
Article Figures & Data
Figures
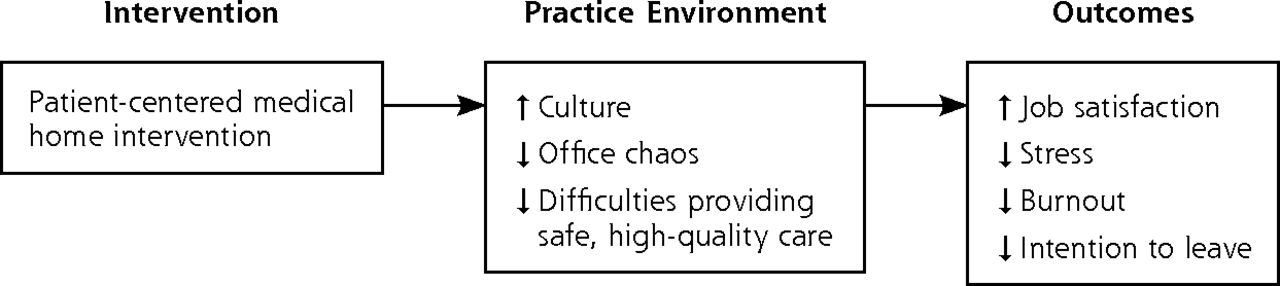
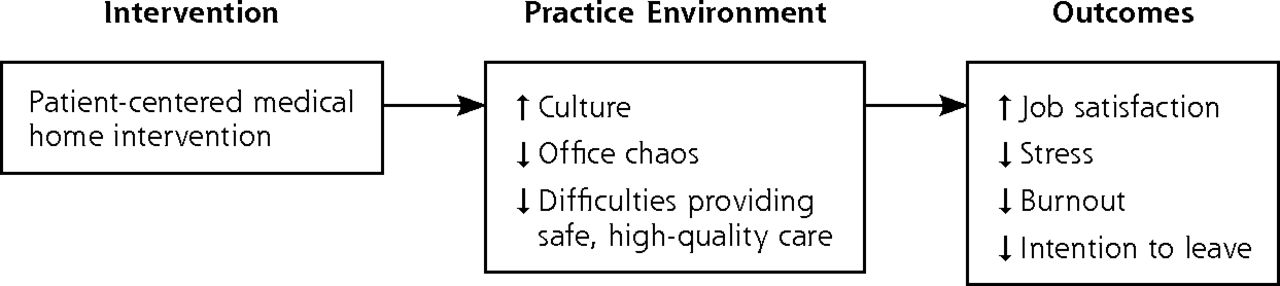
- Figure 1
Conceptual framework.
Tables
Characteristic Practices (N=20) No. (%) Practices Pilot project Rhode Island 5 (25) Colorado 15 (75) Type Private, stand-alone practice 17 (85) Federally qualified health center 1 (5) System-owned practice 2 (10) Affiliated with an IPA 10 (50) Practice size Solo practice 4 (20) 2–3 physicians 8 (40) 4–8 physicians 8 (40) NCQA PCMH recognition level Level 1 3 (15) Level 2 3 (15) Level 3 14 (70) Specialty Family medicine 16 (80) Internal medicine 4 (20) Survey respondents Baseline, No. (%) 30 Mo, No. (%) Total respondents 101 (61) 251 (80) Respondent type Physicians 56 (55) 80 (32) Physician assistants and nurse practitioners 16 (16) 22 (9) Nonclinical office staff 29 (29) 149 (59) Sex, female 61 (60) 208 (83) Average length of employment ≤2 y 34 (34) 80 (32) >2 y 66 (66) 171 (68) -
IPA = independent practice association; NCQA = National Committee for Quality Assurance; PCMH = patient-centered medical home.
-
- Table 2
Changes in the Practice Environment and Job Satisfaction at Baseline and 30 Months
Variable Baseline % 30 Months % P Value Organizational culture (“to a great extent”)a Quality emphasisb 24 35 .06 Electronic information emphasisb 64 63 .90 Open communicationb 51 44 .24 Hectic or chaotic office levelc 34 42 .15 Difficulties in providing safe, high-quality care (“sometimes”/ “frequently”)b,d 30 14 .001 Job satisfaction (“agree”/“strongly agree”)e By pilot project, respondents overall Rhode Island 67 86 .03 Colorado 86 80 .42 By respondent type, pilot projects combined Physicians 71 78 .49 Nurse practitioners and physician assistants 90 76 .41 Nonclinical office staff 76 84 .32 -
MEMO = Minimizing Error, Maximizing Outcomes.
-
↵a Compared with “not at all”/“a little”/“to a considerable extent.”
-
↵b Dichotomized based on median responses.
-
↵c Dichotomized based on <4 and ≥4 based on MEMO approach.
-
↵d Compared with “never”/“rarely.”
-
↵e Compared with “strongly disagree”/“disagree”/“neither agree nor disagree.”
-
Benefits Challenges Culture of quality
“I’m a good doctor, I work very hard. I keep up with the literature. I didn’t think measurement would make a difference. It was a striking and difficult experience when I realized I wasn’t doing as good a job as I thought, as measured…If you assume you are doing a good job, you are leaving the door wide open for not doing a good job. If you measure and improve at whatever level you start…that’s the part that’s far more inspiring.”
“Value depends on quality improvement. This is one of the most motivating pieces in becoming a PCMH. Power of measurement, data collection from one’s own practice, compared to benchmarks to see areas of competence, areas of improvement, areas of weakness—to guide improvement.”
Increased ability to provide safe, high-quality care
“The non-PCMH is episodic. The patient comes in to do something and the patient leaves…If they don’t come back, then they just stay gone. What we’re doing now…they’re not gone in between visits. Their orders are being tracked. If their results don’t come in, we notice. There are team members who are interacting with them in between visits, so they get a follow-up phone call. We’re also tracking outcomes…That is a very different model of care that feels a whole lot better.”
“The core is improved quality of care, more aggressive management of chronic disease, more aggressive preventive care—being that place where patients feel they can go and are cared about. Really trying to reduce those unnecessary complications of poorly managed chronic disease. In the past, when we had paper charts, we would just wait for patients to come and see us…Now with our EMR, with a click of a button we have a full registry of our diabetic patients and we are doing the same thing with other diseases as well. That’s the core of it.”
Meaningful work for physicians
“My colleagues would tell you that they are doing a lot more medicine and more patient care and less of the filling out forms, and more of taking care of people, which is why we went into medicine in the first place. So, on average I think it has been a very positive experience.”
“I can think of 2 physicians who told me that they would have retired from primary care if it were not for this project…[T]hey do feel like they are being better compensated…spending more of their time doing doctoring and less of their time doing things that they don’t consider to be at the top of their training.”
Meaningful work for staff/staff empowerment
“The people who work our registries see the fruits of their labor…one [patient] in particular was reminded about getting a mammogram and proved to have cancer 3 months after the test was ordered. That particular MA understands that this new type of work for her probably helped save a patient’s life. That is powerful stuff.”
“The dramatic difference in our practice was the engagement of our staff to be independent thinkers in patient care. Every staff member feels a part of the patient’s care, feels responsible…When a medical assistant sees an abnormal lab, he or she brings it to the doc’s attention instead of just assuming the doc will notice it.”Challenges in implementing electronic information systems
“We’ve had to jerry-rig our own ways of getting this stuff out and reported. On my really bad days when I am frustrated, I worry that our data might not be that accurate because of all that jerry-rigging. We at least have gone out of our way to really double- and triple-check stuff manually to make sure that we have the right data reported and data entered.”
“The challenges of our EMR should not be underestimated. My staff has come along with it, but it has just been a frustrating challenge to keep that system working right…I think there is some burnout there [among the staff]; there is for me too. It’s just been a challenging system at times.”
Increased workloads
“To transfer from a paper-based practice to electronic is a huge under-taking…People who take that on are really brave souls. That transition is harder than you plan, takes longer and more man hours.”
“I thought we could just lay this out and start doing something new…And it really takes a lot of work and a lot of time…Even if someone has a really good idea of how to do it, you still have to make your changes on the local level, figure out how it’s going to work for you.”
Transformation in roles and responsibilities
“I see our physicians as being significantly stressed by practicing in this environment and to some extent they may have traded in some of the old frustrations for the change management frustrations of a moving target…With so much change, whose job is it and whose job is it today?”
“Now, all of a sudden, we’ve taken people who have just taken orders and made them responsible for patient care. They’re not used to that kind of responsibility and accountability. That takes some character and personality, and there’s a lot of stress that goes along with that.”
Change fatigue
“We haven’t had [change fatigue] in the past, but we are beginning to have it now as we are adding more disease registries. When we only had 1 disease registry, it was easy to keep it up to date. Now that we are trying to do 3 or more, it’s that much more additional work on all of the staff and they get a little frustrated.”
“I do get change fatigue. But, when you are the only physician champion, you can’t really afford to show it…It will be a lot easier for practices years from now who are starting up their PCMH. They are going to have a guidebook they can follow…But for us, making the change is definitely very trying.”
Lack of broader payment reform
“There is just more stuff to do on this really fast-moving hamster wheel. That’s our problem. We need to figure out a way to get paid and get a way to engage patients…When we can move to a system where we can do more, say, phone management, engage patients in other ways that don’t require the time intensity that we have now. I think that is going to be what will be helpful.”-
EMR = electronic medical record; MA = medical assistant; PCMH = patient-centered medical home.
-
Variable Respondents, % Job stressa Above neutral stress (≥3.5) 47.8 High stress (≥4) 27.5 Burnouta Definitely burning out (≥3) 22.6 Persistently or completely burned out (≥4) 8.9 Intention to leave clinic within 2 ya Moderate or greater likelihood of leaving practice leaving (≥3) 22.5 -
↵a Dichotomized using cut points from Linzer et al.7 Scales: stress, 1–5 (1 = less job stress, 5 = high job stress); burnout, 1–5 (1 = no symptoms of burnout, 5 = completely burned out); and intention to leave within 2 years, 1–5 (1=none, 5=definitely).
-
- Table 5
Associations of the Practice Environment With Clinician and Staff Outcomes at 30 Months
Satisfaction Stress Burnout Intention to Leave Practice environmenta Odds Ratio P Value Odds Ratio P Value Odds Ratio P Value Odds Ratio P Value Level of office chaos 0.56 .19 3.47 <.001 3.67 <.001 1.62 .02 Organizational culture Quality emphasis 0.92 .35 1.07 .44 0.92 .22 0.89 .33 Electronic information emphasis 0.83 .30 1.48 <.001 1.91 .03 1.08 .74 Open communication 2.30 .002 0.67 .13 0.46 .03 0.75 .73 Difficulties in providing safe, high-quality care 0.58 <.001 1.37 .009 1.65 .03 1.85 <.0001 -
Note: Analyses controlled for sex, length of employment, and pilot project.
-
↵a As shown in Table 2.
-
Supplemental Appendixes 1-4
Supplemental Appendix 1: Design Elements of the Rhode Island and Colorado PCMH Pilots; Supplemental Appendix 2. Key Elements of Rhode Island PCMH Pilot Activities; Supplemental Appendix 3: Survey of Practice Environment and Satisfaction in PCMH Pilots; Supplemental Appendix 4: Interviews With PCMH Practice Leaders at Baseline, 18 Months and 30 Months
Files in this Data Supplement:
- Supplemental data: Appendixes 1-4 - PDF version
In Brief
Practice Environments and Job Satisfaction in Patient-Centered Medical Homes
Shehnaz Alidina , and colleagues
Background The medical home is a patient-centered, team-based model for organizing and delivering primary care. This study evaluates how transforming primary care practices to medical homes affects job satisfaction for clinicians and staff.
What This Study Found 20 primary care practices participating in medical home projects in Rhode Island and Colorado had only inconsistent changes in job satisfaction in the 30 months after the changes were implemented. Job satisfaction improved in Rhode Island but not in Colorado. For both projects, difficulties in providing safe, high-quality care decreased during the study period, but emphasis on quality and the level of chaos did not change significantly. Fewer difficulties in providing safe, high-quality care and more open communication were associated with greater job satisfaction; in contrast, greater office chaos and an emphasis on electronic information were associated with greater stress and burnout.
Implications
- The authors suggest that, in light of the modest and variable impact of medical home intervention on clinician satisfaction, benefits of intervention may be opposed by the stresses of transformation.
- Interventions that reduce difficulties in providing safe, high-quality care without increasing office chaos may offer the best chance of improving job satisfaction.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Improving surgical quality in low-income and middle-income countries: why do some health facilities perform better than others?
- Effect of interventions for the well-being, satisfaction and flourishing of general practitioners--a systematic review
- Indicators of Workplace Burnout Among Physicians, Advanced Practice Clinicians, and Staff in Small to Medium-Sized Primary Care Practices
- In This Issue: Technical and Personal Systems, and Novel Risk Factors