of their job (62.8%). Only 9.3% of practitioners reported enjoying their work and having no symptoms of burnout; 44.2% reported feeling stressed and having less energy but not feeling burned out; 37.2% reported definitely feeling burned out; and 9.3% reported symptoms of burnout that would not go away. They reported poor or marginal control over workload (60.5%) and time for documentation (67.4%) and moderately high or excessive time spent on EHRs at home (62.8%). Most respondents reported good (67.4%) vs poor or satisfactory (32.6%) EHR proficiency.
Narrative Comments
A qualitative analysis of narrative comments is beyond the scope of this article; select comments are presented in the Discussion section.
Associations Between Key Variables
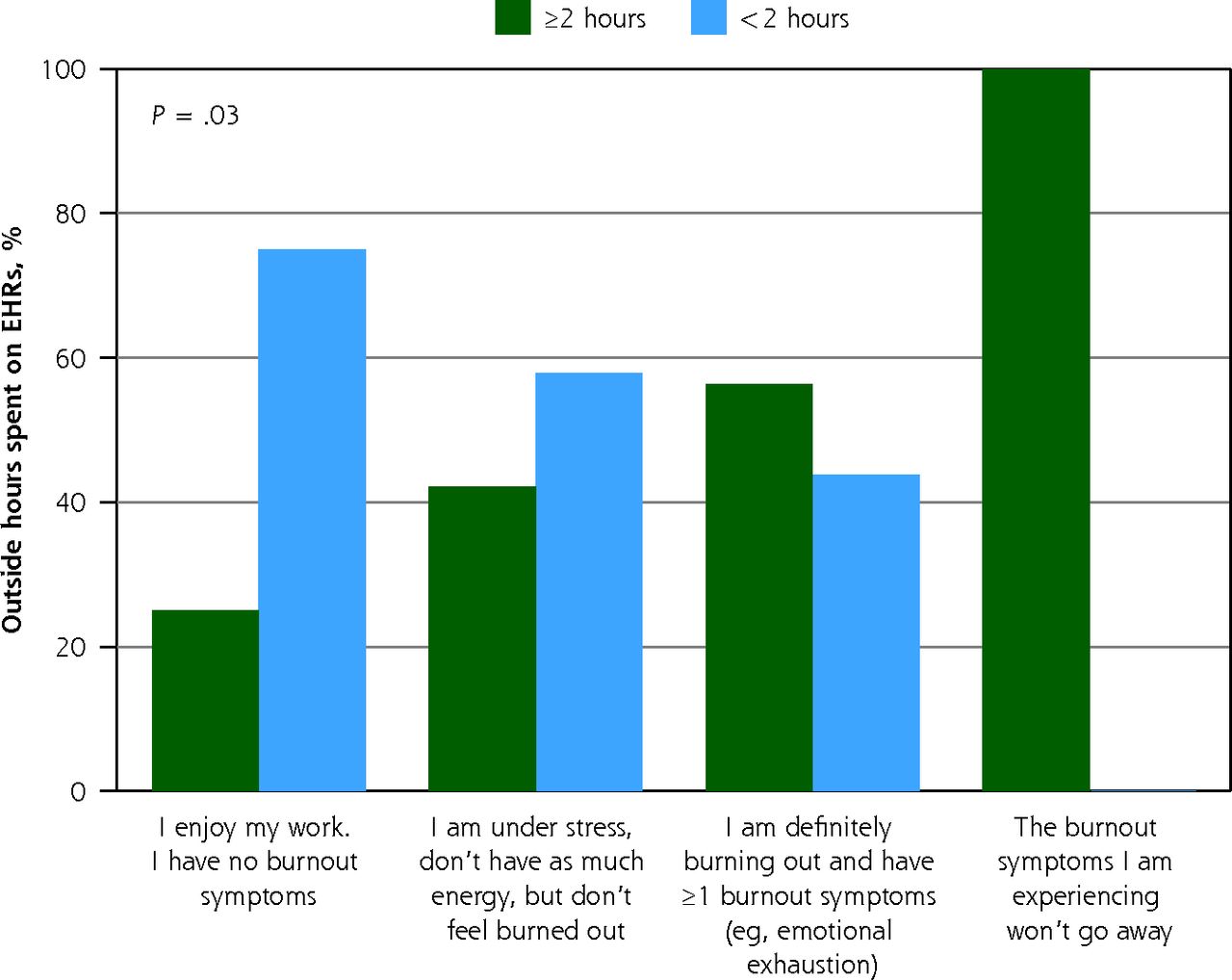
No statistically significant association was found between frequency of documenting or entering orders with patients in the examination room and out-of-office hours spent working on EHRs (P = .2). Of the practitioners who enjoyed their work and had no symptoms of burnout, 75% reported working <2 out-of-office hours per week. However, as burnout increased, fewer respondents reported working <2 out-of-office hours per week (Figure 4; n = 43) (P = .03).

Hours spent outside the office documenting in the electronic health record.
EHR = electronic health record.
Note: Data are shown as percentage of practitioners (n = 43). P value indicates trend for burnout in relation to working <2 out-of-office hours.
DISCUSSION
To improve the experiences of patients and practitioners, we assessed practitioner use of EHR-specific communication skills and patient and practitioner experiences with, and attitudes toward, EHR use during clinical encounters. We hypothesized that the data would reveal the need for an educational intervention to promote EHR-specific skills associated with a better experience. However, we found that practitioners already largely have and use these skills. Most notably, we identified a discrepancy that exists between patient and practitioner experiences with the EHR during clinical encounters. Patients largely had a favorable experience with practitioner use of the EHR during the clinical encounter, whereas practitioners did not.
Directly correlating specific skills with improved experiences is a challenge in experience research.27 The skills of interest studied are ones that experts suggest are patient centered and can be used to better incorporate the EHR into clinical practice for the benefit of patients, allowing them to have a therapeutic alliance with practitioners.22 These behaviors promote the type of eye contact and empathic communication that practitioners fear will be lost when their attention is on the EHR, and sometimes it is.8,9 However, research indicates that practitioners and patients differ in their opinions about the effect of the EHR on communication, and the present study supports these findings.5,7,10,28 Almost all patients reported that physicians maintained enough eye contact during the visit and listened carefully, whereas many of the practitioners (79.1%) reported maintaining less eye contact and listening less carefully (53.5%). Most patients rated their visit as “excellent”; thus, factors other than EHR skills must also have influenced patient experiences. As those in experience research work to improve patient experiences empirically and identify and evaluate behaviors truly correlated with an improved experience, it must be recognized that effect modification, a limitation, might lead to misinterpreting or overlooking relationships between practitioner behavior and patient experience.29
Experts in promoting patient-centered use of the EHR advise that practitioners should educate their patients about the EHR by discussing its potential benefits and explaining how computers and the EHR aid in providing medical care.17,18 In the present study, practitioners less frequently reported discussing these positive aspects of the EHR with their patients. In addition, fewer practitioners than patients agreed that the computer improved patients’ understanding of their health (67.0% vs 76.8%), and approximately 50% of practitioners disagreed that computer use during a patient encounter added anything positive. The data suggested a practitioner misperception that EHR use negatively affected patient experiences.7 The effect of this misperception, and its effect on stress and burnout related to EHR use, needs to be better understood and educational methods designed to remediate it. In the list of EHR-specific behaviors, we included a behavior that has not to our knowledge been previously studied in EHR-related research. We asked practitioners how frequently they ask for patient permission to use the computer during the visit; >80% responded “never/rarely.” We believe that a conversation regarding EHR use during a clinical encounter might benefit practitioners and patients. Practitioners will learn what patients think, and together they can decide how to proceed.30 With patient permission, practitioners might feel more empowered to use the EHR and adopt a more positive attitude about it, one that most patients in the present study had. Additional studies are needed to determine whether this might counter EHR-related burnout and promote well-being.
The practitioner survey also showed other areas of dissatisfaction that respondents had with the EHR. Although 86.0% of participants were overall satisfied with their current job, they reported stress, burnout, poor control over their workload and lack of time for EHR documentation. Of interest, no association existed between the frequency of documenting or entering orders in front of patients and time working outside of office hours. We expected the opposite and gleaned insight into this finding from some of the narrative responses to question prompts. One respondent stated, “…I do a lot of patient care through the in basket at home after work.” This study adds to the literature about practitioner experiences with EHRs and supports the need for organizations to adopt formal strategies to minimize time on EHRs outside of work hours.
The narratives also provided insight into what practitioners believed would be helpful for improving their experiences. They requested consistency in the EHR (ie, fewer changes) so that they do not, as another responded, “…have to figure out how to do something with a computer at almost every visit.” Regarding EHR effect on the patient-physician relationship, a practitioner commented, “It is just very impersonal…work that really detracts from listening/spending time with the patient.” In addition to a more efficient EHR, they requested assistance with inbox and message management and for a scribe to be present during clinical encounters, which would allow them to focus fully on their patients and, “not spend lunch and after hours catching up.”
Although the present study provides data to inform future research, it has limitations. Practitioners were aware of the study, which could have served to change practice behaviors and bias the results. Practitioner and patient data were anonymous; therefore, we could not analyze differences in the 2 practice types studied or differences by provider type. Survey nonresponders might have had different attitudes than those expressed by study participants. Data were collected at a single academic institution in Arizona, with a largely White, college-educated patient population and a largely White practitioner group. Thus, the results might not be representative of attitudes in other locations or among other patient or clinic populations; replicating this study in other clinical practices is critical to understanding the experiences of more diverse patient and provider populations. Surveys of skill implementation relied on self-report of behaviors, which was limited by recall bias and the desire to respond favorably (ie, social desirability); however, this potential limitation was minimized by using anonymous surveys and having patients complete surveys immediately after their visit.29 Patients’ recall of behaviors might have had limited validity, and patients rating their visit that day as “excellent” could be indicative of effect modification.29 Future research with direct observation could mitigate this potential source of bias, but it still must be recognized as a potential weakness in experience research.
Other factors identified in prior studies, such as practitioners’ baseline communication skills and the ongoing relationships between patients and practitioners, likely contributed to the finding of a positive patient experience.3,11,31 The high race concordance between patient and practitioner might have served to favorably bias the experience results.32 In addition, at onboarding, practitioners at our institution complete an in-person, 8-hour course in empathic communication. With implementation of the EHR, practitioners received at minimum 10 hours of EHR data management training. This type of training has been shown to increase proficiency and confidence with EHRs, and most of our participants reported EHR proficiency and feeling confident in their ability to enter orders and document in the EHR in front of the patient.19 Research suggests that EHR-specific empathic communication skills should be taught to practitioners, preferably via experiential learning opportunities, in which learners are observed in a supportive environment and provided direct feedback.3,16,17,19-21,23,33,34 Given that 46% of participants self-reported prior involvement in education or training on EHR-specific communication skills, this could have biased our results toward the null. An important question remains about whether EHR-specific behaviors truly correlate with better patient experience and, if so, by what means.
In conclusion, the results of the present study showed that more research is needed to understand the effects of EHR use on experience. It would be helpful to correlate positive experience findings with the specific behaviors used. In addition, work is needed to understand the discrepancy between patient and practitioner attitudes toward EHR use during a clinical encounter and to minimize practitioners’ misperceptions that use of the EHR negatively affects patient experience. Finally, measures are needed to improve the daily experience and burden of EHR use for practitioners. Organizations should be encouraged to adopt formal strategies to decrease the excessive time practitioners spend on EHRs outside of work hours.
Acknowledgments
The authors thank all of the respondents, whose participation made this study possible. We are also grateful to Helene R. Labonte, DO, and Michael L. Grover, DO, for their guidance and to the Mayo Clinic Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery for grant support. We acknowledge and thank Victor M. Montori, MD, and Ian G. Hargraves, PhD, for their guidance on study design. Marianne Mallia, ELS, MWC, Mayo Clinic, substantively edited the manuscript. The Scientific Publications staff at Mayo Clinic provided proofreading, administrative, and clerical support.
Footnotes
Conflicts of interest: authors report none.
Author contributions: All authors made substantial contributions to the conception and design of the study; the acquisition, analysis, and interpretation of the data; and the drafting and critical revision of the manuscript for important intellectual content.
Funding support: Financial support was provided by a Mayo Clinic Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery Practice Innovation Award.
- Received for publication August 26, 2021.
- Revision received December 9, 2021.
- Accepted for publication January 3, 2022.
- © 2022 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}
{kind=link}
{kind=link}