
Article Figures & Data
Figures
- Figure 1
Flow chart showing participation of American Academy of Family Physicians National Research Network members.
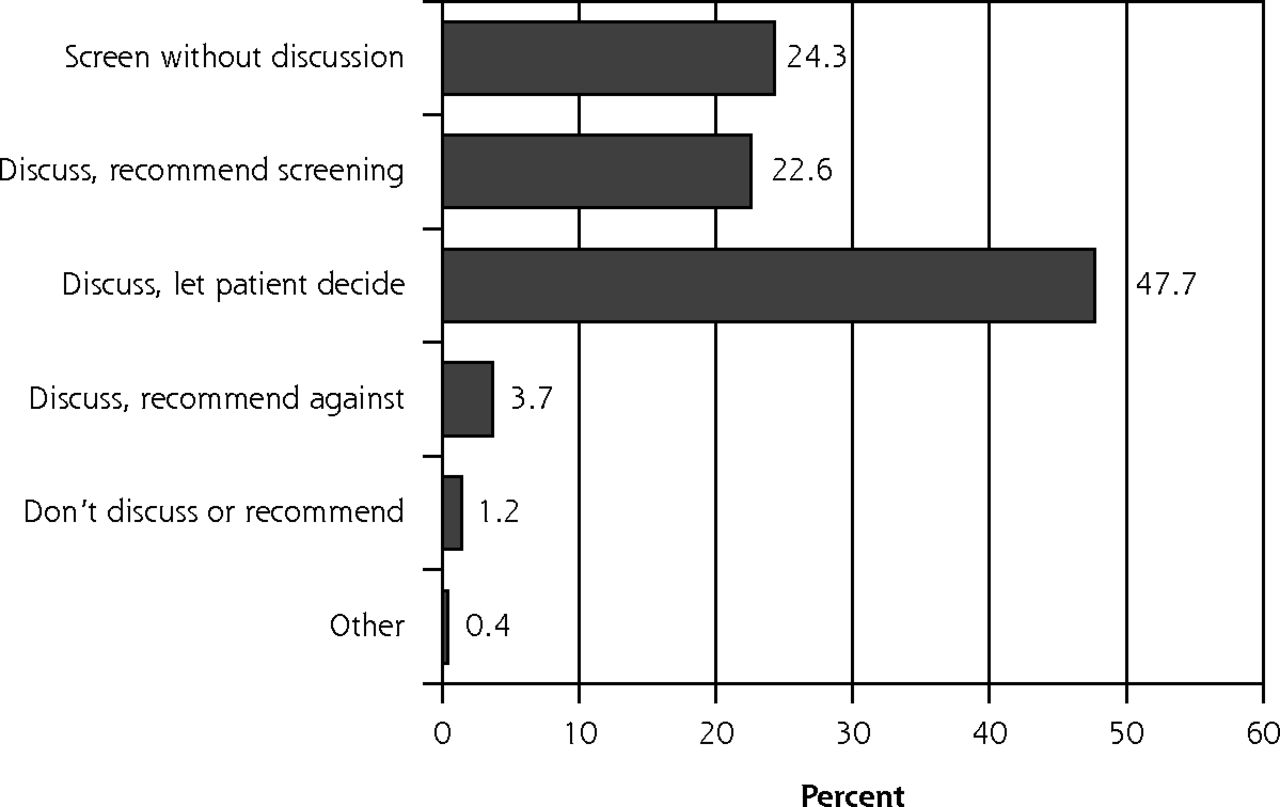
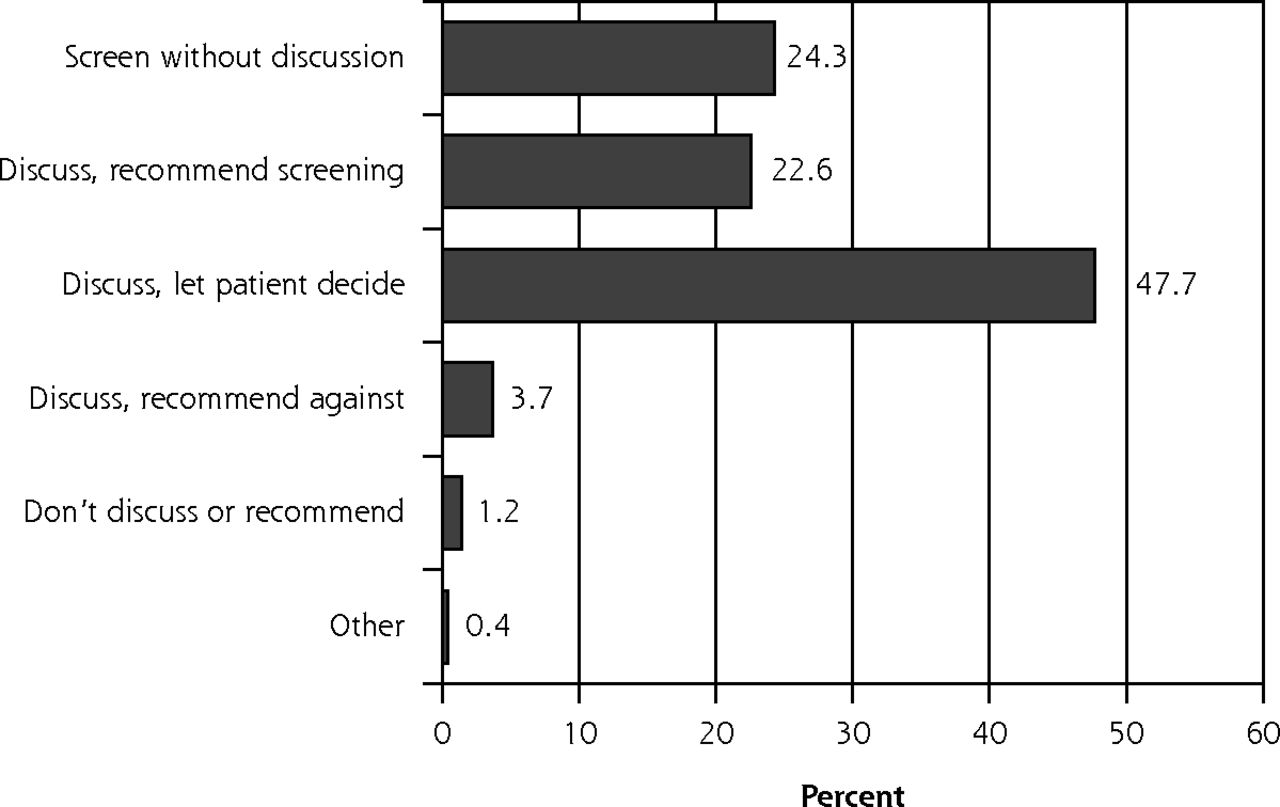
- Figure 2
Practice styles for prostate cancer screening among American Academy of Family Physicians National Research Network physician members (n = 243).

Tables
Study Sample Survey (N = 246) Characteristic Membership Survey (n = 209)a OnlineP(n = 107) Mailed (n = 139) P Valueb Years in practice, mean (SD)c 16.4 (8.5) 19.4 (8.6) 19.4 (9.1) .991 Sex, male, % (n)d 71.3 (149) 74.3 (78) 69.4 (93) .406 Academically affiliated practice, % (n) 37.3 (78) 48.4 (46) 34.8 (48) .037 -
↵a The American Academy of Family Physicians National Research Network membership survey is not completed by all member physicians.
-
↵b Online survey vs mailed survey.
-
↵c Includes 104 online and 138 mailed respondents; data missing on 4 others.
-
↵d Percentages are not based on full sample because of missing responses.
-
- Table 2
Distribution of Physician Characteristics and Responses to Screening Beliefs Indicators, by the 3 Most Common Clinical Practice Styles for Prostate Cancer Screening
Practice Style and Belief Endorsement, %a Variable Score for Beliefs Indicators, Mean (SD)b Screen Without Discussion (n = 59) Discuss, Recommend Screening (n = 55) Discuss, Let Patient Decide (n = 116) PValuec Physician characteristics Sex, male 75.9 73.6 68.7 .577 Academically affiliated practice 3.6 41.5 56.6 <.001 Beliefs indicators Screening/treatment efficacy The benefits of prostate cancer screening outweigh the risks 3.40 (1.00) 76.3 69.1 16.5 <.001 I have wondered if treatment for prostate cancer is worth it for some patients 3.65 (0.97) 50.8 64.8 87.9 <.001 Scientific evidence There is clear evidence that prostate cancer screening saves lives 2.52 (0.99) 30.5 30.9 1.7 <.001 My clinical experience is more important than research studies in how I handle screening 2.96 (1.21) 25.4 25.9 3.4 <.001 The scientific evidence does not support routine screening for prostate cancer 3.31 (0.88) 20.3 23.6 71.6 <.001 Evidence-based medicine orientation I would describe myself as someone who practices evidence-based medicine 3.97 ( 0.53) 71.2 87.3 90.5 .003 Professional experience I have lost patients to prostate cancer who might have been saved if they had been screened with PSA 2.51 (1.08) 27.6 27.8 16.4 .119 Personal experience I have lost close family members or friends to prostate cancer 2.34 (1.29) 28.8 25.9 22.4 .638 Prescreening discussion Patients should be told that it has yet to be proven that prostate cancer screening saves lives 3.82 (0.95) 35.6 61.8 90.5 <.001 Patients’ rights Patients have a right to know the implications of prostate cancer screening before they are screened 4.20 (0.70) 52.5 92.7 98.3 <.001 Patients’ expectations There is no need to educate patients about prostate cancer screening because in general they want to be screened 2.42 (1.11) 54.2 22.2 6.9 <.001 My patients frequently request the PSA test 3.87 (0.79) 83.1 73.6 63.8 .026 Patient anxiety Discussing harms and benefits of prostate cancer screening causes unnecessary anxiety in my patients 2.62 (0.96) 32.2 25.5 14.8 .024 Regret There have been times when I have regretted ordering a PSA test for a patient 2.96 (1.21) 25.4 39.6 56.9 <.001 Malpractice concerns Not ordering a PSA test puts a physician at risk for malpractice liability 3.82 (0.90) 76.3 87.3 63.8 .004 Community standards Prostate cancer screening is a standard of care in my community 4.02 (0.75) 94.8 90.9 64.7 <.001 Time barriers I do not have time to discuss the harms and benefits of prostate cancer screening with my patients 2.67 (1.06) 42.4 18.2 22.4 .005 - Table 3
Multinomial Logistic Regression Analysis of Screening Beliefs Indicators Predicting Clinical Practice Style for Prostate Cancer Screening
Discuss, Let Patient Decide vs Screen Without Discussion Discuss, Let Patient Decide vs Discuss, Recommend Screening Beliefs Indicatorsa ORb P Value ORb P Value The benefits of prostate cancer screening outweigh the risks – – 0.269 .009 There is clear evidence that prostate cancer screening saves lives – – 0.092 .012 The scientific evidence does not support routine screening for prostate cancer 3.628 .046 2.713 .040 Patients should be told that it has yet to be proved that prostate cancer screening saves 6.073 .003 – – Patients have a right to know the implications of prostate cancer screening before they are screened 10.535 .015 – – There is no need to educate patients about prostate cancer screening because in general they want to be screened 0.122 .001 – – Not ordering a PSA test puts a physician at risk for malpractice liability – – 0.271 .025 -
OR = odds ratio.
Effects are adjusted for years in practice, sex of physician, and academically affiliated practice. Dashes are used for nonsignificant beliefs indicators.
-
↵a Belief indicators are scored as endorsed (ie, agree or strongly agree) or not endorsed (neutral, disagree, or strongly disagree).
-
↵b Interpreted as the ratio of the odds of endorsing a belief indicator among physicians who reported a prostate cancer screening practice style of discuss, let patient decide vs the odds of endorsing the same belief indicator among physicians who reported the practice style of screen without discussion (first column) or discuss, recommend screening (second column).
-
Supplemental Appendix
Supplemental Appendix 1. Physician Survey on Prostate Cancer Screening
Files in this Data Supplement:
- Supplemental data: Appendix - PDF file, 3 pages, 283 KB
The Article in Brief
Primary Care Physicians' Use of an Informed Decision-Making Process for Prostate Cancer Screening
Robert J. Volk , and colleagues
Background Although most primary care physicians screen for prostate cancer, little is known about their use of advance discussions of the risks and benefits of screening, a key component of an informed decision-making process. This study examines the use of prescreening discussions about the potential benefits and harms of prostate cancer screening and explores the role of physicians' beliefs about the efficacy of prostate cancer screening.
What This Study Found There is considerable variability in primary care physicians' approaches to engaging patients in advance discussions about prostate cancer screening. Much of the variability in styles can be attributed to physicians' personal beliefs about prostate cancer screening, some of which may be amenable to change. Compared with physicians who order screening without discussion (24 percent), physicians who discuss harms and benefits with patients and then let them decide (48 percent) are more likely to believe that scientific evidence does not support screening, that patients should be told about the lack of evidence, and that patients have a right to know the limitations of screening. They are also less likely to endorse the belief that there is no need to educate patients because they want to be screened. In this study, physicians who discussed the harms and benefits and recommended the test more often expressed concerns about the legal risk associated with not screening compared with physicians who discuss and let the patient decide.
Implications
- The authors call for the use of patient decision aids and efforts to educate physicians about the shared decision-making process, including countering the false beliefs that perpetuate routine screening.




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Primary goals, information-giving and mens understanding: a qualitative study of Australian and UK doctors varied communication about PSA screening
- National Evidence on the Use of Shared Decision Making in Prostate-Specific Antigen Screening
- In This Issue: How We Think and Feel Influences Patient Care