
Abstract
PURPOSE Although the US adolescent pregnancy rate is high, use of the most effective reversible contraceptives—intrauterine devices (IUDs) and implantable contraception—is low. Increasing use of long-acting reversible contraception (LARC) could decrease adolescent pregnancy rates. We explored New York City primary care physicians’ experiences, attitudes, and beliefs about counseling and provision of LARC to adolescents.
METHODS We conducted in-depth telephone interviews with 28 family physicians, pediatricians, and obstetrician-gynecologists using an interview guide based on an implementation science theoretical framework. After an iterative coding and analytic process, findings were interpreted using the capability (knowledge and skills), opportunity (environmental factors), and motivation (attitudes and beliefs) conceptual model of behavior change.
RESULTS Enablers to IUD counseling and provision include knowledge that nulliparous adolescents are appropriate IUD candidates (capability) and opportunity factors, such as (1) a clinical environment supportive of adolescent contraception, (2) IUD availability in clinic, and (3) the ability to insert IUDs or easy access to an someone who can. Factors enabling motivation include belief in the overall positive consequences of IUD use; this is particularly influenced by a physicians’ perception of adolescents’ risk of pregnancy and sexually transmitted disease. Physicians rarely counsel about implantable contraception because of knowledge gaps (capability) and limited access to the device (opportunity).
CONCLUSION Knowledge, skills, clinical environment, and physician attitudes, all influence the likelihood a physician will counsel or insert LARC for adolescents. Interventions to increase adolescents’ access to LARC in primary care must be tailored to individual clinical practice sites and practicing physicians, the methods must be made more affordable, and residency programs should offer up-to-date, evidence-based teaching.
- intrauterine devices
- contraceptive IUD
- qualitative research
- contraceptive devices
- contraception
- physicians, primary care
- adolescent
- delivery of health care
- health services accessibility
INTRODUCTION
Despite high reported contraception use, the US adolescent pregnancy rate is one of the most elevated in the industrialized world.1,2 Bronx County in New York is among the US counties with the highest adolescent pregnancy rate. Eighty-two percent of all US adolescent pregnancies are unplanned or unintended,3 and 31% end in abortion.2 Inconsistent and incorrect contraceptive use is a major direct cause of unintended pregnancy.4,5 Many factors associated with poor adherence to contraception are obviated by use of forgettable methods, namely, intrauterine devices (IUDs) and the etonogestrel implant, collectively known as long-acting reversible contraception (LARC). Despite their safety and efficacy, only 5.5% of all US women6 and 3% of adolescents7 who use contraceptives have an IUD. Far fewer use implantable contraception. Increasing use of LARC could decrease unintended adolescent pregnancy rates.8,9
Although most adolescents access clinical services at general primary care practices,10 there are limited studies about contraception and specifically provision of LARC to adolescents in primary care. The studies that do include primary care physicians or their patients found that female patients say clinicians infrequently discuss IUDs,11 physicians often use unduly restrictive criteria when considering whether a woman is an appropriate IUD candidate,8,12 and family physicians themselves report they are unlikely to recommend IUDs to adolescents.13 Provision of LARC to adolescents in primary care has not been studied, nor do we know why family physicians are unlikely to recommend IUDs to adolescents.
Our research question was to explore New York City primary care physicians’ experiences, attitudes, and beliefs about counseling and provision of LARC to adolescents with a focus on enablers and barriers to access. Our larger objective was to inform the development of interventions to improve adolescents’ access to these forgettable contraceptive methods by increasing the proportion of physicians who either counsel about or insert LARC.
METHODS
Sampling Strategy
Participants were family physicians, generalist pediatricians, and obstetrician-gynecologists who care for female adolescents, provide at least 30% outpatient clinical time, and practice at 1 of 2 large New York medical centers in the Bronx (all 3 physician types) or Brooklyn (family physicians only). We used purposeful stratified sampling of primary care clinical sites and randomly recruited individual physicians within 6 residency sites and 11 nonresidency sites. Our goal was to interview approximately equal numbers of primary care physicians from residency and nonresidency sites and to obtain a balance between the 3 physician types. Specialists, specialty sites, and residents were not included.
Interview Guide
Because little is known about our topic, we conducted a qualitative exploratory interview study14 The interview guide (available online in Supplemental Appendix 1 at http://annfammed.org/content/11/2/130/suppl/DC1) was based on an implementation science theoretical framework.15 We explored the following domains: knowledge, skills, self-efficacy professional role and influences, belief about consequences, environmental constraints, motivation, decision process, and behavioral regulation. To obtain more realistic as opposed to idealistic responses, we wove a vignette throughout the interview guide. The interview guide was piloted with 7 physicians and modified accordingly. Pilot data were not included in the analysis.
Data Collection
After obtaining oral informed consent, a physician-researcher (S.E.R.) conducted telephone interviews until reaching saturation for each of the 3 physician types.14 The interviews were recorded and professionally transcribed.
Analysis
Analysis Team
The team was comprised of 2 experienced family physician clinical researchers, who provided patient care in 2 of the clinics from which study participants were recruited, and a graduate student in psychology, who had an interest in qualitative research and adolescent health issues but no primary care experience.
Thematic Analysis and Coding Scheme Development
During data collection the 2 physician-researchers reviewed transcripts periodically to assess the interview guide’s effectiveness, preliminarily to identify emerging themes and assess for saturation. Minor modifications were made to the interview guide. At completion of data collection, using a template style of analysis,14 team members independently identified themes, met to review transcripts excerpt by excerpt to refine a coding template, and developed an explicit codebook.16 Because all interviews were conducted by a single author, a second author listened to the recordings to ensure accuracy of transcription and to identify nuances of the interviews. We grouped our outcomes into 2 behaviors: (1) counseling, defined as discussing, mentioning, or recommending LARC to adolescents; and (2) inserting, defined as inserting the device. Coded transcripts were entered in MAXQDA 10 (VERBI GmbH) qualitative software.
Explanatory Model
After intensive reading of the completed coded data, we revisited the implementation science literature and then identified an interpretative, conceptual model for understanding our outcomes of interest. This model, the Capability, Opportunity, Motivation-Behavior system (COM-B),17 was developed to improve the design of behavior change interventions. COM-B is comprised of 3 major components influencing behavior: (1) capability, or “having the necessary knowledge and skills”; (2) opportunity, or “factors that lie outside the individual that make the behavior possible or prompt it”; and (3) motivation, or “those brain processes that energize and direct behavior.”17 All of our relevant codes apply to this model.
Achieving Reliability
Upon completing the coding list, we independently coded a subset of the data, working together until reaching conceptual coherence of the coding attributes. An explicit effort was made to search for disconfirming cases. No cases substantively deviated from our model, potentially reflecting relative flexibility and broadness of our model.
This study was approved by the Albert Einstein College of Medicine Institutional Review Board.
RESULTS
The Sample
From November 2010 through April 2011, we conducted 28 interviews (25 to 45 minutes) with 9 family physicians, 10 pediatricians, and 9 obstetrician-gynecologists. Participating physicians worked in 17 different clinical sites with 2 to 15 clinicians per site. Because of a recording device malfunction, 2 pediatric and 1 obstetrician-gynecologist interviews were not recorded. Respondents completed residency from 1977 to 2010, and 16 worked in residency training sites. Nineteen respondents have counseled adolescents about LARC. Two have ever inserted implantable contraception for an adolescent; 13 have done so with IUDs (Table 1).
Demographic Characteristics of Participating Primary Care Physicians by Physician Type
Intrauterine Contraception
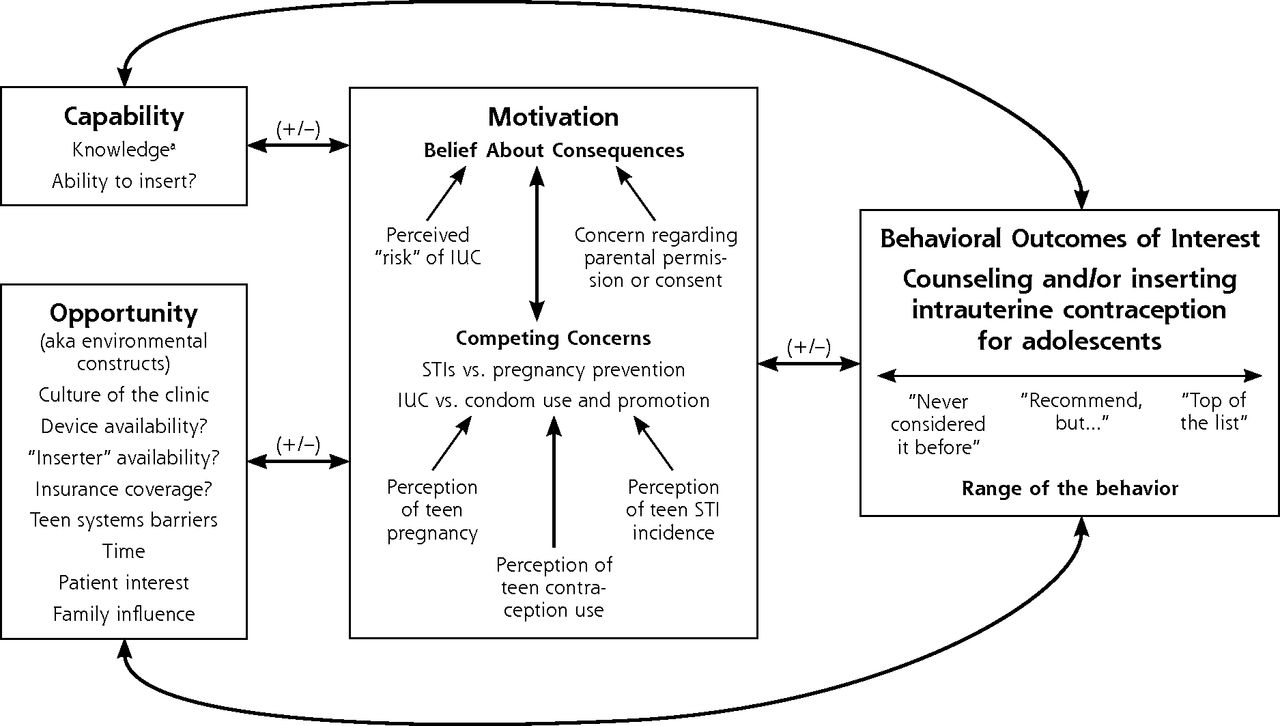
All the obstetric-gynecology practices, 60% of the family practices, and none of the pediatric practices had IUDs on site. Figure 1 depicts our results for IUDs as applied to the COM-B model. Below we describe how our results fit the model.
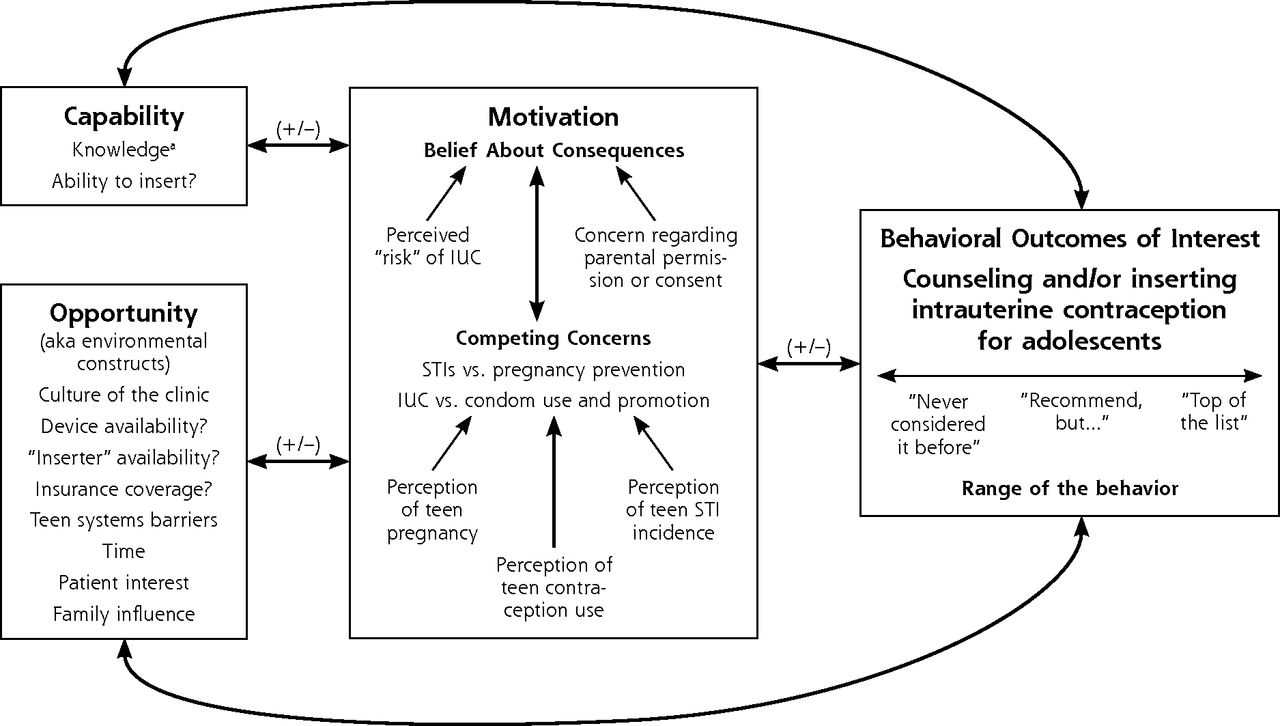
Capability, Opportunity, Motivation-Behavior system, as applied to primary care physicians practice with intrauterine contraception for adolescents.
From Michie S, van Stralen MM, West R. The behaviour change wheel: A new method for characterizing and designing behaviour change interventions. Implement Sci. 2011;6:42.
IUC = intrauterine contraception; STI = sexually transmitted infection.
a Knowledge that teen could be candidate for intrauterine contraception is prerequisite for other factors to come into play.
Capability—defined as knowledge and belief that an adolescent regardless of parity could be an IUD candidate, as well as the skills to discuss or insert IUDs—is the prerequisite activating other components of our explanatory model. Physicians (all pediatricians) who were “not aware that you could even tell adolescents about IUDs” (Pediatrician 1) never moved beyond capability to consider the components of opportunity or motivation. Most respondents practiced what they learned during residency, which often did not reflect current IUD eligibility criteria. A number of respondents did not counsel nulliparous women about IUDs because they were “trained not to offer [IUDs] to people who don’t have children” (Family physician 1).
Opportunity involves factors outside of the individual physician—environmental issues that influence behavior. A principle component of opportunity is the culture of the clinic, particularly the scope of provision of contraception to adolescents. This culture varied considerably by the type of primary care physician; pediatricians offered the most limited contraception options.
If [an adolescent is] really interested in doing oral contraceptives or other birth control, then we would refer them [out]…. I don’t prescribe birth control pills…. There are probably 2 doctors here that would feel comfortable prescribing oral contraceptives. There are no physicians of the 5 of us that do anything further (Pediatrician 6).
Physicians were more likely to counsel about IUDs at sites where colleagues were perceived to be supportive of IUD provision to adolescents, if a reproductive health champion was on site, if the physicians themselves inserted IUDs, or if there was access to a clinician inserter. One family physician worked at a site with a strong focus on women’s reproductive health, where,
…there is a provider who is very interested in women’s health…if we have questions we ask her…people really are pro-contraception, pro-choice in general in the clinic…residents being trained [in IUD insertion] by the faculty…just makes it more normal” (Family physician 2).
Physicians at residency sites appeared to offer a wider range of contraception options.
Another opportunity issue was the perception that certain adolescents, specifically adolescent mothers, were more interested in IUDs. Thus respondents limit their counseling:
We’re using the IUD a lot in young women who are postpartum. I’m trying to talk about it with my younger patients as well, but many of them seem to be a little less receptive to the idea than women who have had the experience of getting pregnant (Family physician 2).
Clinicians also indicated that potential parental resistance to IUD use and limited time alone with adolescents influenced their willingness to counsel or insert the devices. A few respondents were uncomfortable with the idea of IUD use (compared with prescribing contraceptives) without parental permission or consent. “[I] could see a parent flipping out if they found that out an IUD was put in without their knowledge” (Pediatrician 5).
Cost of the device was the main opportunity barrier identified by those physicians who inserted IUDs for adolescents.
[My colleagues] don’t have an issue placing or providing long-term contraception for adolescents. The problem is access [to the device] (Obstetrician-gynecologist 4).
Accessing the device is related to the high cost of the device and insurance:
The insurance issues and confidentiality tend to be problematic. The patient is concerned about her family knowing that she had the IUD inserted…the family may well…get an office bill (Family physician 7)
Some physicians who worked in Federally Qualified Health Centers perceived better access to the device because the full scope of contraception provision aligned with the clinic’s mission, and the administration supported IUD provision despite any potential financial burden. Inability to offer same-day insertions was another barrier.
Motivation was the largest and most complex piece of our explanatory model because it involved several interrelated constructs. One construct, belief about consequences, includes a perception of competing concerns, or tension between (1) sexually transmitted infection (STI) vs pregnancy prevention and (2) IUD vs condom use. Many respondents feared that forgettable contraception results in more forgotten condoms:
[With IUD] I would be worried [adolescents] would then feel freer to have completely unprotected sex and acquire more STIs…[more then with oral contraceptive pills] because they’re not reminded every day to use something (Obstetrician-gynecologist 5).
Others expressed concern that the IUDs’ high efficacy in pregnancy prevention results in less condom or dual protection (condom plus prescription contraception) use: “They’re protected from their worst fear, which is having a baby. I think it gives [adolescents] license to do whatever they want without protection” (Family physician 5). In general, it appeared that the greater the perceived risk of STI, the less likely a physician would counsel about IUDs. All respondents counseled patients about condom use, like this physician who “strongly encourage[s] condom use regardless of anything else and the importance of that for protecting against STIs” (Pediatrician 3).
Belief about consequences also included perceptions about risks inherent to the IUD device itself. Some physicians, even some who inserted IUDs, expressed apprehension stemming from non–evidence-based, outdated device-related concerns. For example, one physician who inserted IUDs for adolescents said, “I’m always also thinking in the back of my head, boy, I hope [adolescent with an IUD] is still using condoms so that she’s not at a higher risk for an infection with this foreign body” (Obstetrician-gynecologist 1). Physicians reported that clear clinical guidelines supporting IUD use in adolescents would make them more comfortable inserting these devices. For those who do insert, this concern is outweighed by their motivation to prevent pregnancy. “The teenager who is sexually active probably ought to have as her number 1 priority not getting pregnant. Therefore, my own bias is to offer her the most effective contraception” (Obstetrician-gynecologist 2).
Confluence of COM-B Factors Influencing Behavior Change
A few respondents described the process by which their behavior related to IUD provision to adolescents changed as a result of capability, opportunity, and motivation factors. One physician said,
[I] was trained at a time when we didn’t use IUDs in adolescents or nulliparous women because we were concerned about PID [pelvic inflammatory disease] and infertility…. I learned the new evidence from [champion] and the reproductive health team. It was a jolt to my way of thinking. I was open to changing because it was a great new option…. So the barrier was knowledge…. I [asked] but what about infection? [Champion] said the evidence does not show an increased rate of infection with IUDs. …I worked in an office with other people, [who were] using a lot of IUDs…. It was, for whatever reason, something I believed and then changed my practice…because I really believe in teenagers not getting pregnant and offering them what I can (Family physician 6).
Implantable Contraception
Only 2 sites (both family medicine) had implantable contraception. Few physicians counseled about this option because they had limited knowledge (capability) and access (opportunity). We could not develop a COM-B figure for implantable contraception because too few respondents discussed it.
DISCUSSION
Our study of New York City primary care physicians gives us important insights into clinical practices regarding counseling and provision of forgettable contraception to adolescents. A number of physicians, in particular pediatricians, did not know that a nulliparous adolescent can be an appropriate IUD candidate and consequently reported that they never counsel about this option. For those physicians who did know, specific enablers to counseling included availability of the device in the clinic, a supportive clinic culture, the ability to insert IUDs or having access to someone who could insert the device, and a belief in the positive consequences with IUD use. The physicians’ perceptions of adolescent pregnancy and STI risk notably influenced their attitudes toward IUDs in adolescents. Lack of access to the device itself was the main barrier for those physicians who insert IUDs. Almost all respondents had limited access to and little or no experience with implantable contraception.
Most pediatricians in our sample reported limited knowledge of and some discomfort with prescribing contraceptives in general. This finding is consistent with those of other studies that describe pediatricians’ contraception knowledge gaps and their interest in additional training in pregnancy prevention.18,19 Other respondents, including some who inserted IUDs, had LARC-specific knowledge gaps and worried about non–evidence-based risk of the IUD device itself. Some gaps reflected outdated information from residency training. Differences in knowledge and comfort may be attributable to different approaches of the primary care specialties. Although all the professional medical organizations endorse STI counseling and prescribing contraception, the American Academy of Pediatrics policy statement on contraception and adolescents does not support implants as a first-line method and discourages IUD use.20 In contrast, the American College of Obstetricians and Gynecologists21 and the US Medical Eligibility Criteria for Contraceptive Use22 recommend LARC for adolescents and nulliparous women. The American Academy of Family Practitioners policy on sexuality and contraception for adolescent patients does not explicitly mention LARC.23 These inconsistent policies may account for some of the variation in counseling practices.
A challenge in promoting adolescents’ access to LARC is addressing physicians’ concerns about STIs. Surprisingly, almost all respondents described competing concerns between STI and pregnancy prevention; many framed this issue as condom vs LARC use. Physician concern about STIs is understandable. Urban adolescents have disproportionately high STI rates.24 Because STI evaluation and treatment are within the scope of primary care practice, an adolescent with STI symptoms is likely to consult her primary care physician.25 But a substantial proportion of unintended adolescent pregnancy remains invisible to the physician because abortion is rarely offered in the primary care setting. Yet Bronx adolescents aged 15 to 19 years experience more pregnancies than infection with Chlamydia trachomatis, the STI with the highest incidence in the Bronx.26,27
Ideally all at-risk individuals would use dual protection, meaning protection against pregnancy and STIs, but few do. Nationally only 6.6% to 8.5% of young women used a condom and oral contraception at their last intercourse.28,29 The limited studies exploring adolescents’ dual protection and LARC found decreased condom use in those women who use LARC, yet the studies are all confounded by selection bias.30 We do not know whether those few adolescents who use dual protection would continue to use condoms if using LARC.
Consistent with other studies, the high up-front cost for an IUD and insurance are the major barriers to IUD insertion.31 Removing financial barriers regionally increases IUD use.32,33 This barrier may be reduced nationally with the Department of Health and Human Services classification of contraceptives as preventive care; under the Affordable Care Act some women have been able to receive contraception without a co-payment starting August 2012. A cost-saving measure would be approval of generic LARC, which are already available worldwide.
Our study has limitations. First, less than one-half of invited participants completed an interview. It is probable that respondents more frequently counseled or inserted IUDs compared with those who did not participate. Second, despite the theoretically controversial nature of our research topic and the interviewer’s efforts to minimize social desirability bias, interviewees knew that the interviewer was a physician whose research interest is LARC use and adolescents. This knowledge likely resulted in respondents’ overestimating their LARC counseling. Third, we conducted interviews by telephone rather than in person; rapport was not difficult to establish, and we found that the added flexibility of scheduling outweighed any potential challenges of not being able to assess body language. A fourth is generalizability. Laws concerning provision of reproductive health care to adolescents and parental involvement mandates vary by state. Primary care physicians in other states likely face additional barriers.
Despite these limitations, our study had strengths, including the rigor with which we developed the interview guide and conducted the analysis and the manner in which our findings fit with the established COM-B behavior change system.17 Both our interview guide and interpretative conceptual model use an implementation science theory approach. COM-B, in addition to being a model of behavior, will provide us with a basis for designing and measuring future interventions.
There are numerous barriers to adolescents’ accessing LARC in primary care that include financial concerns, the clinical environment, and physicians’ knowledge, attitudes, and beliefs. Primary care physicians weigh many factors when considering provision of forgettable contraception to adolescents, and they vary considerably in their comfort level with contraception provision overall. Future research is needed to explore specific strategies to influence physicians’ behavior with their LARC counseling. A concrete step to address the persistent public health issue of adolescent pregnancy is optimizing access to reliable, forgettable forms of reversible contraception. Increasing access to LARC in primary care will improve the likelihood that each interested woman is able to select the most effective method that is right for her. Interventions to increase access for adolescents to LARC in primary care must be tailored to individual clinical practice sites and practicing clinicians, the devices must be made more affordable, and up-to-date, evidence-based teachings should be offered in all primary care residency programs.
Acknowledgments:
We acknowledge the primary care physicians who participated in this study. Without their willingness to take time out of a busy schedule this research would not be possible.
Footnotes
-
Conflicts of interest: the authors report none.
-
To read or post commentaries in response to this article, see it online at http://www.annfammed.org/content/11/2/130.
-
Funding support: This project is funded through NIH NICHD K23HD067247 –01 (Rubin) and the CTSA Grant UL1 RR025750, KL2 RR025749 and TL1 RR025748 from the NCRR, a component of the NIH, and NIH Roadmap for Medical Research.
-
Previous presentations: Findings from this study were presented at the North American Forum on Family Planning, Washington DC, September 2011 poster presentation and as an abstract published September 2011 issue of Contraception; at the North American Primary Care Research Group Annual Meeting, Banff, Canada, November 2011 as an oral presentation; at the Society for Adolescent Health and Medicine’s Annual Meeting, New Orleans, LA, March 2012 as an oral presentation and abstract published in Journal of Adolescent Health, February 2012 supplement.
- Received for publication February 11, 2012.
- Revision received July 12, 2012.
- Accepted for publication July 24, 2012.
- © 2013 Annals of Family Medicine, Inc.
References




{kind=link}
Jump to section
Related Articles
Cited By...
- Understanding barriers to using long-acting reversible contraceptives (LARCs) in primary care: a qualitative evidence synthesis
- Prescription contraception use: a cross-sectional population study of psychosocial determinants
- Intrauterine Devices at Six Months: Does Patient Age Matter? Results from an Urban Family Medicine Federally Qualified Health Center (FQHC) Network
- Evidence-Based Selection of Candidates for the Levonorgestrel Intrauterine Device (IUD)
- In This Issue: Finding the Sweet Spot in Health Care