
Abstract
PURPOSE The Affordable Care Act of 2010 supports marked expansions in Medicaid coverage in the United States. As of January 1, 2014, a total of 25 states and the District of Columbia expanded their Medicaid programs. We tested the hypothesis that rates of uninsured safety net clinic visits would significantly decrease in states that implemented Medicaid expansion, compared with states that did not.
METHODS We undertook a longitudinal observational study of coverage status for adult visits in community health centers, from 12 months before Medicaid expansion (January 1, 2013 to December 31, 2013) through 6 months after expansion (January 1, 2014 to June 30, 2014). We analyzed data from 156 clinics in the OCHIN practice-based research network, with a shared electronic health record, located in 9 states (5 expanded Medicaid coverage and 4 did not).
RESULTS Analyses were based on 333,655 nonpregnant adult patients and their 1,276,298 in-person billed encounters. Overall, clinics in the expansion states had a 40% decrease in the rate of uninsured visits in the postexpansion period and a 36% increase in the rate of Medicaid-covered visits. In contrast, clinics in the nonexpansion states had a significant 16% decline in the rate of uninsured visits but no change in the rate of Medicaid-covered visits.
CONCLUSIONS There was a substantial decrease in uninsured community health center visits and a significant increase in Medicaid-covered visits in study clinics in states that expanded Medicaid in 2014, whereas study clinics in states opting out of the expansion continued to have a high rate of uninsured visits. These findings suggest that Affordable Care Act–related Medicaid expansions have successfully decreased the number of uninsured safety net patients in the United States.
INTRODUCTION
Health insurance facilitates access to care and reduces unmet health care needs,1–4 yet 47 million Americans did not have coverage in 2012.5 The Patient Protection and Affordable Care Act of 2010 (ACA), the largest health care–related legislation in the United States since Medicare’s establishment in 1966, was enacted with the goal of expanding coverage to all citizens and legal residents.6 The ACA calls for expansions in Medicaid coverage to individuals making up to 138% of the federal poverty level (FPL). In 2012, the Supreme Court ruled that states were not legally required to implement the ACA-sponsored Medicaid expansions, and those opting out could not be penalized.7 As of January 1, 2014, a total of 25 states and the District of Columbia had expanded their Medicaid programs.8
Estimates from previous studies suggested that 13 to 22 million individuals would gain Medicaid coverage after ACA implementation,9–11 and some actual results are now known.12,13 By June 2014, 7.2 million people were newly enrolled in Medicaid programs through the ACA,13 and since late 2013, the number of Americans without health insurance dropped by approximately 8.0 million.12 Many persons directly affected by these expansions are seen at community health centers (CHCs), which comprise much of our nation’s health care safety net, and serve a rapidly increasing number of patients regardless of their ability to pay14; in 2012, 36% of CHC patients were uninsured.15 Little is known, however, about the effects of the ACA expansions on the rate of uninsured safety net visits in states that did vs did not implement the Medicaid expansion.
This study compared rates of CHC visits by coverage status in the first 6 months after the ACA’s Medicaid expansions began, with those in the year before expansion. We tested the hypothesis that expansion will significantly decrease rates of uninsured CHC visits, and that rates of visits covered by insurance, particularly Medicaid, will increase significantly in CHCs in states that implemented Medicaid expansion, compared with states that did not.
METHODS
Data Source and Study Population
We used electronic health record data from the Oregon Community Health Information Network, renamed OCHIN as other states joined, a multi-state collaboration of health systems.16,17 This unique national organization facilitates implementation of electronic health records in CHCs and supports a practice-based research network. All OCHIN member clinics share a centrally hosted, linked instance of the EpicCare electronic health record (EPIC Systems). Almost all OCHIN clinic patients are from households below 200% of the FPL.16–18 We included a convenience sample of any CHCs having active status on OCHIN’s electronic health record as of January 1, 2013, totaling 167 CHCs in 11 states. We excluded CHCs from Texas because the majority of our eligible patient population was covered by a state-funded program similar to Medicaid in the preexpansion and postexpansion periods. We also excluded clinics in Wisconsin because their previously closed Medicaid program was opened to new applicants in 2014, so that state resembled an expansion state despite its nonexpansion status. After these exclusions, we had 156 CHCs located in 5 Medicaid expansion states (California, Minnesota, Ohio, Oregon, and Washington) and 4 nonexpansion states (Alaska, Indiana, Montana, and North Carolina). We included all face-to-face primary care visits by nonpregnant adults aged 19 to 64 years in the study period. Encounters were collected from 12 months before expansion (January 1, 2013 to December 31, 2013) through 6 months after expansion (January 1, 2014 to June 30, 2014) resulting in a total sample size of 333,655 patients with 1,276,298 encounters.
Variables
Our outcomes were rates of uninsured, Medicaid-insured, and commercially insured CHC visits in the preexpansion vs postexpansion periods overall, and by month across the 18-month study period. The primary independent variable was expansion status: whether or not a state expanded Medicaid eligibility to at least 138% of the FPL as of January 1, 2014.
Data Analysis
We computed χ2 statistics to compare patient panel characteristics between the study CHCs in expansion vs nonexpansion states. We conducted a 2-group longitudinal preexpansion vs postexpansion analysis where we compared visit rates in each period by expansion status. For greater detail about changes in visit rates, we did a preexpansion vs postexpansion analysis for each state. Generalized estimating equation Poisson models with compound symmetry correlation structure and empirical sandwich variance estimator were fitted to obtain rates and rate ratios (RRs) for the pre-expansion and postexpansion periods with 95% CIs, accounting for temporal correlation within CHCs, and adjusting for significant CHC and state-level covariates. We fitted similar regression models to obtain visit rates by month across the study period.
To account for differences in the composition of the CHCs’ patient panels, we adjusted for clinic-level frequencies of sex, age, race, ethnicity, urban vs rural residence, and household income. When comparing expansion vs nonexpansion status, we also assessed potential state-level economic covariates: 2014 minimum wage19 and unemployment rates,20 and the 2013 rate of uninsured adults.21 Significant covariates (P <.05) from an initial multivariable model were retained in final models. All statistical analyses were done using SAS version 9.3 (SAS Institute, Inc). This study was reviewed and approved by the Oregon Health & Science University Institutional Review Board.
RESULTS
At the start of the study period, CHCs in states that expanded Medicaid eligibility had younger patients, more patients under 138% of the FPL, fewer nonwhite patients, more Hispanic patients, and more patients in urban areas (P <.001 for all, Table 1). The overall encounter rate in the postexpansion period increased by 5% compared with the rate in the prior year in expansion state CHCs (RR = 1.05; 95% CI, 1.01–1.08; P = .01); the encounter rate remained unchanged across CHCs in nonexpansion states (RR = 0.95; 95% CI, 0.87–1.04; P = .25).
Characteristics of States, CHCs, and Encounter Rates Before and After Medicaid Expansion
The rate of Medicaid-covered visits increased sig nificantly in expansion state CHCs (RR = 1.36; 95% CI, 1.24–1.49; P <.001), while remaining unchanged across CHCs in nonexpansion states (RR = 1.05; 95% CI, 0.94–1.18; P = .35). The uninsured visit rate was 40% lower in the postexpansion period among expansion state CHCs (RR = 0.60; 95% CI, 0.54–0.67; P <.001); this rate also dropped in nonexpansion states CHCs, but to a lesser degree (RR = 0.84; 95% CI, 0.74–0.95; P = .01).
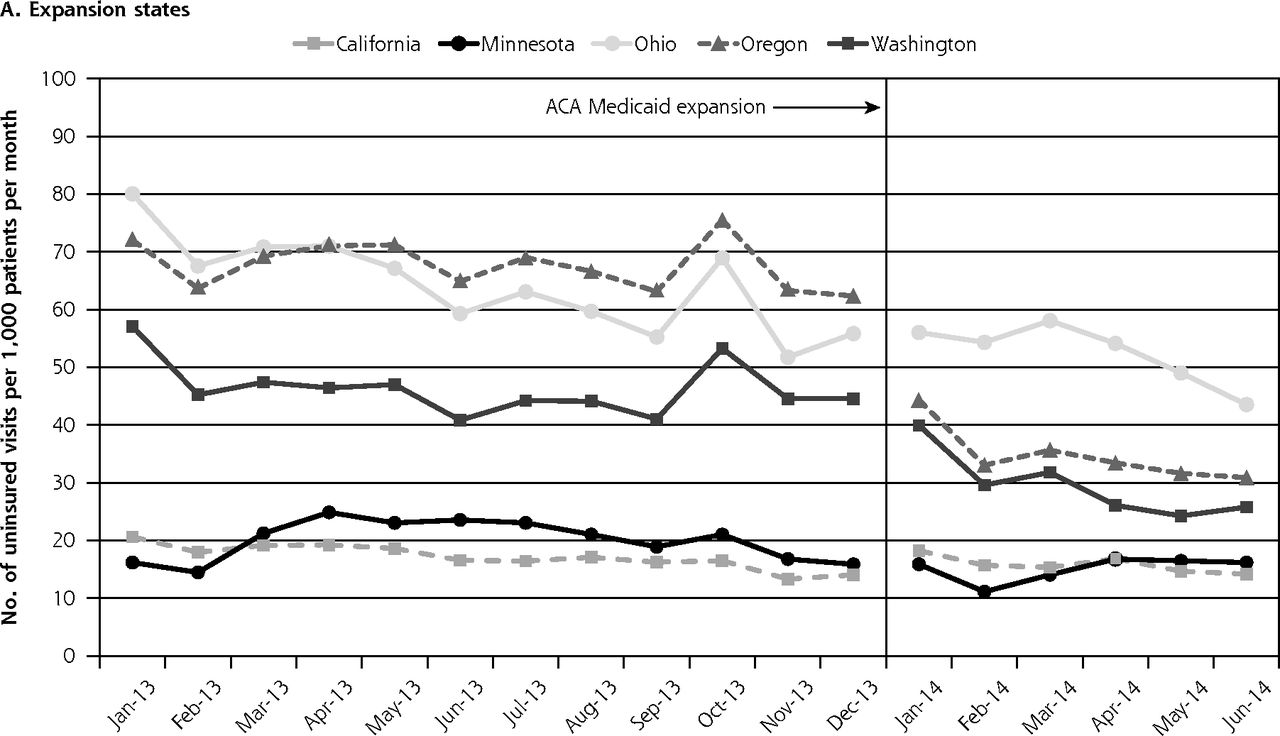
The results of our temporal analyses show a decline in postexpansion uninsured visit rates over time in the study CHCs in several expansion states, most notably Oregon, Washington, and Ohio (Figure 1). CHCs in California and Minnesota had low rates of uninsured visits throughout the study. Uninsured visit rates in nonexpansion state CHCs showed a less consistent pattern: declines in Montana, Indiana, and Alaska CHCs were not seen until March 2014, and uninsured rates remained steady in North Carolina CHCs.


Adjusted rates of uninsured visits by month among CHCs in expansion and nonexpansion states.
ACA = Affordable Care Act; CHC = community health center.
Notes: Rates calculated per 1,000 adult patients across entire study period. Poisson general estimating equation (GEE) model adjusted for percent of patients aged younger than 40 years and percent Hispanic, accounting for temporal correlation within CHCs over time.
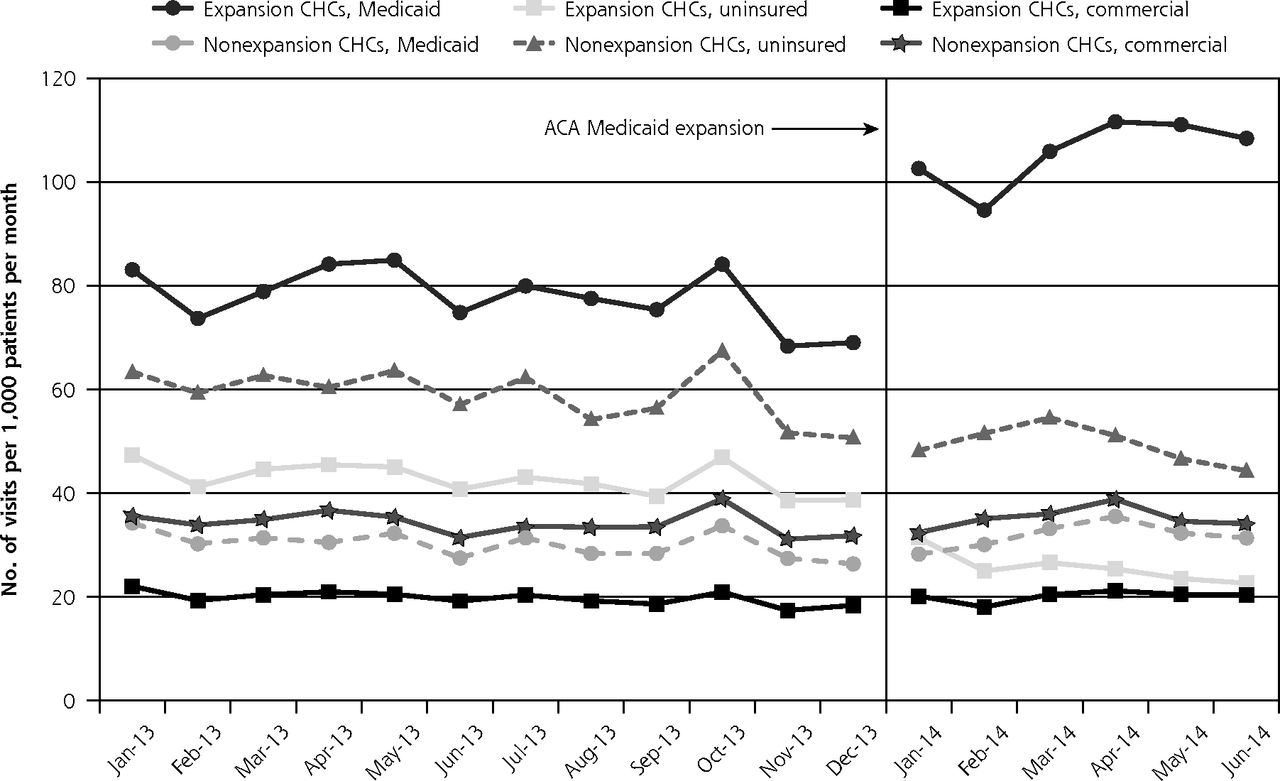
Figure 2 presents monthly visit coverage rates for CHCs by expansion status. In the first month postexpansion, the rate of Medicaid-covered visits increased 32% in expansion state CHCs, with an average increase of 71 encounters per CHC per month. In the same states, the rate of uninsured visits declined throughout the postexpansion period. Among CHCs in states that did not expand Medicaid, a modest increase in commercially insured visit rates was seen in the postexpansion period, but the difference between the preexpansion vs postexpansion periods was not statistically significant (P = .44).
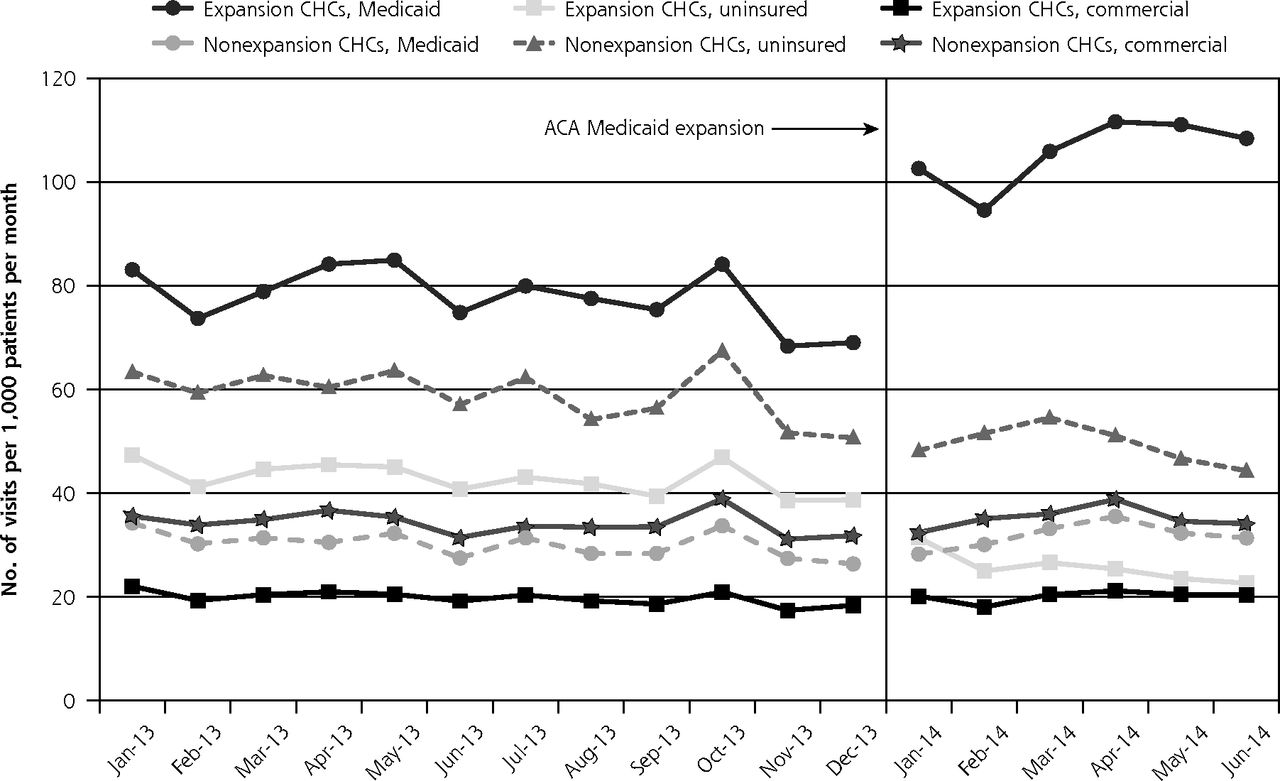
Adjusted visit rates by coverage status and month among CHCs in expansion and nonexpansion states.
ACA = Affordable Care Act; CHC = community health center.
Notes: Rates calculated per 1,000 adult patients across entire study period. Poisson general estimating equation (GEE) model adjusted for percent nonwhite race, percent Hispanic, percent ≤138% federal poverty level (FPL), and percent with unknown FPL; models account for temporal correlation within CHCs over time.
DISCUSSION
Main Findings
This study, the first to use electronic health record data to measure changes in CHC encounter coverage rates after ACA Medicaid expansions, found a 40% decrease in the rate of uninsured CHC visits in study Medicaid expansion states in 2014. Our findings confirm other reports showing increased health insurance coverage rates subsequent to state Medicaid expansion12,24,25 and add new information demonstrating a measurable effect on CHC visits in expansion states.
Although millions will gain Medicaid coverage after ACA implementation,9,10 it is also estimated that as many as 42% of adults who have not had insurance will continue to be without coverage options in states that have decided not to expand Medicaid,26,27 and that income-based inequalities will persist.28 CHCs will therefore likely continue to play a vital role in providing health care to vulnerable populations after the ACA, especially for adults in nonexpansion states who earn too much to qualify for Medicaid, but too little to afford private coverage.29 This population, estimated at nearly 5 million adults, has very limited coverage options and faces barriers to health care access.27 If every state participated in Medicaid expansions, such disparities in health care coverage and access could be mitigated.30 Additionally, the benefit of eliminating these disparities could reach beyond individual adult patients, affecting children and others in the household.29,31,32
Uninsured visits among study CHCs in California showed little change during the study period, which could be due to the backlog of Medicaid applications after expansion.33 The modest decline in uninsured visit rates in nonexpansion states could be attributable to increased coverage options available through the ACA’s insurance marketplaces, although we did not see an increase in commercially insured patients in nonexpansion states. Another explanation is that the capacity for seeing uninsured patients decreased in these states; more research is needed to better understand these findings.
Limitations
This study was based on a convenience sample of primary care CHCs with a linked electronic health record. These CHCs are located in 9 states, some of which are represented by only a few CHCs; thus, our results are not necessarily representative of the post-ACA experiences of all states, all CHCs in the study states, or expansion status groups. Our visit-based analysis evaluates the impact of Medicaid expansion on safety net clinics, but does not capture changes in individuals’ insurance status or patient panel characteristics. There were significant differences between expansion and nonexpansion states’ CHC patients in our sample, which we attempted to account for through adjusted multivariate analysis and by using expansion states as their own control in preexpansion vs postexpansion period comparisons. We recognize, however, that unobserved confounders could potentially influence these results.
Conclusion
We found a significant decrease in uninsured CHC visits and a significant increase in Medicaid-covered visits in study clinics in states that expanded Medicaid in 2014, whereas study CHCs in states opting out of the expansion maintained a high rate of uninsured visits. These findings suggest that ACA-related Medicaid expansions have been successful in decreasing the number of uninsured safety net patients in the United States.
Acknowledgments
We thank the OCHIN practice-based research network and the clinics for assisting with this research.
Footnotes
-
Conflicts of interest: authors report none.
-
Funding support: This work was financially supported by the Patient-Centered Outcomes Research Institute (PCORI), the National Cancer Institute (NCI) of the National Institutes of Health, grant 1 R01 CA181452 01, and the Oregon Health & Science University Department of Family Medicine.
-
Disclaimer: The funding agencies had no involvement in the design and conduct of the study; analysis and interpretation of the data; and preparation, review, or approval of the manuscript.
- Received for publication September 26, 2014.
- Revision received November 13, 2014.
- Accepted for publication November 19, 2014.
- © 2015 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Health Care Expenditures Among Adults With Diabetes After Oregons Medicaid Expansion
- Impact of Alternative Payment Methodology on Primary Care Visits and Scheduling
- Following Uninsured Patients Through Medicaid Expansion: Ambulatory Care Use and Diagnosed Conditions
- The Impact of the Affordable Care Act (ACA) Medicaid Expansion on Visit Rates for Diabetes in Safety Net Health Centers
- Implementation of Health Insurance Support Tools in Community Health Centers
- Uninsured Primary Care Visit Disparities Under the Affordable Care Act
- At Federally Funded Health Centers, Medicaid Expansion Was Associated With Improved Quality Of Care
- Medicaid Expansion And Grant Funding Increases Helped Improve Community Health Center Capacity
- After Medicaid Expansion In Kentucky, Use Of Hospital Emergency Departments For Dental Conditions Increased
- Community Health Center Use After Oregon's Randomized Medicaid Experiment
- In This Issue: Policy and Practice