
Article Figures & Data
Figures
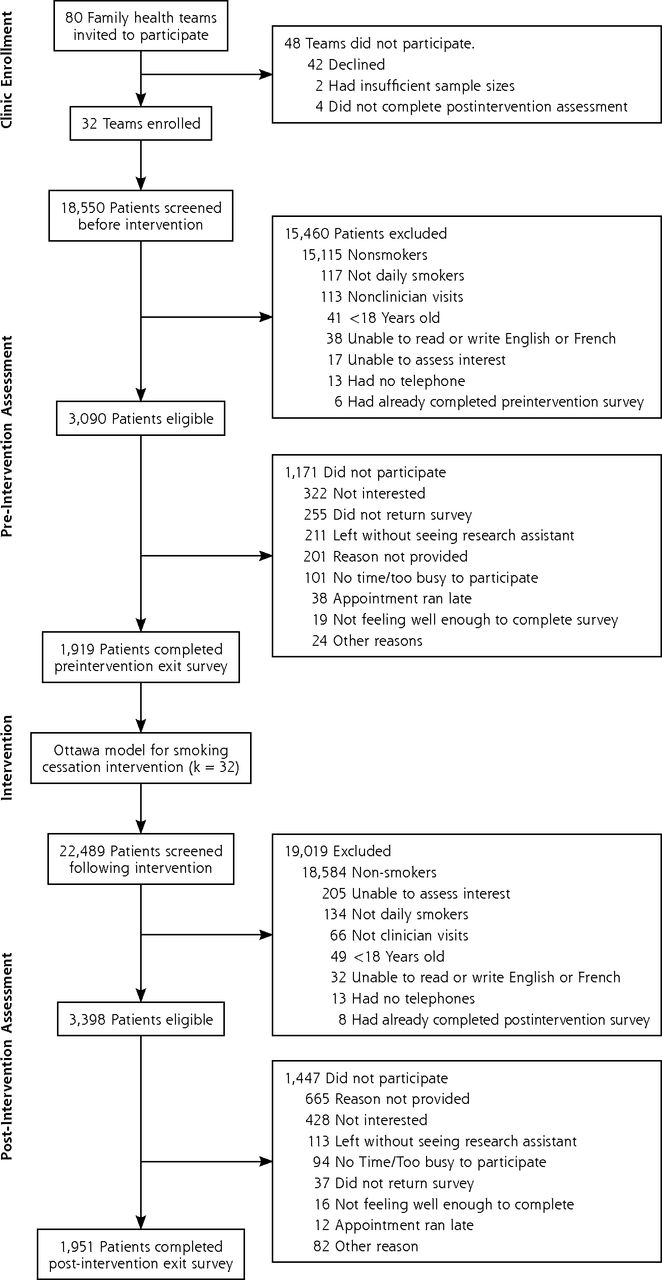
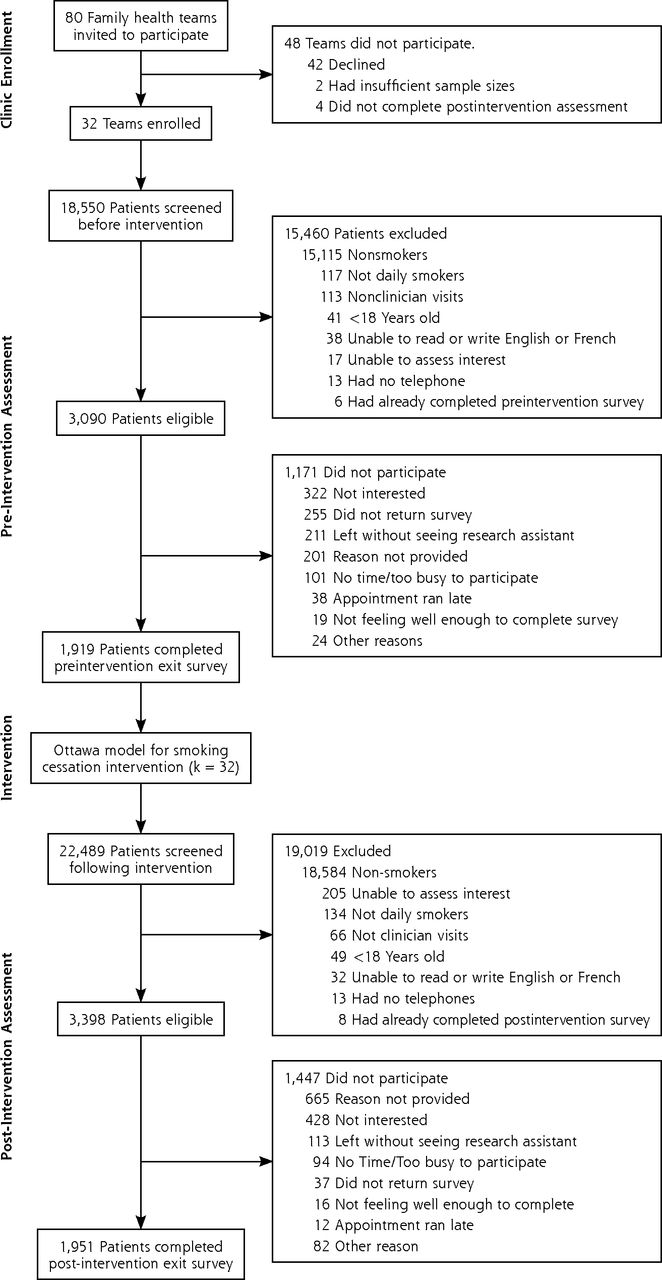
- Figure 1
Flow of practices and patients through the study.
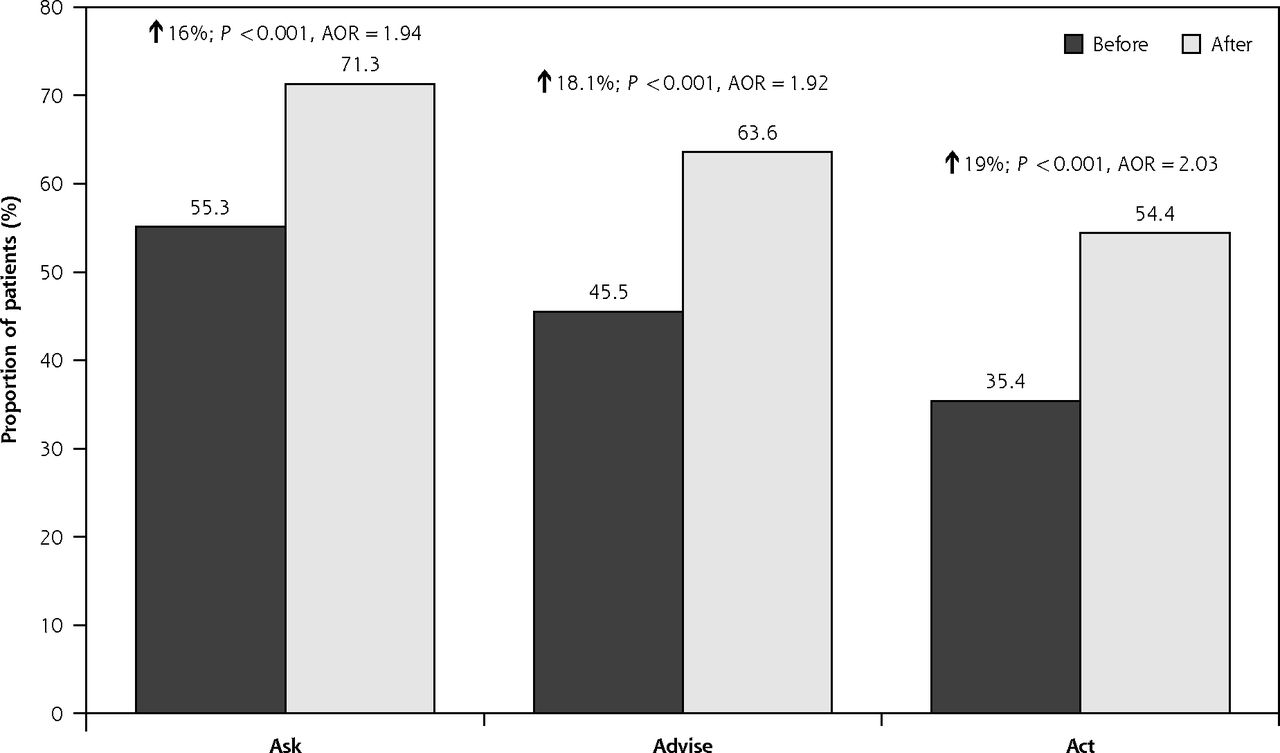
- Figure 2
Clinic performance in the 3 A’s delivery before and after OMSC knowledge translation intervention.
AOR = adjusted odds ratio; OMSC = Ottawa Model for Smoking Cessation; 3 A’s = Ask, Advise, Act.
Note: The AORs presented control for clinic- and provider-level variance between clusters, availability of cost-free nicotine replacement therapy, gender of the patient, self-reported time of first cigarette, and purpose of visit; based on inclusion of 32 clinics and 481 providers. P values are based on the Wald statistic.

Tables
Component Description Outreach facilitation visits A trained outreach facilitator worked with each primary care clinic over a 3-month period to do the following:
• Provide information and recommendations on the integration of evidence-based smoking cessation strategies into clinical practice
• Facilitate the development of a clinic tobacco control protocol for integrating evidence-based smoking cessation strategies into all clinic appointments
• Define roles and responsibilities of clinic staff in delivering evidence-based smoking cessation treatments
• Support communications and training activities for members of the clinic staffClinic staff training Frontline physicians and nurse practitioners participated in a 3-hour training session that provided information and skills training for addressing tobacco use with patients in a busy primary care practice
Key staff who would be responsible for delivering quit plan visits (typically nurses, nurse practitioners, or pharmacists) attended an intensive 1-day training session that taught them how to conduct the quit plan visit and follow-up visits based on evidence-based practiceStandardized staff and patient tools All materials were designed to support 3 A’s delivery and reduce the amount of face-to-face time required. They included the following:
• A patient tobacco use survey to document smoking history
• A checklist-style smoking cessation consult form
• A quit plan booklet for smokers ready to quit
• A booklet for smokers not ready to quit
• Clinic waiting room posters and materialsReal time prompts and EMR tools Real time, point-of-care reminders (eg, standard smoking status questions and prompts to deliver brief advice) were introduced and embedded in vital signs screening forms
Standardized forms were embedded in EMR systems to guide 3 A’s delivery for advice, quit plan, and follow-up visitsFollow-up support and counseling Practices were introduced to a telephone-based Smoker’s Follow-up System for patients ready to quit (5 triage calls over a 2-month period delivered by Interactive Voice Response System) with additional support from trained smoking cessation counselors available for patients struggling with their quit attempts Audit and feedback Practices were given feedback reports on the results of pre- and postintervention assessments
They also received audit and feedback regarding implementation activities 1 to 4 months following initiation of intervention programEMR = electronic medical record; 3 A’s = Ask, Advise, Act.
Parameter Preintervention
n = 1,919Postintervention
n = 1,951Combined
N = 3,870χ2 P Value Age range, % 4.6 .33 18–24 y 8.76 8.06 8.41 25–39 y 20.92 23.61 22.27 40–54 y 36.23 34.37 35.30 55–64 y 21.55 21.42 21.49 ≥65 y 12.53 12.53 12.53 Sex, % 38.4 <0.001 Female 62.70 52.81 57.74 Male 37.30 47.19 42.26 Years of formal education, % 0.9 .81 <High school 3.96 3.83 3.89 High school 51.70 50.35 51.01 University 37.75 39.29 38.53 Graduate school 6.59 6.54 6.57 Smoking-related illness,a % 0.7 .41 No 72.33 73.50 72.92 Yes 27.67 26.50 27.08 Cigarettes per day, % 2.5 .29 <15 45.54 47.92 46.74 15–25 46.53 44.08 45.30 >25 7.92 8.00 7.96 Time to first morning cigarette, % 7.9 .005 >30 minutes 37.59 42.03 39.82 ≤30 minutes 62.41 57.97 60.18 Readiness to quit,b % 0.1 .81 >30 days 69.05 68.68 68.87 next 30 days 30.95 31.32 31.13 Average self-efficacy with quitting,c % 0.2 .64 Low (1–6) 86.15 85.60 85.88 High (7–10) 13.85 14.40 14.12 Anxiety/Depression, % 0.3 .57 No 55.21 56.11 55.66 Yes 44.79 43.89 44.34 Psychiatric Co-Morbidity, % 0.8 .38 No 88.08 87.13 87.60 Yes 11.92 12.87 12.40 Purpose of visit, % 5.0 .03 Follow-up/other 80.86 77.93 79.36 Periodic exam 19.14 22.07 20.64 ↵a “Do you have… heart disease, stroke, heart failure/cancer/chronic obstructive pulmonary disease (COPD)?” (1 = yes, 0 = no for each condition).
↵b “Which of the following best describes your feelings about smoking right now?” (responses: 1 = ready to quit in next 30 days, 0 = ready to quit in next 6 months or not ready to quit).
↵c ”On a scale of 1 to 10, how confident are you that you would be able to quit smoking at this time?” (1 = not at all confident, 10 = extremely confident).
- Table 3
Final Model for the Multi-Level Analysis of Clinic-, Clinician-, and Patient-Level Characteristics Associated With Rates of Clinician Delivery of the 3 A’s (Ask, Advise, Act)
Parameter Ask Advise Act to Assist With Cessation Time, AOR (95% CI) Preintervention (reference) 1.00 1.00 1.00 Postintervention 2.07 (1.77–2.43) 2.32 (1.95–2.76) 2.49 (2.09–2.97) Clinic-level variables, AOR (95% CI) Presence of a physician champion No (reference) 1.00 1.00 1.00 Yes 1.66 (1.13–2.44) Provider-level variables, AOR (95% CI) Importance of cessationa Low (reference) 1.00 1.00 1.00 High 1.25 (1.02–1.53) 1.35 (1.10–1.64) Patient-level variables, AOR (95% CI) Age, y 18–24 (reference) 1.00 1.00 1.00 25–39 1.11 (0.80–1.54) 1.55 (1.10–2.19) 40–54 1.31 (0.95–1.81) 1.85 (1.33–2.58) 55–64 1.55 (1.09–2.20) 1.85 (1.30–2.64) ≥65 1.53 (1.05–2.25) 1.69 (1.14–2.49) Formal education <High school (reference) 1.00 1.00 1.00 High school 0.77 (0.50–1.18) University 0.66 (0.43–1.02) Graduate school 0.54 (0.32–0.90) Smoking-related illnessb No (reference) 1.00 1.00 1.00 Yes 1.28 (1.07–1.53) 1.26 (1.02–1.54) Cigarettes per day, No. <15 (reference) 1.00 1.00 1.00 15–25 1.38 (1.14–1.67) 1.52 (1.25–1.84) >25 1.25 (0.89–1.78) 1.62 (1.14–2.29) Time to first morning cigarette >30 min (reference) 1.00 1.00 1.00 <30 min 1.23 (1.05–1.45) 1.23 (1.02–1.49) 1.31 (1.08–1.59) Readiness to quitc Not ready in next 30 d (reference) 1.00 1.00 1.00 Ready in next 30 d 1.29 (1.10–1.53) 1.50 (1.25–1.80) 1.60 (1.33–1.92) Self-efficacy with quittingd Low (reference) 1.00 1.00 1.00 High 1.36 (1.06–1.74) Purpose of visit Follow-up (reference) 1.00 1.00 1.00 Annual exam 2.79 (2.26–3.45) 1.98 (1.59–2.46) 1.84 (1.49–2.27) Random Variance, Variance (SE) Provider 0.214 (0.068) 0.128 (0.059) 0.088 (0.058) Clinic 0.154 (0.060) 0.087 (0.043) 0.083 (0.041) Model fit statistics Akaike information criterion 3,921.93 3,123.72 3,001.19 Bayesian information criterion 3,939.52 3,150.10 3,030.50 Note: Models are adjusted for clinic- and provider-level clustering effects and all other variables in the column.
↵a “As a practitioner, how would you describe the importance you place personally on helping your patients quit smoking?” (Responses: 1–5 Likert scale, 1 = not important, 5 = extremely important)
↵b “Do you have... heart disease/ stroke/ heart failure/ cancer/ chronic obstructive pulmonary disease (COPD)?” (1 = yes, 0 = no for each condition)
↵c “Which of the following best describes your feelings about smoking right now?” (Responses: 1 = Ready to quit in next 30 days, 0 = Ready to quit in next 6 months or not ready to quit.)
↵d “On a scale of 1 to 10, how confident are you that you would be able to quit smoking at this time?” (1 = Not at all confident, 10 = Extremely confident.)
- Table 4
Implementation of Ottawa Model for Smoking Cessation 10 Best Practices Before and After Intervention
Before Intervention After Intervention Clinics with the OMSC 10 Best Practices implemented, by best practice, % 1. Clinic task force formed 3.1 93.8 2. Clinic tobacco control protocol developed 0.0 96.9 3. Tobacco use queried and documented for all clinic patients 28.1 81.3 4. Training in tobacco dependence treatment offered to health care providers in last year 28.1 90.6 5. Staff trained and available to provide tobacco dependence treatment 59.4 96.9 6. Self-help materials readily available to patients, family members, and staff 68.8 90.6 7a. EMR or other real time prompt in place to inform clinician of patient smoking status 3.1 90.6 7b. EMR supports in place (smoking status identification, consult form, etc) 3.1 93.8 8. Process to follow-up tobacco users for at least 1 month after clinic visit in place 43.8 93.8 9. Process to evaluate quality or program implementation in place 3.1 71.9 10. Process to provide feedback to clinicians about performance in place 3.1 81.3 Average number of best practices implemented, No. 2.4 8.9 Clinics with 10 best practices implemented, % 0.0 59.3 EMR = electronic medical record; OMSC = Ottawa Model for Smoking Cessation.
Note: Based on data from 32 primary care practices.
The Article in Brief
Increasing Rates of Tobacco Treatment Delivery in Primary Care Practice: Evaluation of the Ottawa Model for Smoking Cessation
Sophia Papadakis , and colleagues
Background The Ottawa Model for Smoking Cessation (OMSC) provides clinicians with multiple components to help patients quit smoking. It includes use of the three As: Ask (identify smoking status), Advise (counsel patients to quit smoking), and Act (assist with cessation). This study examines the association between implementation of the OMSC program and rates at which the 3 As are delivered to tobacco users in primary care practices.
What This Study Found The OMSC is successful in increasing rates of tobacco treatment delivery. In 32 primary care practices with 481 clinicians and 3,870 patients, rates of delivery of the three As increased significantly following implementation of the program. Clinicians are significantly more likely to address tobacco use during periodic exams, indicating that they may be missing opportunities when patients present for other reasons.
Implications
- The results of this evaluation lend support to existing evidence about the effectiveness of multicomponent interventions in influencing tobacco treatment delivery in primary care settings.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Understanding the implementation strategy of a secondary care tobacco addiction treatment pathway (the CURE project) in England: a strategic behavioural analysis
- Smoking cessation: health system challenges and opportunities
- Improving Smoking and Blood Pressure Outcomes: The Interplay Between Operational Changes and Local Context
- Delivering high value therapies in COPD: the secret is in the marketing
- From Good to Great: The Role of Performance Coaching in Enhancing Tobacco-Dependence Treatment Rates
- Prospective, Cluster-Randomized Trial to Implement the Ottawa Model for Smoking Cessation in Diabetes Education Programs in Ontario, Canada
- Managing smoking cessation
- In This Issue: Decisions, Decisions