
Article Figures & Data
Figures
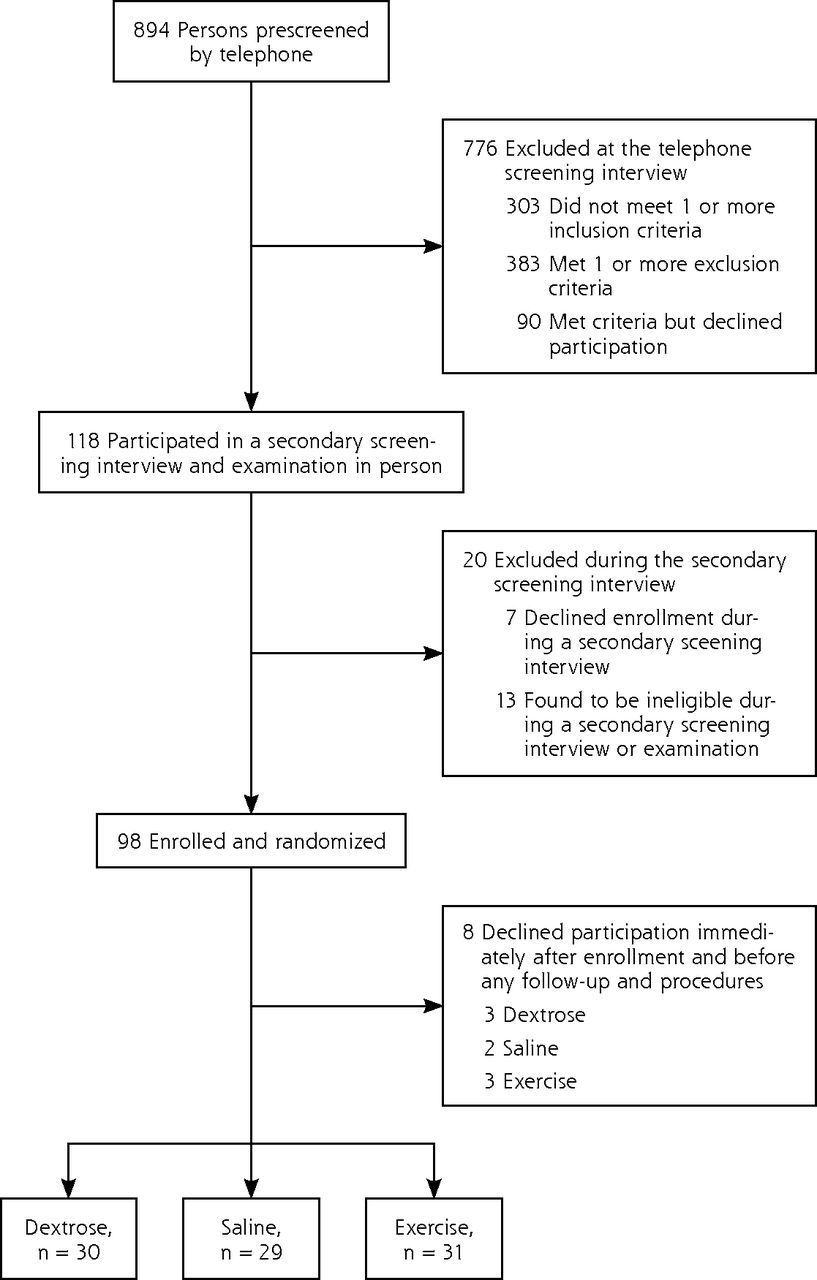
- Figure 1
Screening, enrollment, and randomization.
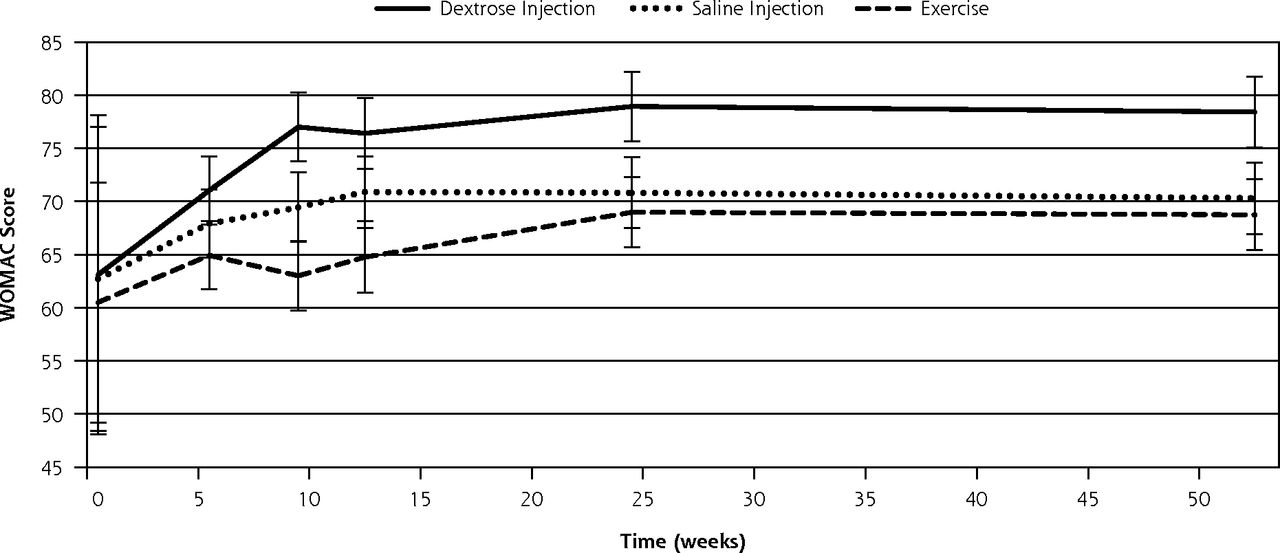
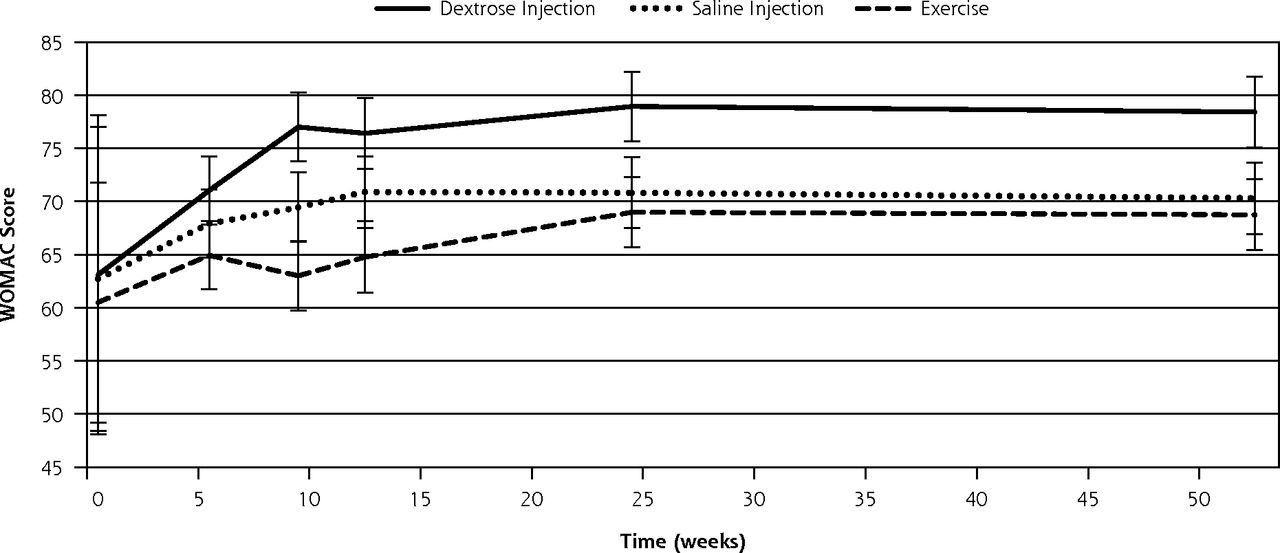
- Figure 2
Change in WOMAC composite scores over 52 weeks (± standard error).
WOMAC = Western Ontario McMaster University Osteoarthritis Index.
Note: WOMAC is scored on a range of 0 to 100 points, with higher scores indicating better knee-related quality of life. Nonoverlapping confidence intervals indicate significance of change in dextrose scores compared with change in scores of both saline (P <.05) and exercise (P <.05) groups.

Tables
Injection Type Solution Injection Technique Dextrose Intra-articular 25% dextrose In a 10-mL syringe: -
5 mL 50% dextrose
-
5 mL lidocaine
-
1% saline
6.0 mL was injected using an inferomedial approach Extra-articular 15% dextrose 22.5 mL distributed in 3, 10-mL syringes (7.5 mL each) using the following recipe: -
6.75 mL 50% dextrose
-
4.5 mL 1% lidocaine
-
11.25 mL 0.9% saline
Up to 15 subdermal injections were placed, and 0.5 mL of 15% solution was injected using a peppering technique with a 25-gauge needle at each ligament-bone insertion. Each puncture site allowed for placement of solution at up to 3 ligament-bone insertions using a skin-sliding technique (withdrawing the needle to just below the skin and reinserting into an adjacent area without removing from the initial puncture site), allowing for the placement of up to 22.5 mL of solution Saline control Intra-articular -
5 mL 0.9% sodium chloride
-
5 mL 1% lidocaine
Injection technique identical to intra-articular injections above Extra-articular 22.5 mL distributed in 3, 10-mL syringes (7.5 mL each) using the following recipe: -
18 mL 0.9% sodium chloride
-
4.5 mL 1% lidocaine
Injection technique identical to extra-articular above -
Characteristic Dextrose Saline Exercise P Value No. 30 29 31 Female, No. (%) 19 (63) 20 (69) 21 (68) 0.82 Age, mean (SD), y 56.8 (7.9) 56.8 (6.7) 56.4 (7.0) 0.97 Duration of knee pain, No. (SD), mo 79.8 (62.9) 108.0 (99.5) 60.4 (71.6) 0.08 Body mass index, No. (%) ≤25 10 (33) 8 (28) 6 (19) 25–30 6 (20) 11 (38) 12 (39) 0.44 ≥30 14 (47) 10 (34) 13 (42) Prior knee intervention, No. (%) History of arthroscopic surgery 7 (23) 5 (17) 7 (23) 0.84 Physical therapy 6 (20) 3 (27) 16 (52) 0.08 Hyaluronic acid injection 3 (10) 0 (0) 2 (6) 0.62 Corticosteroid injection 4 (13) 1 (9) 2 (6) 0.79 Glucosamine 7 (23) 5 (17) 8 (26) 0.82 Characteristic Dextrose Saline Exercise P Value X-ray Kellgren-Lawrence osteoarthritis severity scorea 1–2 (mild osteoarthritis) 11 12 9 .35 3–4 (moderate to severe osteoarthritis) 14 9 14 WOMAC total score (SD) [range]b 63.1 (15.0) [34.6–93.1] 62.7 (14.3) [34.3–90.8] 60.5 (11.3) [35.7–77.0] .73 Pain score (SD) [range] 66.8 (14.9) [35.0–95.0] 66.7 (16.1) [30.0–95.0] 63.2 (13.1) [35.0–90.0] .49 Stiffness score (SD) [range] 57.1 (19.9) [25.0–87.5] 53.9 (14.2) [25.0–87.5] 55.3 (18.0) [12.5–100.0] .73 Function score (SD) [range] 65.2 (15.8) [39.7–96.9] 67.6 (17.5) [35.3–100.0] 61.9 (12.7) [36.8–86.8] .36 Knee pain scalec Treated Knee n=43 Untreated Knee n=17 Treated Knee n=41 Untreated Knee n=17 Treated Knee n=47 Untreated Knee n=15 TreatedPValue UntreatedPValue Pain frequency score (SD) 2.5 (0.9) 0.6 (1.1) 2.4 (0.9) 0.9 (0.9) 2.5(0.9) 0.7 (1.0) .52 .69 Pain severity score (SD) 1.8 (0.8) 0.5 (1.1) 1.7 (0.7) 0.6 (0.8) 1.7(0.8) 0.4 (0.7) .42 .74 -
WOMAC = Western Ontario McMaster University Osteoarthritis Index.
-
↵a Kellgren-Lawrence scores range from 1 to 4.
-
↵b The theoretical range in this study is 0 to 100, with higher values indicating better knee-related quality of life.
-
↵c The theoretical range of scores for knee pain frequency is 0 to 4 and for knee pain severity is 0 to 5, with higher values indicating worse symptoms.
-
Score Week 5 Week 9 Week 12 Week 24 Week 52 WOMAC composite score change, mean (SE) Dextrose 7.94 (3.21) 13.91 (3.23)a 13.31 (3.32)b 15.85 (3.26)a 15.32 (3.32)a Saline 5.22 (3.21) 6.75 (3.27)a 8.19 (3.37)b 8.12 (3.33)a 7.59 (3.36)a Exercise 4.42 (3.21) 2.51 (3.26)a 4.26 (3.36)b 8.48 (3.28)a 8.24 (3.33)a Subscale score change, mean (SE) Pain Dextrose 8.17 (3.49) 14.00 (3.52)a 11.78 (3.62)b 15.50 (3.56)a 14.18 (3.62) Saline 3.28 (3.50) 5.29 (3.56)a 5.79 (3.67)b 6.40 (3.63)a 7.38 (3.67) Exercise 4.53 (3.51) 3.44 (3.55)a 4.89 (3.66)b 8.07 (3.60)a 9.24 (3.63) Stiffness Dextrose 7.08 (4.50) 14.17 (4.53)c 13.49 (4.67)b 14.85 (4.58) 15.55 (4.66) Saline 8.62 (4.51) 9.12 (4.59)c 12.22 (4.73)b 10.40 (4.67) 9.97 (4.72) Exercise 3.63 (4.51) 0.14 (4.58)c 3.13 (4.71)b 8.18 (4.61) 8.31 (4.68) Function Dextrose 8.57 (3.27) 13.58 (3.30)a 14.61 (3.40)a 17.19 (3.33)a 16.25 (3.39)a Saline 3.77 (3.28) 5.85 (3.34)a 6.63 (3.44)a 7.62 (3.40)a 5.46 (3.44)a Exercise 5.10 (3.28) 4.00 (3.33)a 4.89 (3.43)a 9.30 (3.35)a 7.31 (3.40)a -
WOMAC = Western Ontario McMaster University Osteoarthritis Index.
-
Notes: Numbers of participants for measurement points are as follows. Week 5: n = 30 dextrose, n = 29 saline, n = 28 exercise. Week 9: n = 30 dextrose, n = 26 saline, n = 27 exercise. Week 12: n = 27 dextrose, n = 24 saline, n = 25 exercise. Week 24: n = 28 dextrose, n = 25 saline, n = 27 exercise. Week 52: n = 26 dextrose, n = 25 saline, n = 26 exercise. Repeated measures analysis of variance compared between-group total and subscale WOMAC scores after adjusting for baseline scores, age, sex, and body mass index.
-
↵a Dextrose outperformed saline (P <.05) and exercise (P <.05); no statistically significant differences between saline and exercise.
-
↵b Dextrose outperformed exercise (P <.05); no statistically significant differences between dextrose and saline, and between saline and exercise.
-
↵c Dextrose outperformed exercise (P <.05); saline outperformed exercise (P <.05); no statistically significant differences between dextrose and saline.
-
- Table 5
Change in Knee Pain Scale Pain Frequency and Pain Severity Scores in Individual Treated Knees Over Time
Measure Week 5 Week 9 Week 12 Week 24 Week 52 KPS pain frequency score, mean (SE) [No.] Dextrose −0.55 (0.26) [43] −0.84a (0.25) [42] −0.87a (0.27) [38] −1.19a (0.25) [40] −1.20a (0.21) [37] Saline −0.26 (0.26) [40] −0.32 (0.25) [37] −0.31 (0.27) [36] −0.48 (0.25) [37] −0.60 (0.21) [38] Exercise −0.15 (0.25) [38] −0.22 (0.24) [40] −0.12 (0.26) [37] −0.49 (0.24) [39] −0.40 (0.21) [38] KPS pain severity score, mean (SE) Dextrose −0.25 (0.26) −0.48 (0.25) −0.51 (0.27) −0.92a (0.25) −0.92a (0.21) Saline −0.07 (0.26) −0.19 (0.25) −0.16 (0.27) −0.26 (0.25) −0.32 (0.21) Exercise −0.07 (0.25) −0.15 (0.24) −0.06 (0.26) −0.33 (0.24) −0.11 (0.21) -
KPS=knee pain scale.
-
Repeated measures analysis of variance compared between-group KPS scores after adjusting for baseline scores, age, sex, and body mass index.
-
↵a Change in dextrose score was greater than change in saline (P <.05) and exercise (P <.05) scores, and there were no statistically significant differences between saline and exercise scores.
-
The Article in Brief
Dextrose Prolotherapy for Knee Osteoarthritis: A Randomized Controlled Trial
David Rabago , and colleagues
Background Knee osteoarthritis is a common, debilitating, chronic disease. This study tests the effectiveness of prolotherapy-an injection using a sugar solution to relieve musculoskeletal pain-for knee osteoarthritis.
What This Study Found Dextrose prolotherapy offers sustained improvement of pain, function, and stiffness for patients with knee osteoarthritis. Ninety adults with at least 3 months of painful knee osteoarthritis received dextrose prolotherapy injections, saline injections, or at-home exercise. Injections were done at 1, 5, and 9 weeks with as-needed additional treatments at weeks 13 and 17. Patients receiving dextrose prolotherapy improved more at 52 weeks and reported significantly better function than patients receiving saline and exercise. Individual knee pain scores also improved more in the prolotherapy group. Patient satisfaction with prolotherapy was high and no adverse events were reported.
Implications
- With most of the population showing evidence of osteoarthritis by the age of 65 years, the authors call for larger studies to compare the effectiveness of prolotherapy for knee osteoarthritis with other therapies.
Correction
In Table 1, under Solution, the components for intra-articular 25% dextrose erroneously contained 1% saline. There is no saline in the intra-articular injection, just the specified 5 mL 50% dextrose and 5 mL 1% lidocaine.




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Highlighting the Advantages and Benefits of Non-NSAID Treatment After Total Knee Arthroplasty: A Cross-sectional Study
- Decellularized Articular Cartilage Microparticles for Expansion of Mesenchymal Stem Cells and Zonal Regeneration of Articular Cartilage
- Efficacy of Intra-Articular Hypertonic Dextrose (Prolotherapy) for Knee Osteoarthritis: A Randomized Controlled Trial
- Ischiofemoral impingement due to a lipoma of the ischiofemoral space
- In This Issue: Practice Change--Context Matters