
Article Figures & Data
Figures
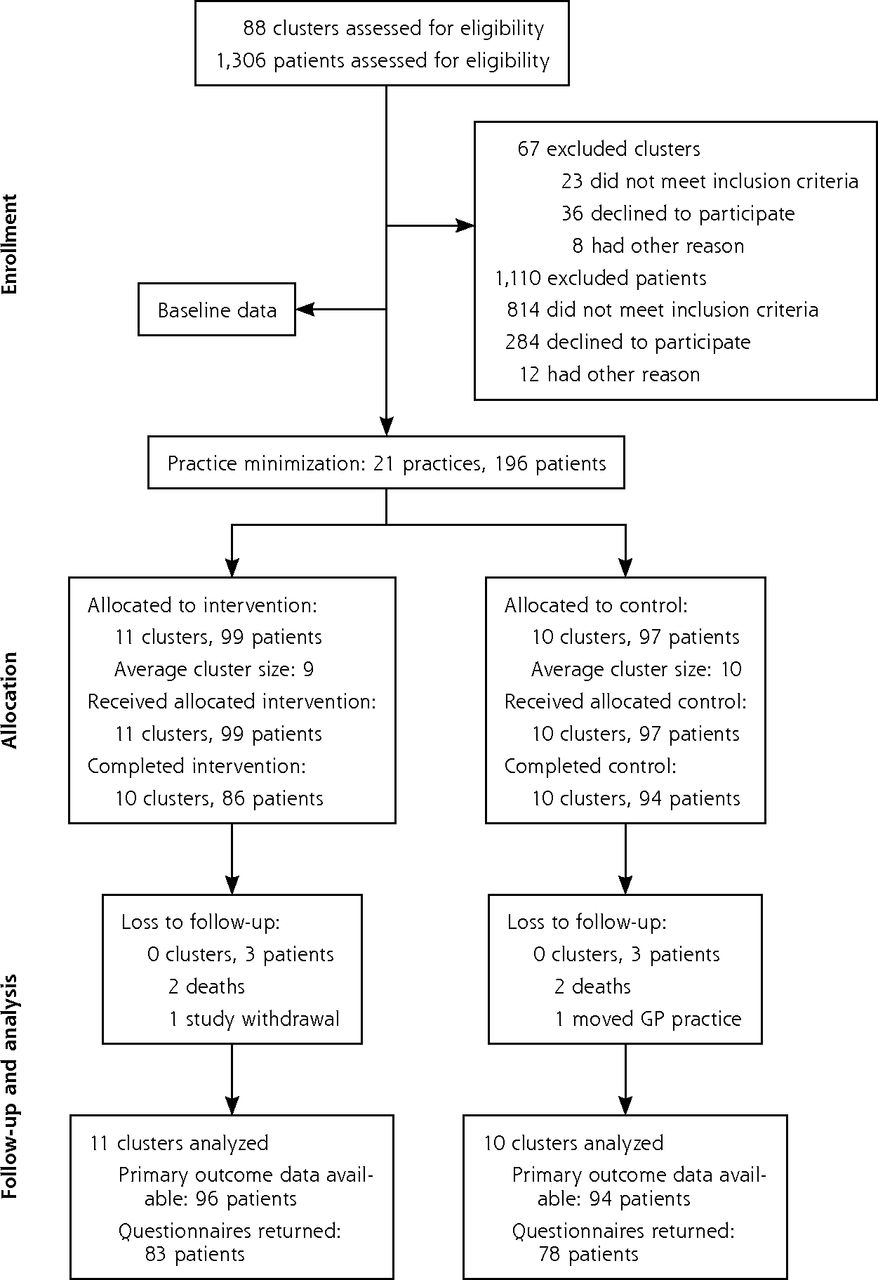
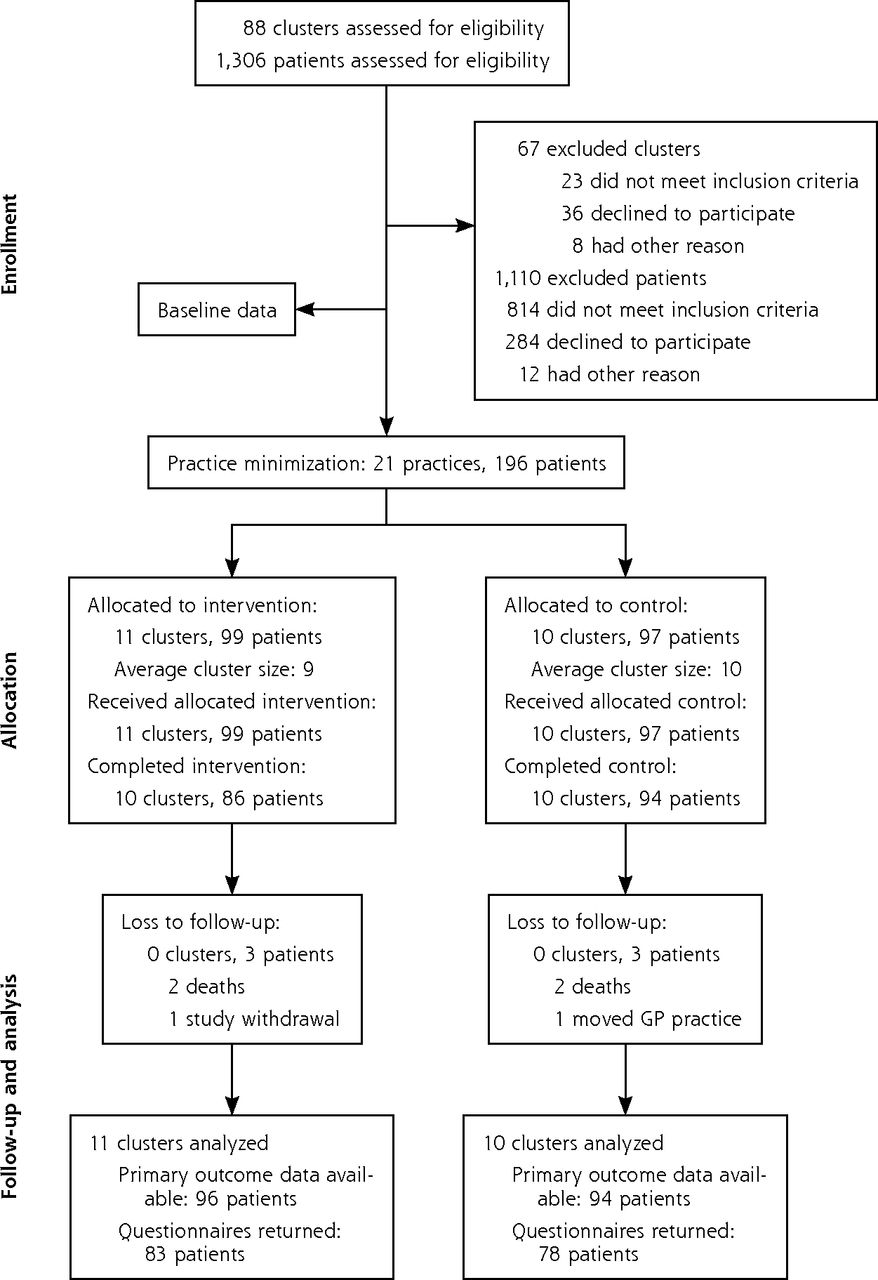
- Figure 1
Flow of practices and patients through the study.
GP = general practitioner.
Tables
Intervention Control Academic detailing with a pharmacist, which entailed one 30-min session in which a pharmacist visited the practice to discuss PIP, a review of medicines, and the web-based pharmaceutical treatment algorithms
Medicine review with web-based pharmaceutical treatment algorithms. GPs were asked to conduct 1 review per patient using the web-based platform to guide them through the process. The GP was presented with the specific PIP drug(s) for each patient, and for each PIP drug, was offered a treatment algorithm with the following structure:
1. The individual PIP with reason for concern
2. Alternative pharmacologic and nonpharmacologic treatment options
3. Background information (where relevant)
Patient information leaflets to give to patients during the review. Each leaflet:
1. Described the PIP and the reasons why it may be inappropriate
2. Outlined the alternative pharmacologic and nonpharmacologic therapies GPs may offerDelivery of usual care, which for public general medical services patients allows GPs to give a prescription on a monthly or 3-month basis
Receipt of simple, patient-level PIP postal feedback in the form of a list summarizing the medication class to which the individual patient’s potentially inappropriate medication belonged
No academic detailing visit, and no prompts to carry out a medicine review with the individual patientsGP = general practitioner; OPTI-SCRIPT = Optimizing Prescribing for Older People in Primary Care, a cluster-randomized controlled trial; PIP = potentially inappropriate prescribing.
- Table 2
Baseline Characteristics of Practices and Patients in Intervention and Control Groups
Characteristic Intervention Group Control Group Practices n = 11 n = 10 GMS list size, No. (%) ≤500 1 (9.1) 2 (20.0) 501–1,500 3 (27.3) 2 (20.0) ≥1,501 7 (63.6) 6 (60.0) Have a manager, No. (%) 8 (72.8) 7 (70.0) Location, No. (%) Urbana 8 (80.0) 8 (72.7) Mixed 3 (20.0) 2 (27.3) GPs per practice, mean (SD) 4.1 (3.1) 4.1 (2.1) Patients >70 years old per practice, mean (SD) 712.1 (525.3) 788.2 (987.2) Deprivation score, median (IQR)b 0.5 (–0.3 to 1.6) 1.4 (0.3 to 2.4) Patients n = 99 n = 97 Male, No. (%) 55 (55.6) 50 (51.5) Marital status, No. (%) Married 56 (56.6) 51 (53.1) Widowed 26 (26.3) 32 (33.3) Single 14 (14.1) 10 (10.4) GMS card holder, No. (%) 88 (88.9) 95 (97.9) Age, mean (SD) 77.1 (4.9) 76.4 (4.8) Repeat medications, mean (SD) 10.2 (4.5) 9.5 (4.1) PIP drugsc Mean (SD) 1.31 (0.6) 1.39 (0.6) Median (IQR) 1 (1–2) 1 (1–2) Most prevalent PIP drug: proton pump inhibitors, No. (%) 53 (53.3) 65 (67.7) GMS = general medical services; GP = general practitioner; IQR = interquartile range; PIP = potentially inappropriate prescribing.
Note: Figures are numbers (percentages) unless stated otherwise.
↵a Urban area: relatively small center of population, with at least 5,000 residents.37
↵b Population-weighted deprivation score for each practice; higher scores mean practices are situated in more socioeconomically deprived areas.
↵c All patients had at least 1 potentially inappropriate prescription at baseline.
- Table 3
Potentially Inappropriate Prescriptions at Baseline in Intervention and Control Groups
Potentially Inappropriate Prescription Intervention Group, No. (%) (n = 99) Control Group, No. (%) (n = 97) Proton pump inhibitor at maximum therapeutic dosage for >8 weeks 53 (53.3) 65 (67.7) NSAIDs: long-term use, interactions with certain medications (eg, diuretic) 21 (21.2) 16 (16.8) Therapeutic duplication: any regular duplicate drug class prescription (eg, 2 concurrent opiates, NSAIDs) 19 (19.2) 13 (13.5) Long-term use (>1 month) of long-acting benzodiazepines 14 (14.4) 8 (8.3) Steroid without bisphosphonate 9 (9.1) 4 (4.2) Bladder antimuscarinics: contraindications and interactions with certain medications 1 (1.0) 9 (9.4) Prolonged use (>1 week) of first-generation antihistamines 4 (4.0) 2 (2.1) Tricyclic antidepressants: contraindications and interactions with certain medications (eg, opiate, calcium channel blocker) 1 (1.0) 5 (5.2) Thiazide diuretic in patient with gout 3 (3.0) 2 (2.1) Aspirin: contraindications and interactions with certain medications (eg, warfarin) 3 (3.0) 1 (1.0) Digoxin: inappropriate dose 1 (1.0) 3 (3.1) Calcium channel blocker: contraindications and interactions with certain medications 0 (0.0) 3 (3.1) NSAID = nonsteroidal anti-inflammatory drug.
Outcome Intervention Group, No. (%) Control Group, No. (%) Adjusteda Odds Ratio (95% CI) Adjusteda Incidence Rate Ratio (95% CI) Mean Differencea,b (95% CI) P Value Primary outcome: proportion with PIP Baseline 99 (100) 97 (100) – – – – Intervention completion 52 (52.5) 75 (77.3) 0.32 (0.15–0.70) – – .02 Primary outcome: mean (SD) PIP Baseline 1.31 (0.6) 1.39 (0.6) – – – – Intervention completion 0.70 (0.1) 1.18 (0.1) – – −0.48 (–0.80 to –0.17) .02 Additional outcome: median (IQR) PIP per patient Baseline 1 (1–2) 1 (1–2) – – – – Intervention completion 1 (0–1) 1 (1–2) – – – – Additional outcome: Poisson regression Baseline 99 (100) 97 (100) – – – – Intervention completion 52 (52.5) 75 (77.3) – 0.71 (0.50–1.02)c – .49 IQR = interquartile range; PIP = potentially inappropriate prescribing.
Note: Values are numbers (percentages) unless stated otherwise. We used the Bonferroni method to account for multiple comparisons.
↵a Adjusted for age, sex, baseline number of PIP drugs, baseline number of repeat medications, number of general practitioners, and practice location.
↵b Results from modeling the number of PIP drugs per patient with Poisson regression analysis adjusted for age, sex, baseline number of PIP drugs, baseline number of repeat medications, number of general practitioners, and practice location.
↵c Results from unadjusted cluster-level t test.
Outcome Intervention Group Control Group Adjusteda Odds Ratio or Mean Difference (95% CI) P Value Drug-specific outcomes Proton pump inhibitor, No. (%) Baseline 53 (53.5) 65 (67.7) Intervention completion 23 (23.2) 46 (47.4) 0.30 (0.14–0.68) .04 Duplicate, No. (%) Baseline 19 (19.2) 13 (13.5) Intervention completion 11 (11.1) 11 (11.3) 0.83 (0.32–2.13) .99 Long-term benzodiazepines, No. (%) Baseline 14 (14.1) 8 (8.1) Intervention completion 9 (9.1) 9 (9.1) 1.31 (0.47–3.68) .99 Patient-reported outcomes WBQ-12 score: mean well-beingb Baseline 24.3 24.4 Intervention completion 23.6 24.0 –0.41 (−0.80 to 1.07) .99 BMQ score: median necessity-concern differentialc Baseline 7.0 5.8 Intervention completion 6.0 6.0 0.16 (−1.85 to 1.07) .99 BMQ = Beliefs About Medicine Questionnaire; WBQ-12 = 12-item Well-Being Questionnaire.
Note: Figures are numbers (percentages) unless stated otherwise. The Bonferroni method was used to account for multiple comparisons.
↵a Adjusted for age, sex, baseline number of PIP drugs, baseline number of repeat medications, number of general practitioners, and practice location.
↵b Well-being score ranges from 0 to 36 (1–12 low, 13–24 medium, 25–36 high).
↵c Scale from −20 to 20, where positive scores indicate benefits outweigh risks.
- Table 6
Comparison of PIP in the OPTI-SCRIPT Study Population With the PCRS National Comparator
PIP Outcome OPTI-SCRIPT Intervention Group OPTI-SCRIPT Control Group PCRS National Comparator Presence of PIP PIP at baseline 99 (100) 97 (100) 103,261 (100) PIP at intervention completion 52 (52.5) 75 (77.3) 75,401 (73.1) No PIP at intervention completion 47 (47.5) 22 (22.7) 27,860 (26.9) Crude odds ratio (95% CI) 0.4 (0.3–0.6) – 1.0 (ref) Decrease in PIP PIP at baseline 99 (100) 97 (100) 103,261 (100) PIP same or increased at intervention completion 42 (42.4) 65 (67.0) 67,188 (65.1) PIP decreased at intervention completion 57 (57.6) 32 (32.9) 36,073 (34.9) Crude odds ratio (95% CI) 2.5 (1.8–4.0) – 1.0 (ref) OPTI-SCRIPT = Optimizing Prescribing for Older People in Primary Care, a cluster-randomized controlled trial; PCRS = Primary Care Reimbursement Services; PIP = potentially inappropriate prescribing; ref = reference group.
Note: Numbers (percentages) of participants are presented, unless otherwise stated.
Supplemental Appendixes
Supplemental Appendix 1. Selected prescribing criteria/prescribing indicator; Supplemental Appendix 2. OPTI-SCRIPT website materials
Files in this Data Supplement:
- Supplemental data: Appendixes - PDF file
The Article in Brief
Effectiveness of a Multifaceted Intervention for Potentially Inappropriate Prescribing in Older Patients in Primary Care: A Cluster-Randomized Controlled Trial (OPTI-SCRIPT Study)
Barbara Clyne , and colleagues
Background Potentially inappropriate prescribing of medications is a common and growing public health concern that can result in increased death, adverse drug reactions, hospitalizations, and costs. Previous research in Ireland showed that 36 percent of those aged 70 years or older received at least one potentially inappropriate prescription in 2007 with an associated cost of more than 45 million euros. In this study, researchers in Ireland test the effectiveness of an intensive multifaceted intervention for reducing potentially inappropriate prescribing (PIP) in primary care.
What This Study Found The year-long intervention was effective in reducing PIP. It included face-to-face academic detailing with a pharmacist, medicine review with web-based pharmaceutical treatment algorithms that provided alternative treatment options, and tailored patient information leaflets. At the completion of the intervention, the percentage of patients having PIP was 52 percent in the intervention group compared with 77 percent in the control group. The average number of PIP drugs per patient in the intervention group was 0.70 compared with 1.18 in the control group. Potentially inappropriate prescribing of proton pump inhibitors, which was highly prevalent at baseline (60 percent) was greatly improved through the intervention.
Implications
- The authors suggest that face-to-face, patient-specific detailing encouraged immediate action rather than simply providing educational support or information. They call for future research to examine tailoring of this intervention to influence different cases of PIP.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- DepRescribing inapprOpriate Proton Pump InhibiTors (DROPIT): study protocol of a cluster-randomised controlled trial in Swiss primary care
- Potentiality of algorithms and artificial intelligence adoption to improve medication management in primary care: a systematic review
- Ambulatory Medication Safety in Primary Care: A Systematic Review
- Safer Prescribing and Care for the Elderly (SPACE): a cluster randomised controlled trial in general practice
- Deprescribing intervention activities mapped to guiding principles for use in general practice: a scoping review
- Integrating clinical pharmacists within general practice: protocol for a pilot cluster randomised controlled trial
- Evaluation of the General Practice Pharmacist (GPP) intervention to optimise prescribing in Irish primary care: a non-randomised pilot study
- Are payment methods for prescription drugs associated with polypharmacy in older adults in Ireland? Evidence from the TILDA cohort study
- Evaluation of the General Practice Pharmacist (GPP) intervention to optimise prescribing in Irish primary care: a non-randomised pilot study
- Why evidence still matters to general practice: James Mackenzie Lecture 2019
- Economic impact of potentially inappropriate prescribing and related adverse events in older people: a cost-utility analysis using Markov models
- Effectiveness of an intervention to optimise the use of mirabegron for overactive bladder: a quasi-experimental study in primary care
- The PIPc Study--application of indicators of potentially inappropriate prescribing in children (PIPc) to a national prescribing database in Ireland: a cross-sectional prevalence study
- Safer Prescribing and Care for the Elderly (SPACE): a pilot study in general practice
- Beliefs about prescribed medication among older patients with polypharmacy: a mixed methods study in primary care
- PIPc study: development of indicators of potentially inappropriate prescribing in children (PIPc) in primary care using a modified Delphi technique
- In This Issue: Multilevel Effects