
Article Figures & Data
Figures
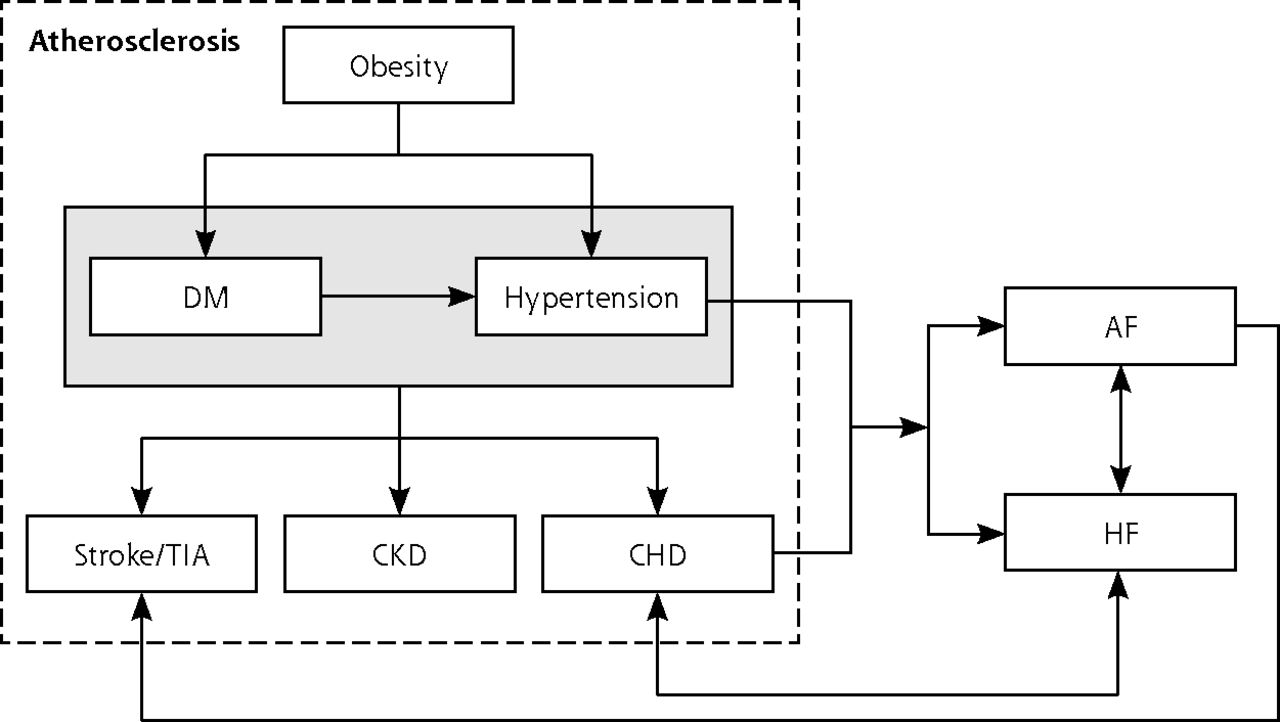
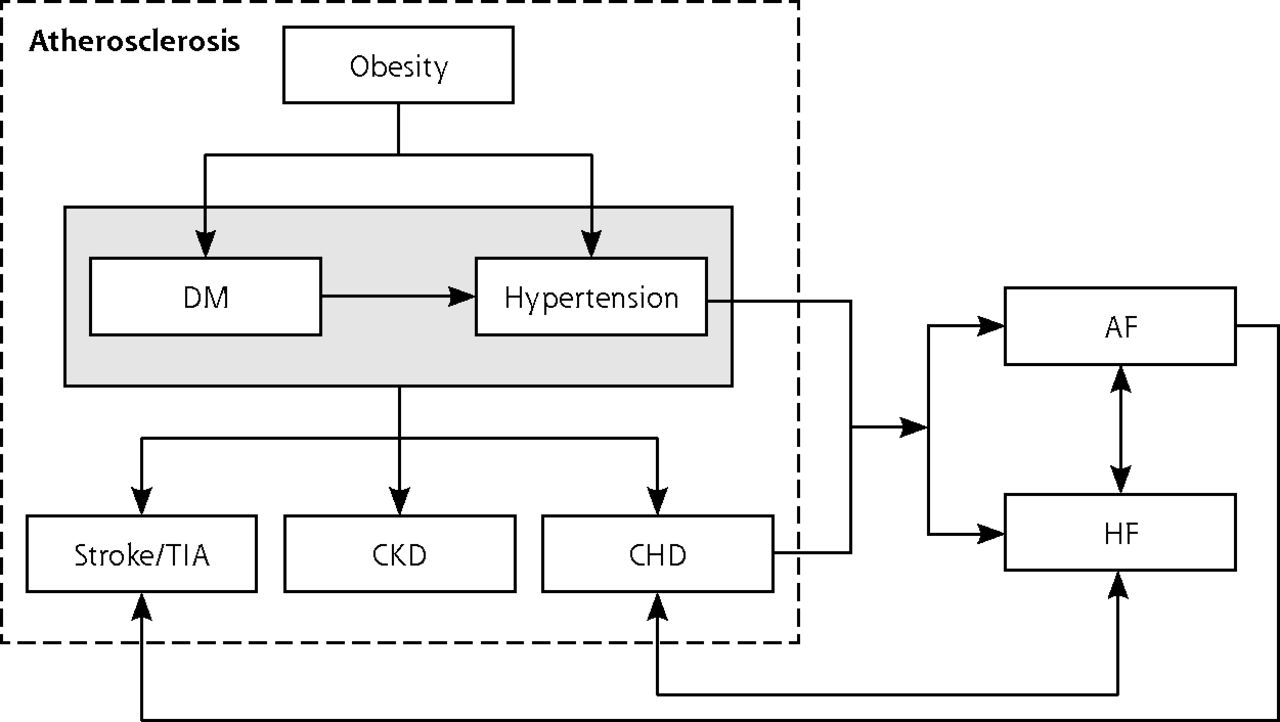
- Figure 1
Etiopathophysiologic relation between concordant conditions.
AF = atrial fibrillation; CHD = coronary heart disease; CKD = chronic kidney disease; DM = diabetes mellitus; HF = heart failure; TIA = transient ischemic attack.
Tables
Indicator Short Name Description (% Patients) Type of Indicator DM02 BMI record Whose notes record body mass index Process of care DM10 Neuropathy testing With a record of neuropathy testing Process of care DM13 Microalbuminuria record Who have a record of microalbuminuria testing (except reporting for patients with proteinuria) Process of care DM15 ACE inhibitor With a diagnosis of proteinuria or microalbuminuria who are treated with ACE inhibitors (or angiotensin II receptor blockers) Process of care DM18 Influenza immunization Who have had influenza immunization Process of care DM21 Retinal screening Who have a record of retinal screening Process of care DM22 Renal function record Who have a record of estimated glomerular filtration rate or serum creatinine testing Process of care DM29 Foot risk With a record of foot examination and risk classification: (1) low risk (normal sensation, palpable pulses), (2) increased risk (neuropathy or absent pulses), (3) high risk (neuropathy or absent pulses plus deformity or skin changes or previous ulcer), or (4) ulcerated foot Process of care DM17 Cholesterol ≤193.05 mg/dL (≤5 mmol/L) Whose last measured total cholesterol was 193.05 mg/dL (≤5 mmol/L) or lower Intermediate outcome DM26 Diabetes control (HbA1c = 7.5%) In whom the last IFCC-HbA1c reading was 59 mmol/mol (equivalent to HbA1c of 7.5% in DCCT-derived units) or lower Intermediate outcome DM31 BP ≤140/80 mm Hg In whom the last blood pressure reading was 140/80 mm Hg or lower Intermediate outcome ACE = angiotensin-converting enzyme; BMI = body mass index; BP = blood pressure; DCCT = Diabetes Control and Complications Trial; DM = diabetes mellitus; HbA1c = glycated hemoglobin; IFCC = International Federation of Clinical Chemistry.
Note: All indicators within the previous 15 months except for DM18 (immunization in the preceding September 1 to March 31).
Characteristic Mean (SD) Range Registered patients, No. 6,877 (4,001) 572–37,474 Female patients, % 50.16 (6.08) 8.64–75.85 Patient age ranges 18–24 y, % 9.82 (5.91) 0–91.65 25–34 y, % 17.50 (8.46) 0–71.15 35–44 y, % 18.02 (5.63) 0–45.09 45–54 y, % 18.47 (4.30) 0–42.38 55–64 y, % 14.76 (4.42) 0–32.54 65–74 y, % 11.70 (4.71) 0–30.00 75–84 y, % 6.98 (3.13) 0–22.21 ≥85 y 2.74 (1.65) 0–14.41 Ethnicity White, % 84.15 (21.72) 0–100 Asian, % 7.98 (14.00) 0–87.48 Black, % 3.28 (6.41) 0–59.07 Index of multiple deprivation score 21.78 18.54 Prevalence of diabetes, % 6.21 (1.77) 0.10–18.00 Prevalence of diabetes-concordant conditions Obesity, % 11.25 (3.83) 0–43.30 Hypertension, % 13.81 (3.67) 0–36.10 CHD, % 3.34 (1.17) 0–9.10 CKD, % 4.16 (2.08) 0–24.10 Stroke and TIA, % 1.66 (0.65) 0–6.50 Atrial fibrillation, % 1.45 (0.66) 0–5.10 Heart failure, % 0.71 (0.33) 0–3.90 Prevalence of diabetes-discordant conditions Asthma, % 5.95 (1.36) 0–13.70 Cancer, % 1.87 (0.74) 0–5.50 COPD, % 1.79 (0.89) 0–8.20 Dementia, % 0.55 (0.39) 0–9.60 Depression, % 5.78 (3.01) 0–35.90 Epilepsy, % 0.78 (0.28) 0–4.00 Hypothyroidism, % 3.17 (1.05) 0.10–8.50 Severe mental health disorders, % 0.87 (0.45) 0–11.80 CHD = coronary heart disease; CKD = chronic kidney disease; COPD = chronic obstructive pulmonary disease; TIA = transient ischemic attack.
- Table 3
Association Between Quality of Diabetes Care (Process) and the Prevalence of Diabetes and Diabetes-Concordant and Diabetes-Discordant Conditions
Condition <3,000 Patients (n = 1,376) % (95% CI) 3,000–6,000 Patients (n = 2,466) % (95% CI) 6,001–10,000 Patients (n = 2,354) % (95% CI) >10,000 Patients (n = 1,688) % (95% CI) All Practices (N = 7,884) % (95% CI) Diabetes −0.32
(−0.57 to −0.07)a−0.23
(−0.41 to −0.05)a−0.26
(−0.44 to −0.08)a−0.54
(−0.78 to −0.29)−0.31
(−0.41 to −0.21)aDiabetes concordant Obesity 0.37
(0.29 to 0.44)a0.31
(0.26 to 0.38)a0.35
(0.30 to 0.41)a0.27
(0.20 to 0.35)a0.33
(0.30 to 0.37)aHypertension −0.13
(−0.26 to −0.01)a−0.10
(−0.20 to 0.00)−0.11
(−0.20;−0.01)a0.09
(−0.03 to −0.21)a−0.08
(−0.13 to −0.02)aCHD −0.31
(−0.77 to 0.14)−0.54
(−0.92 to −0.20)a−0.09
(−0.43 to 0.24)−0.38
(−0.84 to 0.05)−0.38
(−0.58 to −0.20)aCKD 0.29
(0.14 to 0.45)a0.21
(0.10 to 0.33)a0.07
(−0.02 to 0.17)0.2 1
(0.09 to 0.32)a0.18
(0.12 to 0.24)aStroke and TIA 0.81
(0.05 to 1.50)a−0.30
(−0.97 to 0.32)0.35
(−0.26 to 0.91)0.2 8
(−0.53 to 1.03)0.28
(−0.05 to 0.60)Atrial fibrillation −0.38
(−1.29 to 0.45)0.87
(0.30 to 1.46)a1.25
(0.71 to 1.76)a0.6 2
(−0.13 to 1.31)0.57
(0.25 to 0.89)aHeart failure 0.89
(−0.10 to 1.78)0.59
(−0.13 to 1.30)0.40
(−0.31 to 1.06)0.4 4
(−0.51 to 1.29)0.60
(0.25 to 0.89)aDiabetes discordant Asthma 0.09
(−0.13 to 0.30)0.30
(0.15 to 0.46)a0.01
(−0.14 to 0.16)0.32
(0.13 to 0.51)a0.19
(0.10 to 0.27)aCancer 1.05
(0.49 to 1.59)a0.70
(0.29 to 1.13)a0.10
(−0.32 to 0.50)0.41
(−0.04 to 0.85)0.59
(0.37 to 0.81)aCOPD 0.29
(−0.14 to 0.70)0.26
(−0.06 to 0.59)0.06
(−0.28 to 0.38)0.19
(−0.26 to 0.62)0.23
(0.05 to 0.41)aDementia −0.11
(−0.83 to 0.56)0.28
(−0.24 to 0.78)−0.15
(−0.83 to 0.48)−0.62
(−1.52 to 0.21)0.01
(−0.30 to 0.31)Depression −0.02
(−0.12 to 0.08)−0.05
(−0.12 to 0.02)−0.03
(−0.09 to 0.03)0.01
(−0.06 to 0.09)−0.03
(−0.07 to 0.01)Epilepsy 0.12
(−0.90 to 1.05)−0.77
(−1.75 to 0.08)−1.07
(−2.07 to −0.15)a−1.65
(−3.06 to −0.39)a−0.80
(−1.30 to −0.33)aHypothyroidism 0.06
(−0.28 to 0.38)0.19
(−0.05 to 0.45)0.07
(−0.17 to 0.31)−0.06
(−0.35 to 0.22)0.08
(−0.05 to 0.22)Severe mental health disorder −0.85
(−1.42 to −0.31)a−1.16
(−1.82 to −0.62)a−0.42
(−0.99 to 0.12)−0.45
(−1.27 to 0.31)−0.76
(−1.04 to −0.49)aCHD = coronary heart disease; CKD = chronic kidney disease; COPD = chronic obstructive pulmonary disease; TIA = transient ischemic attack.
Note: Based on multivariate linear regression analysis. Dependent variable is the logit-transformed achievement rate of processes of care indicators. Independent variables are the prevalence of diabetes and conditions concordant and discordant to diabetes. Analysis adjusted for age, sex, ethnicity, deprivation, number of general practitioners, Carr-Hill list size, and exception rate. Coefficients have been back-transformed to percentages from logit-transformed achievement rates. β is the fully adjusted, absolute percentage change in achievement rate across the overall processes of care, per 1% change in prevalence.
↵a P <.05.
- Table 4
Association Between the Quality of Diabetes Care (Intermediate Outcomes) and the Prevalence of Diabetes and Diabetes-Concordant and Diabetes-Discordant Conditions
Condition <3,000 Patients (n = 1,376) % (95% CI) 3,000 to 6,000 Patients (n = 2,466) % (95% CI) 6,001 to 10,000 Patients (n = 2,354) % (95% CI) >10,000 Patients (n = 1,688) % (95% CI) All Practices (N = 7,884) % (95% CI) Diabetes 0.06
(−0.32 to −0.44)0.04
(−0.22 to 0.31)0.08
(−0.22 to 0.36)0.25
(−0.11 to 0.60)0.06
(−0.09 to 0.22)Diabetes concordant Obesity 0.27
(0.15 to 0.39)a0.27
(0.18 to 0.36)a0.28
(0.18 to 0.37)a0.08
(−0.04 to 0.20)0.24
(0.19 to 0.29)aHypertension −0.21
(−0.40 to −0.02)a−0.23
(−0.37 to −0.08)a−0.33
(−0.49 to −0.18)a−0.22
(−0.40 to −0.04)a−0.22
(−0.30 to −0.14)aCHD −0.28
(−0.97 to 0.40)−0.43
(−0.93 to 0.07)0.09
(−0.45 to 0.62)−0.20
(−0.86 to 0.45)−0.31
(−0.59 to −0.02)aCKD 0.36
(0.11 to 0.60)a0.30
(0.13 to 0.47)a0.26
(0.10 to 0.41)a0.32
(0.15 to 0.50)a0.30
(0.21 to 0.39)aStroke and TIA 0.28
(−0.94 to 1.48)−0.15
(−1.07 to 0.76)0.11
(−0.89 to 1.08)0.53
(−0.71 to 1.72)0.14
(−0.37 to 0.65)Atrial fibrillation −0.57
(−1.90 to 0.72)1.30
(0.38 to 2.19)a2.39
(1.45 to 3.32)a1.17
(0.02 to 2.29)a0.97
(0.46 to 1.48)aHeart failure 1.19
(−0.39 to 2.71)1.30
(0.21 to 2.36)a−0.26
(−1.45 to 0.90)1.42
(0.01 to 2.77)a0.98
(0.36 to 1.60)aDiabetes discordant Asthma −0.22
(−0.55 to 0.11)0.18
(−0.05 to 0.42)−0.26
(−0.51 to −0.01)a0.01
(−0.29 to 0.30)−0.07
(−0.20 to 0.07)Cancer 2.01
(1.09 to 2.91)a0.81
(0.16 to 1.46)a0.22
(−0.46 to 0.89)0.56
(−0.14 to 1.26)0.89
(0.53 to 1.25)aCOPD 0.99
(0.33 to 1.64)a0.85
(0.38 to 1.33)a0.89
(0.36 to 1.42)a1.12
(0.45 to 1.78)a0.95
(0.68 to 1.23)aDementia 0.38
(−0.69 to 1.42)0.42
(−0.34 to 1.18)−0.09
(−1.16 to 0.95)−0.63
(−1.91 to 0.61)0.17
(−0.30 to 0.64)Depression 0.10
(−0.05 to 0.24)−0.05
(−0.15 to 0.05)0.08
(−0.02 to 0.18)0.05
(−0.06 to 0.16)0.03
(−0.03 to 0.08)Epilepsy 0.39
(−1.15 to 1.87)−2.46
(−3.78 to −1.18)a−1.74
(−3.23 to −0.30)a−2.97
(−4.86 to −1.14)a−1.58
(−2.30 to −0.87)aHypothyroidism 0.33
(−0.18 to 0.85)0.28
(−0.09 to 0.65)−0.16
(−0.56 to 0.24)−0.08
(−0.52 to 0.36)0.13
(−0.08 to 0.34)Severe mental health disorder −1.76
(−2.58 to −0.95)a−0.54
(−1.34 to 0.24)−0.04
(−0.91 to 0.82)−1.06
(−2.25 to 0.11)−0.95
(−1.35 to −0.56)aCHD = coronary heart disease; CKD = chronic kidney disease; COPD = chronic obstructive pulmonary disease; TIA = transient ischemic attack.
Note: Based on multivariate linear regression analysis. Dependent variable is the logit–transformed achievement rate of intermediate outcomes indicators. Independent variables are the prevalence of diabetes and conditions concordant and discordant to diabetes. Analysis adjusted for age, sex, ethnicity, deprivation, number of general practitioners, Carr-Hill list size, and exception rate. Coefficients have been back-transformed to percentages from logit-transformed achievement rates. β is the fully adjusted, absolute percentage change in achievement rate across the overall intermediate outcomes, per 1% change in prevalence.
↵a P <.05.
Supplemental Appendixes
Supplemental Appendix 1. Empirical logit transformation and back transformation; Supplemental Appendix 2. Association between quality of diabetes care (process) and the prevalence of diabetes and of diabetes concordant conditions (sensitivity analysis based on QOF scores instead of achievement rates); Supplemental Appendix 3. Association between quality of diabetes care (intermediate outcomes) and the prevalence of diabetes and diabetes-concordant conditions (sensitivity analysis based on QOF scores instead of achivement rates)
Files in this Data Supplement:
- Supplemental data: Appendixes - PDF file
The Article in Brief
Impact of the Prevalence of Concordant and Discordant Conditions on the Quality of Diabetes Care in Family Practices in England
Ignacio Ricci-Cabello , and colleagues
Background This study sets out to explain the quality of diabetes care in family practices. It assesses the potential impact of the prevalence of diabetes-concordant conditions (conditions with related physiologic processes that may therefore be part of the same care management plan) such as obesity, hypertension, coronary heart disease, chronic kidney disease, stroke, atrial fibrillation and heart failure) and diabetes-discordant conditions (conditions that are not directly related to each other physiologically or in their care management) such as asthma, cancer, chronic obstructive pulmonary disease, dementia, depression, epilepsy, hypothyroidism and severe mental disorders. The study examines whether family practices with a higher proportion of patients with related cardiometabolic conditions may prioritize and more efficiently allocate resources for the management of these conditions. In comparison, practices with a higher proportion of patients with diabetes-discordant conditions might find it more difficult to deliver high-quality diabetes care because of competition for resources and attention from varying conditions.
What This Study Found Although the quality of diabetes care provided in practices is associated with the prevalence of other major chronic conditions, the nature and direction of the associations is only partially explained by the concordant-discordant model. Specifically, prevalence rates for four of seven concordant conditions (obesity, chronic kidney disease, atrial fibrillation and heart failure) were positively associated with quality of diabetes care. Similarly, negative associations were observed as predicted for two of eight discordant conditions examined (epilepsy and mental health). Observations for other concordant and discordant conditions, however, did not match predictions. The prevalence of hypertension and coronary heart failure, for example, were negatively associated with both processes and intermediate outcomes of diabetes. There were strong positive associations for diabetes quality of care and cancer and COPD.
Implications
- The authors conclude that while the concordant-discordant model does not fully explain the patterns of association between the prevalence of chronic conditions and the quality of diabetes care, the prevalence of a number of chronic conditions can be a predictor of quality of care for diabetes. The authors assert that incentive programs should consider the number of chronic conditions when assessing performance of individual clinicians.




{kind=link}