
Article Figures & Data
Figures
- Figure 1
Standardized mean differences for posttreatment depression scores of psychological treatments compared with control (usual care or placebo).
CBT = cognitive behavioral therapy; SD = standard deviation; SMD = standard mean difference; IV = inverse variance.
aStudies included patients with major depression.
bStudies included patients with mixed/unclear depression.
cStudies included patients minor depression/dysthymia.
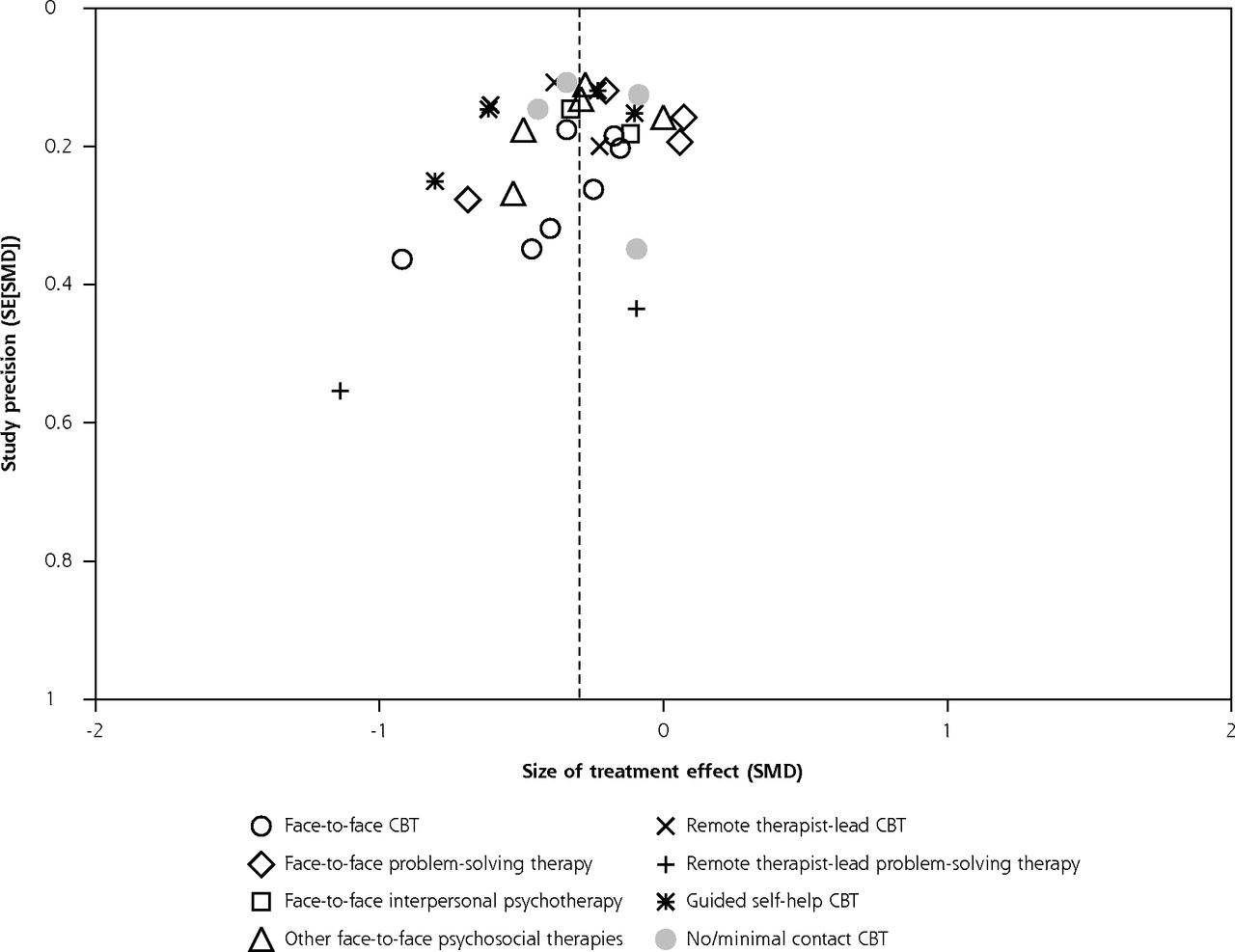
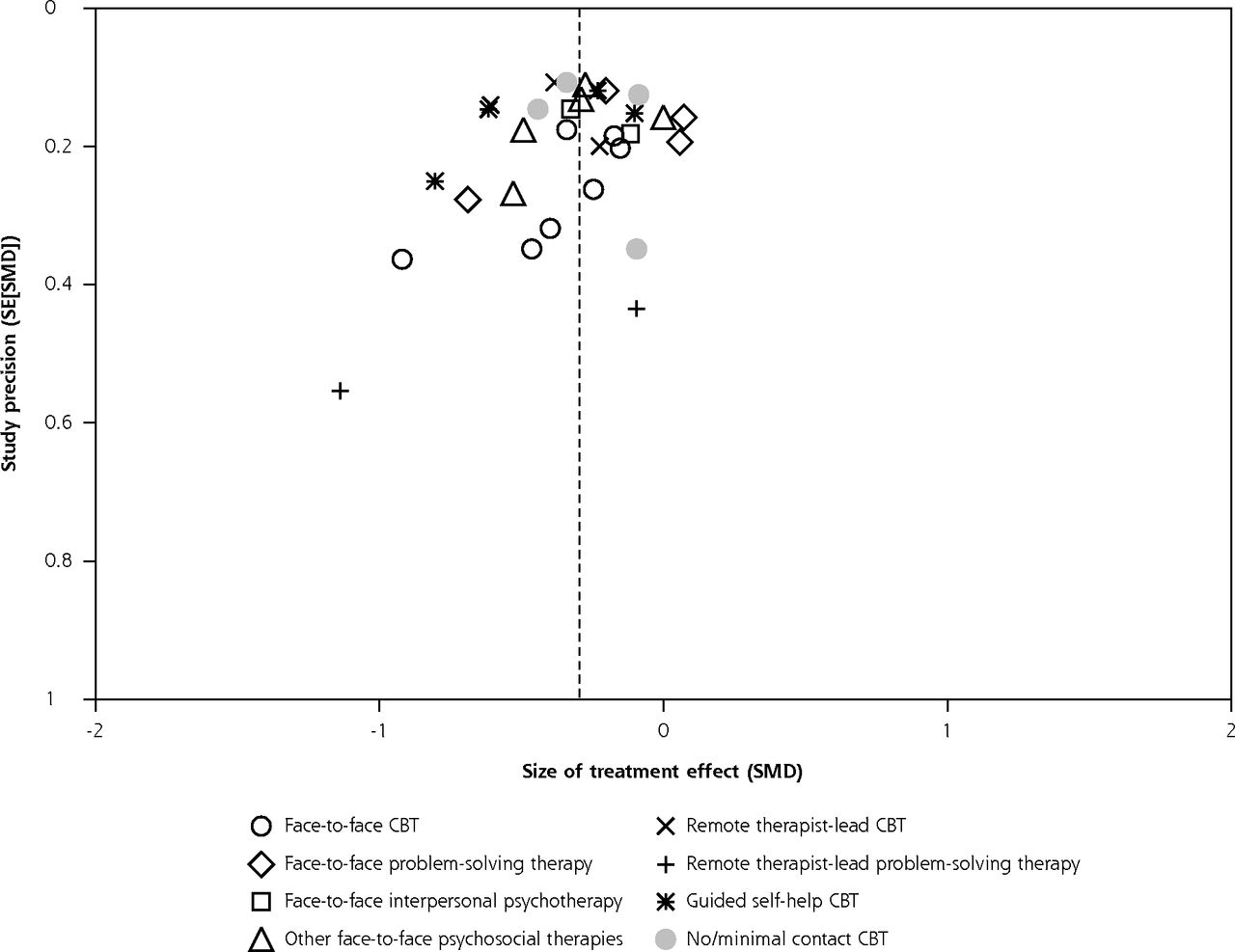
- Figure 2
Funnel plot plotting study precision against size of the treatment effect.
SE = standard error; SMD = standardized mean difference

Tables
First Author Risk of Bias No.a Recruitment Depression Diagnosis % Female Mean Age, y Group 1 (No. of Sessions; Clinician) Group 2 (No. of Sessions; Clinician) Further Groups Week Posttreatment Measurement Score and Instrument Response Remission Face-to-face CBT Laidlaw 2008 44 Referral Major depression 72 CBT Usual care 18 HRSD (i) u (luuul) 74 (8; psychologist) BDI HRSD (i) Scott 1997 48 Referral Major depression 67 Brief CT Usual care 7 HRSD (i) h (uuuhh) 41 (6; therapist) BDI HRSD (i) Serfaty 2009 137 Mainly screening Depression 79 CBT Usual care Talking controlb 16 BDI (i) l (llhul) 74 (≤12; therapist) BDI BDI (i) Smit 2006 116 Referral Major depression 64 CBT Usual care Recurrence preventionb 12 BDI (i) l (llhll) 43 (10–12; therapist) BDI BDI (i) Teasdale 1984 44 Screening Major depression 94 CT Usual care ca 16 HRSD h (uuhhl) 38 (≤20; psychologist) BDI (i) BDI Face-to-face problem-solving therapy Barrett 2001 161 Referral Dysthymia, minor depression 64 Problem solving Placebo Paroxetineb 11 nr u (luuuu) 44 (6; psychologist) HSCL-D (c, i) HRSD ≤6 Mynor-Wallis 1995 60 Referral Major depression 77 Problem solving Placebo Amitriptyline 12 HRSD (i) h (uuuhl) 37 (6; trained physician) BDI HRSD (i) Oxman 2008 141 Screening Minor depression 58 Problem solving Usual care 9 MADRS (i) u (llhuu) 55 (6; counselor) MADRS MADRS (i) Williams 2000 278 Referral or screening Dysthymia or minor depression 41 Problem solving Placebo Paroxetineb 11 HSCL-D (i) h (llhlh) 71 (6; psychologist/counselor) HSCL-D (c) HAD-D Face-to-face interpersonal psychotherapy Schulberg 1996 185 Screening Major depression 83 Interpersonal PT Usual care Nortriptylineb 26 HRSD (i) h (uuuhh) 38 (16; psychologist/psychiatrist) HRSD (i) HRSD (i) Van Schaik 2006 143 Screening Major depression 69 Interpersonal PT Usual care 26 MADRS u (ulhul) 68 (10; psychologist/nurse) MADRS MADRS Other face-to-face psychosocial therapies Casanas 2012 231 Referral Major depression 89 Psychoeducation Usual care 12 BDI (i) l (llhul) 53 (12; nursec) BDI BDI (i) Corney 1984 87 Referral Depression 100 Social work Usual care Unclear Improvement h (huhuh) 30 (Unclear; social worker) nr nr Corney 2005 181 Screening Depression 80 Counseling Usual care 26 BDI (i) l (luhll) (≥6 mo) 43 (6–12; counselorc) BDI BDI (i) MacPherson 2013 453 Referral Depression 73 Counseling Usual care Acupunctureb 12 PHQ-9 (i) l (llhul) 44 (12; counselors) PHQ-9 PHQ-9 (i) Three-armed trials with face-to-face CBT and other face-to-face psychosocial therapies Scott 1992 121 Referral Major depression 76 CBT Counseling HRSD (i) u (uuuul) 32 (10; psychologist) (13; social worker) Usual care 16 HRSD Ward 2000 197 Referral Depression 77 CBT Counseling Amitriptylineb HRSD BDI (i) l (ulhll) 37 (6–12; psychologist) (6–12; counselorc) Usual care 16 BDI (i) Remote therapist-led CBT Dwight-Johnson 2011 101 Screening Depression 78 Telephone CBT Usual care 12 HSCL-D l (llhul) 40 (8; trained therapist) HSCL-D nr Kessler 2009 297 Referral Major depression 68 Online CBT Usual care 16 BDI (i) h (llhhl) 35 (≤10; psychologist) BDI BDI (i) Simon 2004 393 Referral Depression 76 Telephone CBT Usual care 26 HSCL-D u (llhuu) 44 (8; psychotherapist) HSCL-D HSCL-D Remote therapist-led problem-solving therapy Lynch 1997 29 Screening Minor depression 86 Telephone problem solving Usual care, 6 nr h (uuhhu) 48 (6; trained student) no treatment BDI (i) BDI (i) Lynch 2004 54 Screening Mild depression 83 Telephone problem solving Usual care 6 nr h (uuhhh) 38 (6; nurse) BDI BDI (i) Guided self-help CBT Joling 2011 170 Screening Subthreshold depression 54 Bibliotherapy Usual care 12 CES-D reduction ≥5 u (luhul) 81 (3; nurse) CES-D CES-D ≤16 Proudfoot 2004 274 Referral or screening Depression 74 Computerized CBT Usual care 9 BDI (i) u (ulhuu) 44 (≤80 min; nursec) BDI BDI (i) Watkins 2012 82 Screening Depression 55 Guided self-help concreteness training Usual care 8 HRSD (i) l (llull) 46 (≤4; psychologist) Relaxation controlb BDI HRSD (i) Williams 2013 281 Referral Depression 68 Guided self-help CBT Usual care 16 BDI u (ulhul) 42 (3; psychologist) BDI BDI (i) No/minimal contact CBT de Graaf 2009 303 Screening Depression 57 Computerized CBTd Usual care l (llhll) 45 8 BDI reliable change Levesque 2011 350 Screening Depression 67 Computer behavioral intervention (TTM) Usual care, no intervention BDI BDI (i) h (luhhl) 47 39 BDI ≤9+ significant change Levin 2011 191 Referral Depression 77 Computer CBT Usual care BDI l (luhll) 44 BDI (i) Naylor 2010 38 Screening Depression 84 Bibliotherapy Usual care 6 SCID symptoms (i) h (luhhl) 51 CES-D nr 6 BDI-FS (i) BDI-FS BDI-FS (i) -
BDI = Beck Depression Inventory; BDI-FS = Beck Depression Inventory-Fast Screen; c = only change from baseline data available; ca = circa; CBT = cognitive behavioral therapy; CES-D = Center for Epidemiologic Studies-Depression Scale; CT = cognitive therapy; HAD-D = Hospital Anxiety and Depression Scale subscale depression; HRSD = Hamilton Rating Scale for Depression; HSCL-D = Hopkins Symptom Checklist Depression Scale; i = imputed data; MADRS = Montgomery Asberg Depression Rating Scale; nr = not measured or reported; PHQ-9 = Patient Health Questionnaire for Depression; PT = psychotherapy; RDC = Research Diagnostic Criteria; SCID = Structured Clinical Interview for DSM Disorders; TTM = transtheoretical model.
Note: Risk of bias: l = low, u = unclear, h = high. First letter indicates the overall risk of blinding, not taking blinding into account; letters in parentheses sequentially indicate the risk of bias for the following 5 items: sequence generation, concealment, blinding, attrition, and selective reporting, respectively.
-
↵a Number of patients randomized (only in groups included in analyses).
-
↵b Comparator or control group not included in analyses.
-
↵c Trial included 2 separate groups (computerized CBT alone and in combination with usual care), which were pooled.
-
↵d Person providing the treatment was explicitly or probably a routine member of the primary care team.
-
Therapy Response NNTa (95%-CI) Remission NNTb (95% CI) Study Discontinuation Face-to-face CBT 10 (5–47) na OR (95% CI) 1.58 (1.11 to 2.26) 1.49 (0.90 to 2.46) 0.98 (0.52 to 1.86) I2, % 0 35 25 No. of trials 7 7 6 Face-to-face problem-solving therapy na na OR (95% CI) 1.56 (0.85 to 2.86) 1.29 (0.83 to 2.02) 0.60 (0.23 to 1.57) I2, % 55 44 80 No. of trials 3 4 4 Face-to-face interpersonal psychotherapy na na OR (95% CI) 1.28 (0.80 to 2.05) 1.37 (0.81 to 2.34) 0.98 (0.40 to 2.38) I2, % 0 12 na No. of trials 2 2 1 Other face-to-face psychological therapies 11 (6–31) 10 (5–35) OR (95% CI) 1.54 (1.17 to 2.03) 1.68 (1.17 to 2.41) 1.04 (0.65 to 1.67) I2, % 0 0 37 No. of trials 6 5 5 Remote therapist-led CBT 6 (4–13) na OR (95% CI) 2.04 (1.44 to 2.90) 1.51 (0.98 to 2.32) 1.05 (0.29 to 3.75) I2, % 23 36 75 No. of trials 3 3 2 Remote therapist-led problem-solving therapy No data No data na OR (95% CI) 1.22 (0.23 to 6.57) 1.32 (0.33 to 5.26) I2, % 20 46 No. of trials 2 2 Guided self-help CBT 9 (5–24) 9 (5–28) OR (95% CI) 1.67 (1.22 to 2.28) 1.73 (1.21 to 2.50) 1.54 (1.00 to 2.37) I2, % 0 0 32 No. of trials 4 4 4 No/minimal contact CBT 11 (6–58) na OR (95% CI) 1.52 (1.09 to 2.13) 1.46 (0.96 to 2.23) 1.32 (0.88 to 2.00) I2, % 0 0 0 No. of trials 4 3 4 Test for subgroup differences χ2 3.32 5.80 4.44 P value .85 .67 .82 I2, % 0 0 0 All treatments 10 (8–14) 15 (10–25) OR (95% CI) 1.59 (1.40 to 1.80) 1.42 (1.24 to 1.62) 1.08 (0.85 to 1.38) I2, % 0 0 46 No. of trials 27 28 27 -
CBT = cognitive behavioral therapy; I2 = measure of statistical heterogeneity; na = not applicable; NNT = number needed to treat; OR = odds ratio.
Note: NNTs for study discontinuation cannot be calculated in a valid manner as the confidence intervals of all odds ratios include the value 1.
-
↵a Proportion of control group patients with response = 27%.
-
↵b Proportion of control group patients with remission = 23%.
-
Variable Posttreatment Scores SMD (95% CI) I2, % No. of Comparisons Diagnostic subgroups Major depression −0.38 (−0.50 to −0.25) 5 10 Mixed/unclear −0.31 (−0.41 to −0.21) 33 14 Minor depression and/or dysthymia −0.09 (−0.26 to 0.07) 18 6 Test for subgroup differences, P value = .03 Delivery mode Face-to-face −0.23 (−0.33 to −0.14) 17 18 Remote therapist-led −0.43 (−0.62 to −0.25) 20 5 Guided self-help and no/minimal contact −0.33 (−0.48 to −0.17) 53 8 Test for subgroup differences, P value = .14 Treatment concept CBT (all delivery modes) −0.34 (−0.44 to −0.25) 29 18 PST (all delivery modes) −0.19 (−0.45 to 0.07) 51 6 Interpersonal psychotherapy (face-to-face) −0.24 (−0.47 to −0.02) 0 2 Counseling intervention (face-to-face) −0.27 (−0.50 to −0.05) 39 4 Psychoeducation (face-to-face) −0.29 (−0.55 to −0.03) na 1 Test for subgroup differences, P value = .77 Recruitment Referral −0.31 (−0.41 to −0.22) 20 14 Screening −0.28 (−0.40 to −0.16) 44 17 Test for subgroup differences, P value = .68 Age-group Adults −0.31 (−0.41 to −0.23) 39 26 Only elderly −0.17 (−0.32 to −0.02) 0 5 Test for subgroup differences, P value = .08 Number of treatment sessions >6 −0.33 (−0.48 to −0.17) 53 8 6 to 9 −0.25 (−0.38 to −0.11) 35 13 ≥10 −0.32 (−0.44 to −0.21) 12 10 Test for subgroup differences, P value = .65 Risk of bias Low −0.27 (−0.38 to −0.15) 24 11 Unclear −0.24 (−0.39 to −0.09) 48 10 High −0.40 (−0.54 to −0.26 21 10 Test for subgroup difference, P value = .24 Sample size Up to median (≤152 patients) −0.33 (−0.47 to −0.19) 22 16 Above median −0.28 (−0.37 to −0.19) 46 15 Test for subgroup differences, P value = .58 -
CBT = cognitive behavioral therapy; na = not applicable; PST = problem-solving therapy; SMD = standardized mean difference.
-
Supplemental Appendix
Files in this Data Supplement:
- Supplemental data: Appendix - PDF file, 4 pages + cover
The Article in Brief
Effectiveness of Psychological Treatments for Depressive Disorders in Primary Care: Systematic Review and Meta-Analysis
Klaus Linde , and colleagues
Background Psychological interventions have a central role in treating depressive disorders. This analysis of currently available evidence looks at whether psychological treatments are effective for treating depressed primary care patients compared to usual care or placebo, taking type of therapy and its delivery method into account.
What This Study Found Overall, psychological treatments, including cognitive behavioral therapy (CBT), are superior to usual care alone, with small to moderate effect sizes. Differences between different types of psychological treatments are minor, with remote therapist-led, guided self-help and minimal-contact approaches appearing to produce effects similar to more intensive, personalized face-to-face therapies. However, the finding that remote, reduced or minimal contact CBT-based interventions seem to be similarly effective to intense face-to-face treatments should be interpreted carefully, in light of the limited number and moderate size of the identified studies.
Implications
- The authors conclude that these findings are reassuring for patients and clinicians wishing to pursue treatment options other than drugs.
- Although the available evidence for non-drug treatment of depression in primary care is promising, it is still not sufficient to guide practice and health policy. The authors call for large pragmatic trials comparing long-term outcomes and acceptability of different psychological treatment strategies in primary care patients with depression.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Strategies for Implementing Integrated Behavioral Health into Health Centers
- Implementing primary healthcare-based measurement, advice and treatment for heavy drinking and comorbid depression at the municipal level in three Latin American countries: final protocol for a quasiexperimental study (SCALA study)
- Implementation of e-mental health interventions for informal caregivers of adults with chronic diseases: a protocol for a mixed-methods systematic review with a qualitative comparative analysis
- Study protocol for a systematic review of evidence for digital interventions for comorbid excessive drinking and depression in community-dwelling populations
- Brief behaviour change strategies for distressed patients in primary care
- Mental health specialist video consultations for patients with depression or anxiety disorders in primary care: protocol for a randomised controlled feasibility trial
- Do psychosocial job stressors influence mental health service use? Evidence from an Australian cohort
- Depression in primary care: part 2--management
- Treating Subthreshold Depression in Primary Care: A Randomized Controlled Trial of Behavioral Activation With Mindfulness
- Comparative efficacy and acceptability of interventions for major depression in older persons: protocol for Bayesian network meta-analysis
- Incentives and disincentives for treating of depression and anxiety in Ontario Family Health Teams: protocol for a grounded theory study
- Approaches for synthesising complex mental health interventions in meta-analysis
- Psychological treatments are effective for depression in primary care, study shows
- In This Issue: Policy and Practice
- Treatment of Depression in Primary Care