


Abstract
PURPOSE We undertook a study to evaluate the effects of medical home transformation on job satisfaction in the primary care setting.
METHODS We collected primary data from 20 primary care practices participating in medical home pilot projects in Rhode Island and Colorado from 2009 to 2011. We surveyed clinicians and staff about the quality of their practice environments (eg, office chaos, communication, difficulties in providing safe, high-quality care) and job satisfaction at baseline and 30 months, and about stress, burnout, and intention to leave at 30 months. We interviewed practice leaders about the impact of pilot project participation. We assessed longitudinal changes in the practice environment and job satisfaction and, in the final pilot year, examined cross-sectional associations between the practice environment and job satisfaction, stress, burnout, and intention to leave.
RESULTS Between baseline and 30 months, job satisfaction improved in Rhode Island (P =.03) but not in Colorado. For both pilot projects, reported difficulties in providing safe, high-quality care decreased (P <.001), but emphasis on quality and the level of office chaos did not change significantly. In cross-sectional analyses, fewer difficulties in providing safe, high-quality care and more open communication were associated with greater job satisfaction. Greater office chaos and an emphasis on electronic information were associated with greater stress and burnout.
CONCLUSIONS Medical home transformations that emphasize quality and open communication while minimizing office chaos may offer the best chances of improving job satisfaction.
- patient-centered medical home
- job satisfaction
- practice environment
- primary care
- quality culture
- office chaos
- transformation
- practice-based research
INTRODUCTION
Primary care can improve health outcomes and the overall performance of the health system.1,2 Primary care physicians, however, report lower job satisfaction than other physicians,3 and job dissatisfaction has been identified as a potential cause and result of quality problems in physician practices.4 Improving the practice work environment may enhance primary care job satisfaction.4–7
In theory, patient-centered medical homes (PCMHs, or medical homes) improve job satisfaction by promoting better work environments, increasing the quality of care, and enhancing practice resources.7–9 In theory, medical homes combine the 4 principles of primary care (first contact with the health system, continuity of care with a personal physician, a focus on the whole person, and coordination of care across the continuum), with an emphasis on care that is patient centered, team based, evidence based, and optimized through information technology.10 The ability of medical home interventions to achieve their goals, including improved professional satisfaction, is subject to empirical evaluation, however.11,12
Better job satisfaction (specifically, lower burnout) has been reported in a single-practice pilot project conducted within the Group Health Cooperative.13 These findings have not yet been replicated elsewhere, and the specific factors that may mediate medical home effects on job satisfaction have not been identified. To address these gaps, we focused our study on 3 main goals. First, we evaluated longitudinal effects of 2 medical home pilot projects on multiple dimensions of practice environment and job satisfaction. Second, at the conclusion of these projects, we explored cross-sectional relationships between dimensions of practice context and clinician and staff satisfaction, stress, burnout, and intention to leave. Third, we sought to understand the benefits and challenges of medical home transformation using qualitative methods.
Published research identifies 3 main aspects of the practice environment affecting job satisfaction in primary care. First, clinicians and staff are more satisfied when their organizational cultures emphasize quality and communication.4,9,14–16 Second, a chaotic office atmosphere is associated with job dissatisfaction and stress.6,7 Third, clinicians and staff are less satisfied when they face difficulties in providing safe, high-quality care.4,9
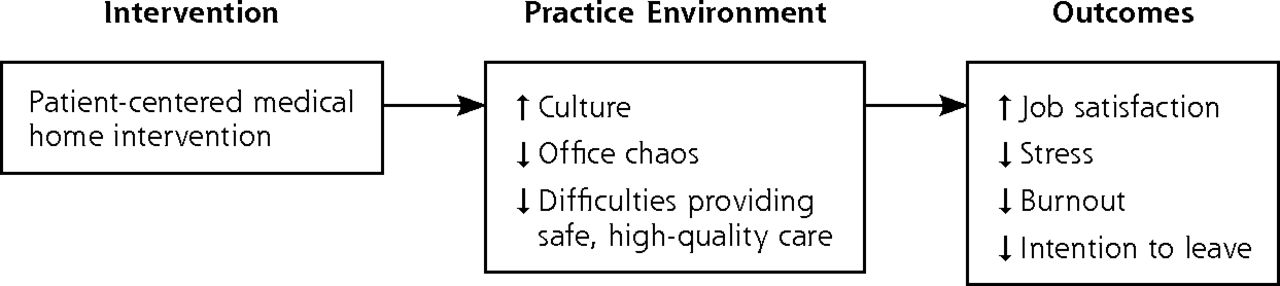
Our study addressed 2 related hypotheses (Figure 1). First, medical home pilot practices would report improvements over time in practice environment and job satisfaction. Second, at each pilot project’s conclusion, practices with better practice environments (ie, lower levels of chaos and difficulty providing safe, high-quality care) would have greater job satisfaction and lower stress, burnout, and intention to leave.
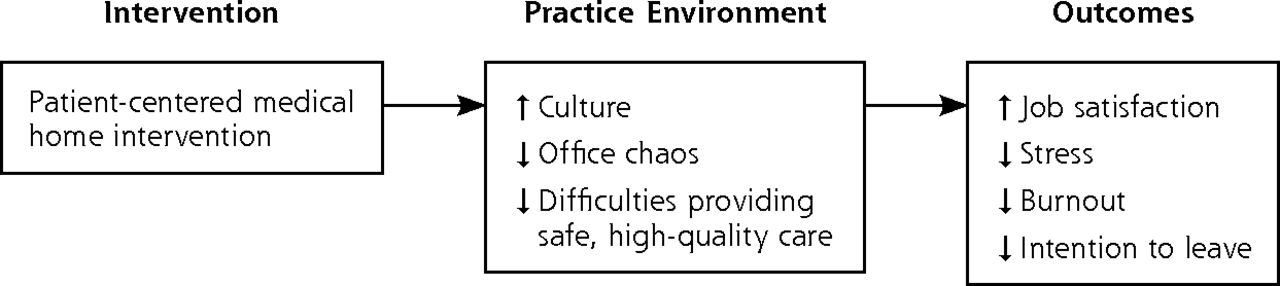
Conceptual framework.
METHODS
Study Sample
We collected data at baseline and 30 months from 20 primary care practices participating in medical home pilot projects in Rhode Island (5 practices, 28 physicians) and Colorado (15 practices, 50 physicians). Rhode Island and Colorado were 2 of the earliest multipayer PCMH initiatives and therefore were selected by the Commonwealth Fund for evaluation. Although both pilot projects targeted small to medium-sized practices (9 or fewer physicians), they had different payer and clinician environments.
The Rhode Island Chronic Care Sustainability Project (Rhode Island pilot project), convened by the state and 3 major commercial payers, began in October 2008 and ran 3 years. Each practice received a monthly fee of $3 to $4.50 per member based on its PCMH recognition level (from the National Committee for Quality Assurance [NCQA]), financial support for a nurse care manager, assistance from a “transformation coach,” and opportunities to participate in learning collaboratives.
The HealthTeamWorks initiative (Colorado pilot project), convened by HealthTeamWorks and 7 commercial and Medicaid payers, began in May 2009 and lasted 3 years. Each practice received a fee of $4 to $8 per member based on its PCMH recognition level (from the NCQA), performance-based payments, transformation coaching, and learning collaborative sessions.
The design elements and changes implemented by the practices from baseline to 30 months in both pilot projects are shown in Supplemental Appendixes 1 and 2.
Survey Instrument
We designed a written survey instrument to collect information on 3 aspects of the practice environment: organizational culture, office chaos, and difficulties in providing safe, high-quality care.
We assessed organizational culture by asking respondents to assess their practice’s emphasis on quality (5 items; Cronbach α = 0.90), electronic information (2 items; Spearman correlation = 0.77), and open communication between clinicians and staff (1 item). Questions came from the Quality Emphasis and the Information and Communication Emphasis scales of the Minimizing Error, Maximizing Outcomes (MEMO) clinician survey instrument.6,7 Office chaos was measured using a single MEMO item rating the office atmosphere from “calm” to “chaotic.”7 We measured difficulties providing safe and high-quality care by drawing 2 items from a prior survey of Massachusetts primary care practices (Spearman correlation = 0.75).17
The survey instrument included 4 outcome measures: job satisfaction, stress, burnout, and intention to leave. Job satisfaction was measured at baseline (wave 1) and 30 months (wave 2) using a single item assessing global job satisfaction. Stress, burnout, and intention to leave were measured at 30 months only. For burnout, we used 1 item highly correlated with the Maslach Burnout Inventory.18 For intention to leave, we asked respondents about their likelihood of leaving a practice within 2 years. The survey instrument appears in Supplemental Appendix 3.
Survey Administration
We administered the clinician and staff surveys for both waves by mailing and e-mailing questionnaires to each pilot practice leader, who distributed them to clinicians and staff. All clinicians (physicians, physician assistants, and nurse practitioners) and other staff (medical assistants, care coordinators, nurses, office managers, and administrative support staff) in these practices were eligible to receive the questionnaires.
Interviews
We conducted 3 sets of hour-long, semistructured interviews with practice leaders at baseline, 18 months, and 30 months. Practice leaders were physicians responsible for spearheading transformation efforts and often held formal leadership roles, although some were informal champions of medical home transformation. Each interview was conducted by at least 2 authors and included open-ended questions exploring the effects of medical home transformation on job satisfaction and related constructs. Specific questions evolved across the interview waves, congruent with progression of the medical home pilots. The interview protocols appear in Supplemental Appendix 4.
Data Analysis
To assess longitudinal differences in survey responses, we created dichotomous variables using previous MEMO thresholds6 or median responses. We assessed differences in responses at baseline and at 30 months using Fisher exact tests with significance at P <.05. In longitudinal analyses, standard errors could not account for clustering by physician practice, because practice identifiers were absent from the baseline survey responses.
In cross-sectional analyses of survey responses in the final year of each pilot project, we fit logistic regression analyses with job satisfaction, stress, burnout, and intention to leave as the dependent variables, and characteristics of the practice environment (organizational culture, office chaos, and difficulties in providing safe, high-quality care) as the independent variables, controlling for sex, employment length, and pilot project as potential confounders. For stress, burnout, and intention to leave, we used dichotomous variables based on thresholds established by Linzer et al.7 We used generalized estimating equations to account for clustering of observations within practices.19 All statistical analyses were performed using SAS version 9.3 (SAS Institute).
We analyzed the qualitative data using thematic analysis.20 First, we agreed on a coding scheme that reflected 3 main categories in our conceptual framework: organizational culture, office chaos, and difficulties providing safe, high-quality care. One author (S.A.) then coded interview transcript data using ATLAS.ti version 6.2 qualitative software (ATLAS.ti GmbH), clarifying coding decisions as needed with the other authors. We established coding reliability with a second, independent coder for approximately 15% of the transcripts (κ = 0.86, percent agreement = 0.90).
After completing the initial coding, we sorted the data by code to identify similarities and differences across cases. All investigators discussed and refined preliminary results of the qualitative analysis and compared these with results from the quantitative data. Finally, we selected quotes to illustrate the key themes that emerged from the interviews.
The study was approved by institutional review boards at the Harvard School of Public Health and RAND.
RESULTS
Survey response rates were 61% at baseline and 80% at 30 months. (The sample size changed between time points because of the hiring of care coordinators and considerable growth in one of the practices.) Practice and respondent characteristics at baseline are summarized in Table 1.
Characteristics of Practices and Survey Respondents at Baseline
Effects of Medical Home Pilot Project Participation
The effects of medical home pilot project participation on organizational culture, office chaos, difficulties in the practice environment, and job satisfaction are summarized in Table 2. Key themes and illustrative interview quotes on the perceived benefits and challenges associated with transformation to PCMHs appear in Table 3.
Changes in the Practice Environment and Job Satisfaction at Baseline and 30 Months
Key Themes Emerging as Benefits and Challenges of Medical Home Transformation
Practice Environment
Project participation was associated with a reduction in the percentage of respondents who reported “sometimes” or “frequently” experiencing difficulties providing safe, high-quality care at 30 months (P <.001). There also were trends, which did not reach statistical significance, toward stronger emphasis on quality (P = .06) and increasing office chaos (P = .15) between baseline and 30 months.
In interviews, practice leaders described developing greater ability to provide high-quality care and adopting longitudinal, team-based approaches to serving chronically ill patients. Additional workload, implementation hurdles, underdeveloped technology, and change fatigue were noted as potential detractors from job satisfaction, however.
Job Satisfaction
Averaged across clinician and staff categories, job satisfaction had increased at 30 months in the Rhode Island pilot project (P = .03) but not in the Colorado pilot project. Combining both projects, there was nonsignificant improvement in job satisfaction among primary care physicians and nonclinical staff, and a nonsignificant trend toward worsening job satisfaction among nurse practitioners and physician assistants.
In interviews, practice leaders rated job satisfaction from very positive to neutral. They identified an increased ability for primary care physicians to concentrate on practicing medicine as a key contributor to job satisfaction. Leaders also reported greater staff satisfaction, which they attributed to empowerment. The changes in responsibilities related to the transformation were also challenging, however. For example, not all medical assistants coped well with adding new tasks and responsibilities to their existing duties, resulting in the departure of some staff.
Stress, Burnout, and Intention to Leave
At 30 months, about one-half of the respondents perceived their jobs to be moderately stressful, while about one-quarter reported highly stressful jobs, high levels of burnout, and a moderate or greater likelihood of leaving their practices within 2 years, as shown in Table 4.
Respondent Stress, Burnout, and Intention to Leave in Practices at 30 Months
Associations of Practice Environment With Clinician and Staff Outcomes
Table 5 shows the multivariate cross-sectional associations between dimensions of the practice environment and job satisfaction, stress, burnout, and intention to leave at 30 months. More open communication between clinicians and staff was associated with greater satisfaction and less burnout; greater emphasis on electronic information was associated with more stress and burnout. A 1-point increase in electronic information emphasis was associated with a nearly 50% increase in the odds of experiencing stress and a 2-fold increase in the odds of experiencing burnout.
Associations of the Practice Environment With Clinician and Staff Outcomes at 30 Months
Office chaos had large, significant associations with poor work experiences. A 1-point increase in office chaos was associated with a more than a 3-fold increase in the odds of experiencing high levels of stress and burnout and a 60% increase in the odds of intending to leave the practice within 2 years. Difficulties in providing safe, high-quality care were associated with lower job satisfaction and greater stress, burnout, and intention to leave.
DISCUSSION
In our study of medical home pilot projects in Rhode Island and Colorado, we found inconsistent changes in job satisfaction. For the 2 pilot projects combined, there were no statistically significant changes in job satisfaction; however, there was significant improvement in job satisfaction in the Rhode Island project and a modest, nonsignificant decline in satisfaction in the Colorado project. What explains these different results? First, baseline levels of job satisfaction were higher in Colorado, leaving less room to improve. Second, our qualitative data suggest that Colorado’s transformation work was more intensive, which could have created a “worse before better” scenario, like that described in evaluations of the TransforMed National Demonstration Project.21
Our findings suggest that the theoretical benefits of medical homes for clinicians and staff professional satisfaction may have been opposed by the stresses of transformation. For example, practices exhibited increasing emphasis on quality and fewer problems in providing safe, high-quality patient care. Such changes would be expected to enhance satisfaction; however, other trends seen among the practices—notably, greater office chaos—may have prevented greater job satisfaction from taking hold. Moreover, strategies aimed at reducing stress, such as reduced panel sizes, longer patient visit times, and dedicated time for care coordination (which have been featured in some medical home interventions13) were not included in the interventions we studied. These and similar transformation components may be necessary to foster better clinician experiences on a short timeline.
In general, fee-for-service payment does not compensate primary care physicians for non–visit-based care or coordination of care.22 The incentives provided in the pilot projects we studied may have been insufficient to encourage physicians to reduce office visit volumes while redesigning their practice. Broader payment reform may be essential for enabling transformation without increasing office chaos.
Finally, baseline levels of stress, burnout, and intention to leave were slightly lower than those previously found by Linzer et al.7 The practices we studied volunteered for early medical home pilot projects and so may have been better off at baseline than other practices, leaving relatively little room for improvement.
Our cross-sectional results suggest how medical home interventions can increase their chances of improving job satisfaction in primary care. Interventions that reduce difficulties in providing safe, high-quality care without increasing office chaos may offer the best chance of improving job satisfaction. The associations we observed between a quality emphasis, fewer quality problems, and job satisfaction corroborate research showing associations between greater engagement in quality-improvement activities, higher physician satisfaction, and less work-life stress.9 Similar to Hall et al,23 we found that a culture of open communication was associated with greater job satisfaction and less burnout. As suggested by other studies,7 our cross-sectional analysis found that greater office chaos was a key driver of dissatisfaction. Finally, we found associations between greater emphasis on electronic communication and increased stress and burnout, similar to findings of other recent studies.4,24
Our study has limitations. First, our sample size was small, limiting the power to detect longitudinal effects of project participation. Second, the observational nature of both our longitudinal and cross-sectional analyses limits causal inference. Third, no control practices were surveyed or interviewed about job satisfaction, so we cannot exclude the possibility that our longitudinal results are attributable to changes in primary care practice other than a medical home intervention. Fourth, practices in our study volunteered to be pilot project sites, and our findings may not generalize to later adopters of new practice models. Fifth, the 2 pilot projects we studied were administered by different entities and had multiple different intervention components, limiting our ability to compare the interventions directly on any single component. Sixth, we measured global job satisfaction only, limiting our ability to make inferences about subdimensions of job satisfaction. Finally, we interviewed only practice leaders, and this sampling may have yielded an incomplete or skewed perception of advances in the practice environment (ie, a rosier picture than front-line clinicians would paint).
Improving job satisfaction in primary care practices is an important goal of medical home interventions. Our findings suggest that medical home transformations that emphasize quality and open communication while minimizing office chaos may offer the best chances of improving job satisfaction.
Acknowledgments
The authors gratefully acknowledge the individuals who participated in this research. We would also like to acknowledge the invaluable assistance of Dr Mark Linzer and Dr Roger Brown in constructing subscales from the Minimizing Errors/Maximizing Outcomes clinician survey instruments, Dr E. John Orav for his statistical guidance, and Ms Diana Eastman for administering the surveys and transcribing the interviews.
Footnotes
-
Conflicts of interest: Dr Friedberg has received compensation from the US Department of Veterans Affairs for consultation related to the medical home model and research support from the Patient-Centered Outcomes Research Institute via subcontract to the National Committee for Quality Assurance.
-
Funding support: Shehnaz Alidina’s effort on this project was supported by dissertation grants from the Canada Program of the Weather-head Center for International Affairs and from the Canadian Federation of University Women. Funding for the study as a whole and for the effort of Meredith Rosenthal, Eric Schneider, Sara Singer, and Mark Friedberg was provided by the Commonwealth Fund.
-
Supplementary materials: Available at http://www.AnnFamMed.org/content/12/4/331/suppl/DC1/
- Received for publication October 25, 2013.
- Revision received March 25, 2014.
- Accepted for publication April 1, 2014.
- © 2014 Annals of Family Medicine, Inc.
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Improving surgical quality in low-income and middle-income countries: why do some health facilities perform better than others?
- Effect of interventions for the well-being, satisfaction and flourishing of general practitioners--a systematic review
- Indicators of Workplace Burnout Among Physicians, Advanced Practice Clinicians, and Staff in Small to Medium-Sized Primary Care Practices
- In This Issue: Technical and Personal Systems, and Novel Risk Factors