
Article Figures & Data
Figures
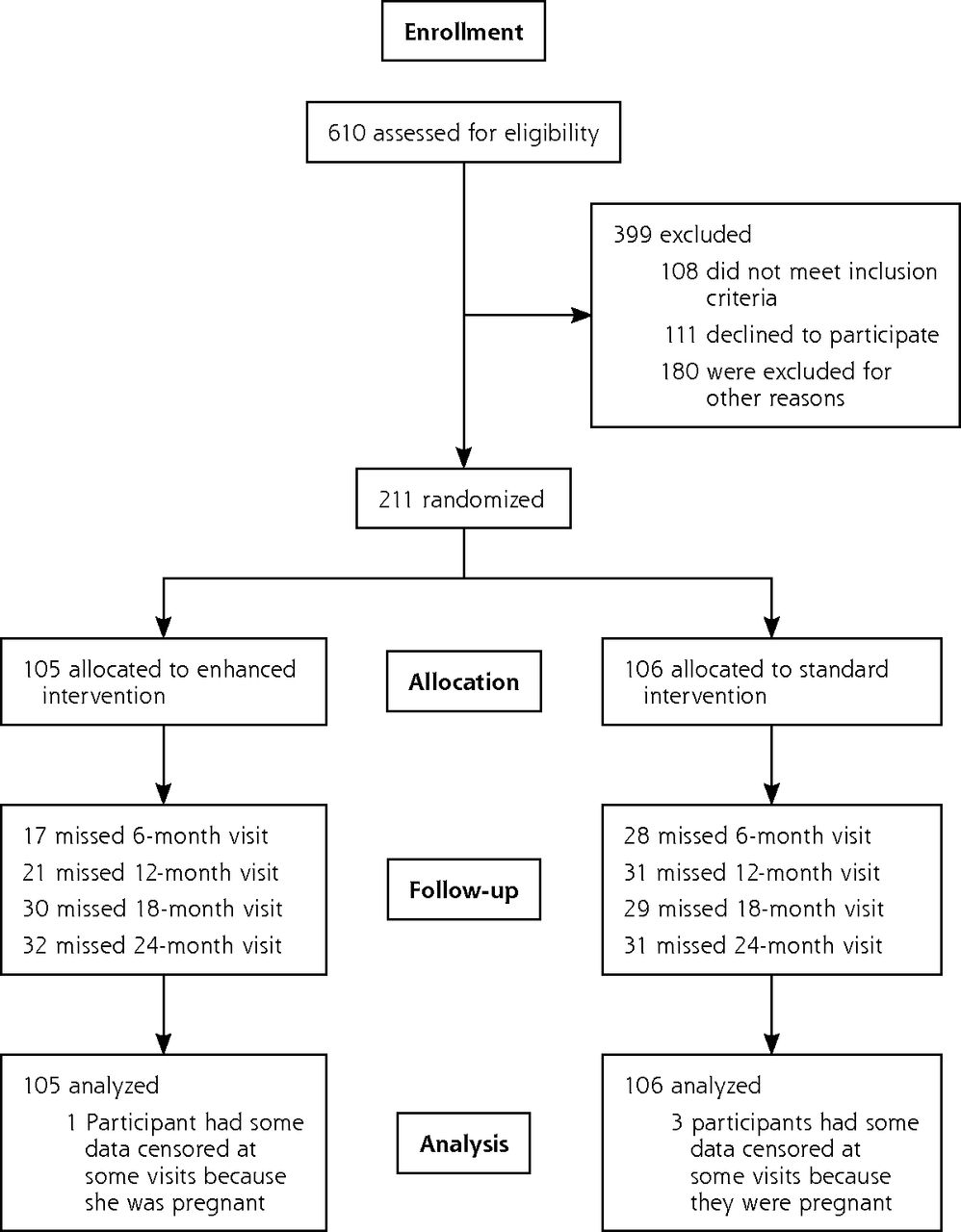
- Figure 1
CONSORT diagram of participant flow.
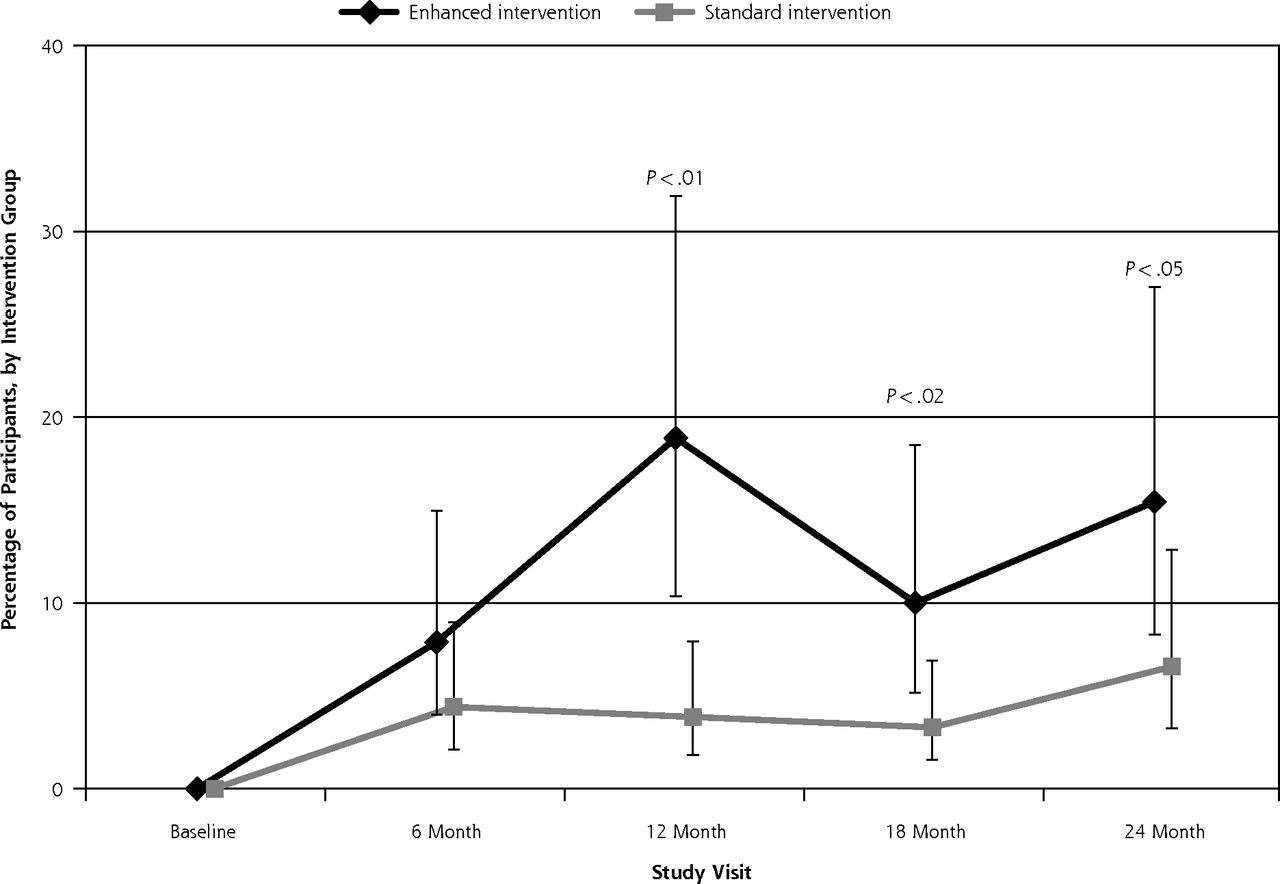
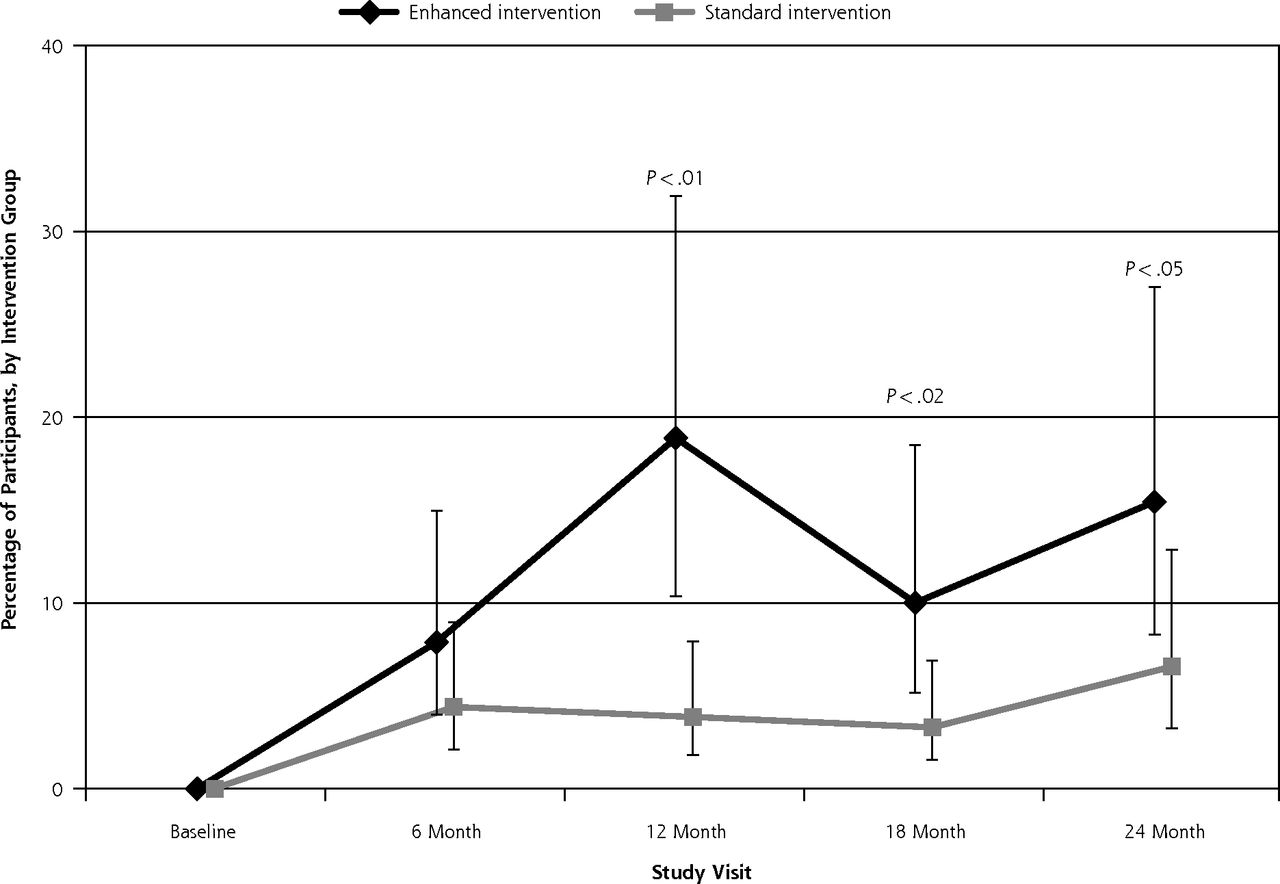
- Figure 2
Percentage of participants attaining 5% weight loss from baseline by intervention group over 24 months.
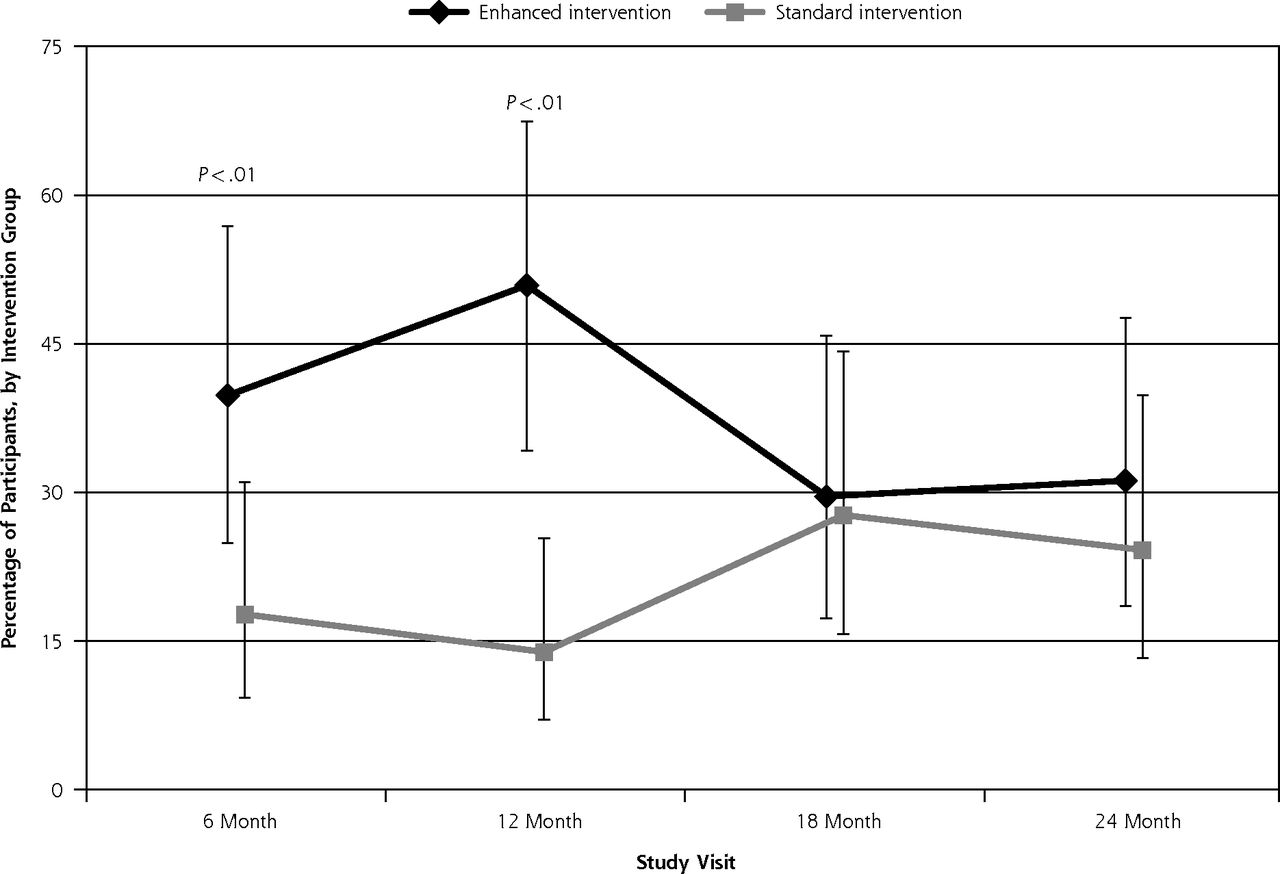
- Figure 3
Percentage of participants attaining ACSM guideline levels of physical activity by intervention group over 24 months.
ACSM = American College of Sports Medicine.


Tables
Characteristic Enhanced Intervention n = 106 Standard Intervention n = 105 P Value Age, mean (SD), y 48.5 (11.9) 48.6 (112.1) .96 Weight, mean (SD), kg 104.8 (21.6) 102.1 (18.7) .35 Body mass index, mean (SD) 37.7 (6.5) 37.8 (6.7) .93 Waist circumference, mean (SD), cm 116.0 (15.1) 114.8 (14.1) .54 Physical activity,a mean (SD), min/wk 20.3 (26.0) 22.1 (28.6) .65 Race/ethnicity, No. (%) .44 White 83 (79.0) 92 (86.8) Hispanic 6 (5.7) 3 (2.8) Black 11 (10.5) 9 (8.5) Other 5 (4.8) 2 (1.9) Education, No. (%) .47 High school or less 25 (23.8) 23 (22.33) Some college 31 (29.5) 22 (21.35) College graduate or other 47 (46.7) 57 (55.34) Female sex, No. (%) 79 (75.2) 88 (83.0) .18 Household income, No. (%) .97 <$25,000 15 (14.3) 17 (16.0) $25,000–$75,000 48 (45.7) 47 (44.3) >$75,000 40 (38.1) 39 (36.8) Unknown 2 (1.9) 3 (2.8) Employment, No. (%) .55 Full time 57 (54.3) 64 (60.4) Part time 25 (23.8) 17 (16.0) Not employed 22 (21.0) 24 (22.6) Don’t know 1 (0.9) 1 (0.9) Medical Conditions, No. (%) Hypertension 50 (47.6) 54 (50.9) .68 Diabetes 15 (14.3) 20 (18.9) .46 Dyslipidemia 47 (44.8) 41 (38.7) .40 Osteoarthritis 17 (16.2) 16 (15.1) .86 Congenital heart disease 3 (2.9) 3 (2.8) .99 ↵a Minutes of moderate and vigorous physical activity per week.
- Table 2
Change from Baseline in Weight and Minutes of Moderate and Vigorous Physical Activity per Week Over 24 Months
Study Visit Weight, Average (95% CI), kg Physical Activity, Average (95% CI), min/wk EI Group SI Group EI Group SI Group Baseline 103.8 (99.8 to 107.8) 102.8 (98.8 to 106.8) 20.6 (0.0 to 44.4) 23.0 (0.0 to 46.7) 6 Mo −5.0 (−6.4 to −3.5) −3.4 (−4.9 to −1.9) 95.7 (71.9 to 119.4) 67.9 (44.2 to 91.6) 12 Mo −5.4 (−6.9 to −3.9) −3.8 (−5.3 to −2.3) 126.1 (102.3 to 149.8) 73.3 (49.6 to 97.0) 18 Mo −4.4 (−5.9 to −2.9) −4.3 (−5.8 to −2.8) 103.6 (80.0 to 127.5) 63.3 (39.6 to 87.0) 24 Mo −4.1 (−5.6 to −2.6) −4.0 (−5.5 to −2.5) 101.3 (77.6 to 127.4) 75.0 (51.3 to 98.7) Group by Visit Interaction F ratio F3,620 = 3.17a; P = .02 F4,832 = 2.49b; P = .04 EI = enhanced intervention; SI = standard intervention.
Note: Weight at baseline is actual weight; weights at 6, 12, 18, and 24 months are weight changes from baseline.
↵a Interaction F statistic for change in weight; model adjusted for age, sex, and race/ethnicity.
↵b Interaction F statistic for physical activity minutes; model adjusted for age, sex, and race/ethnicity.
Type of Contact Enhanced Intervention Standard Intervention Per Protocol Average Actual Per Protocol Average Actual Lifestyle counselor, face-to-face counseling, year 1 3 2.7 3 2.8 Lifestyle counselor, telephone calls, year 1 8 7 — — Food and exercise journals — — Journals completed 24 14 — — Weekly weights recorded 24 12 — — Fat grams recorded 24 11 — — Physical activity recorded 24 10.5 — — Tailored mailings Nutrition reports, year 1 4 3.2 — — Physical activity reports, year 1 13 5.9 — — Physical activity reports, year 2 4 1.4 — —
Supplemental Appendixes
Supplemental appendixes in pdf.
Files in this Data Supplement:
- Supplemental data: Appendixes - PDF file
The Article in Brief
A Randomized Clinical Trial of a Tailored Lifestyle Intervention for Obese, Sedentary, Primary Care Patients
Charles B. Eaton , and colleagues
Background Tailored interventions that match individual patient characteristics with treatment may help patients lose weight and increase physical activity. Such programs implemented by print, telephone, and/or video, without extensive face-to-face counseling, may be an effective model for primary care patients. This study uses weekly telephone counseling calls, individually tailored educational materials and DVDs focused on diet and physical activity over the first year, with a tapered maintenance phase during the second year.
What This Study Found A home-based weight loss and physical activity intervention for obese, sedentary adult primary care patients is effective in promoting weight loss and increasing physical activity, with effects peaking at 12 months but waning at 24 months. In this study, by the end of the active treatment phase, almost half of the enhanced intervention group lost more than 5 percent of baseline weight � a clinically significant amount � and one-third maintained the loss at 24 months. The enhanced intervention group also reported significantly more minutes of moderate to vigorous physical activity over time than the standard intervention group. Similar trends were found for absolute weight loss and the percentage reaching national guidelines for physical activity. Overall, the benefits appear to peak at 12 months for both weight loss and increasing physical activity, with no statistically significant difference in benefit between the groups at 24 months.
Implications
- These findings suggest that referral by a primary care physician to a home-based program with limited face-to-face contact can lead to weight loss and increases in moderate to vigorous physical activity.
- The authors call for research to examine the use of ancillary health care staff or peer counselors in combination with computerized tailoring software, as well as technology such as web e-mails, text messages or smart phone apps, to provide support and tailored content.
Annals Journal Club
Jul/Aug 2016: A Randomized Clinical Trial of a Tailored Lifestyle Intervention for Obese, Sedentary, Primary Care Patients
The Annals of Family Medicine encourages readers to develop a learning community of those seeking to improve health care and health through enhanced primary care. You can participate by conducting a RADICAL journal club and sharing the results of your discussions in the Annals online discussion for the featured articles. RADICAL is an acronym for Read, Ask, Discuss, Inquire, Collaborate, Act, and Learn. The word radical also indicates the need to engage diverse participants in thinking critically about important issues affecting primary care and then acting on those discussions.1
HOW IT WORKS
In each issue, the Annals selects an article or articles and provides discussion tips and questions. We encourage you to take a RADICAL approach to these materials and to post a summary of your conversation in our online discussion. (Open the article online and click on "TRACK Discussion: Submit a comment.") You can find discussion questions and more information online at: http://www.AnnFamMed.org/site/AJC/.
CURRENT SELECTION
Article for Discussion
Eaton CB, Hartman S, Perzanowski E, et al. A randomized clinical trial of a tailored lifestyle intervention for obese, sedentary, primary care patients. Ann Fam Med 2016;14(4):311-319.
Discussion Tips
This article provides a chance to consider a pragmatic intervention for one of the country's biggest health problems.
Discussion Questions
- What question is asked by this study and why does it matter?
- Why did the authors choose this lifestyle intervention? How does this intervention differ from other programs for obese, sedentary adults?
- How appropriate is the block-randomized controlled trial design for answering this question?
- To what degree can the findings be accounted for by:
- How patients were selected, excluded, randomized, and lost to follow-up?
- How the main outcome variables were measured or self-reported?
- Confounding (false attribution of causality because 2 variables discovered to be associated actually are associated with a 3rd factor)? How do the authors attempt to control for confounding in their analysis?
- Chance?
- What are the main study findings?
- How do you interpret the differences in outcomes after 6, 12, 18, and 24 months follow-up?
- How applicable is the study protocol to your practice? Are the study participants similar to your patients? What would be needed to make such an intervention practical in your setting?
- How could this study change your practice? Policy? Education? Research?
- If you designed a new lifestyle intervention for obese, sedentary adults in your own practice, how would it be structured and why? What evidence would you have to support its efficacy?
- What are the next steps in interpreting or applying these findings?
- What researchable questions remain?
References
- Stange KC, Miller WL, McLellan LA, et al. Annals Journal Club: It's time to get RADICAL. Ann Fam Med. 2006;4(3):196-197 http://annfammed.org/content/4/3/196.full.




{kind=link}
{kind=link}
{kind=link}