
Article Figures & Data
Figures
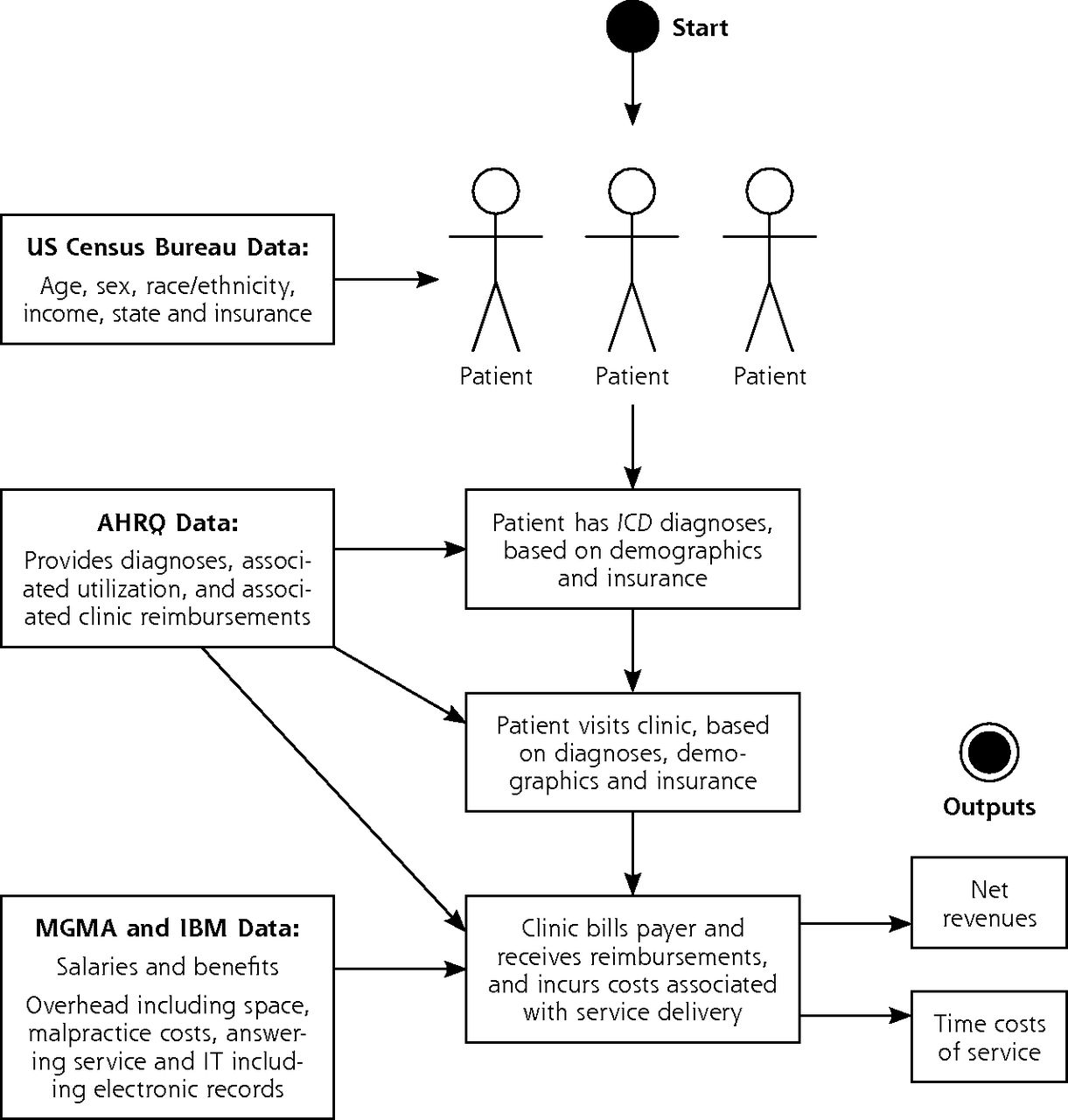
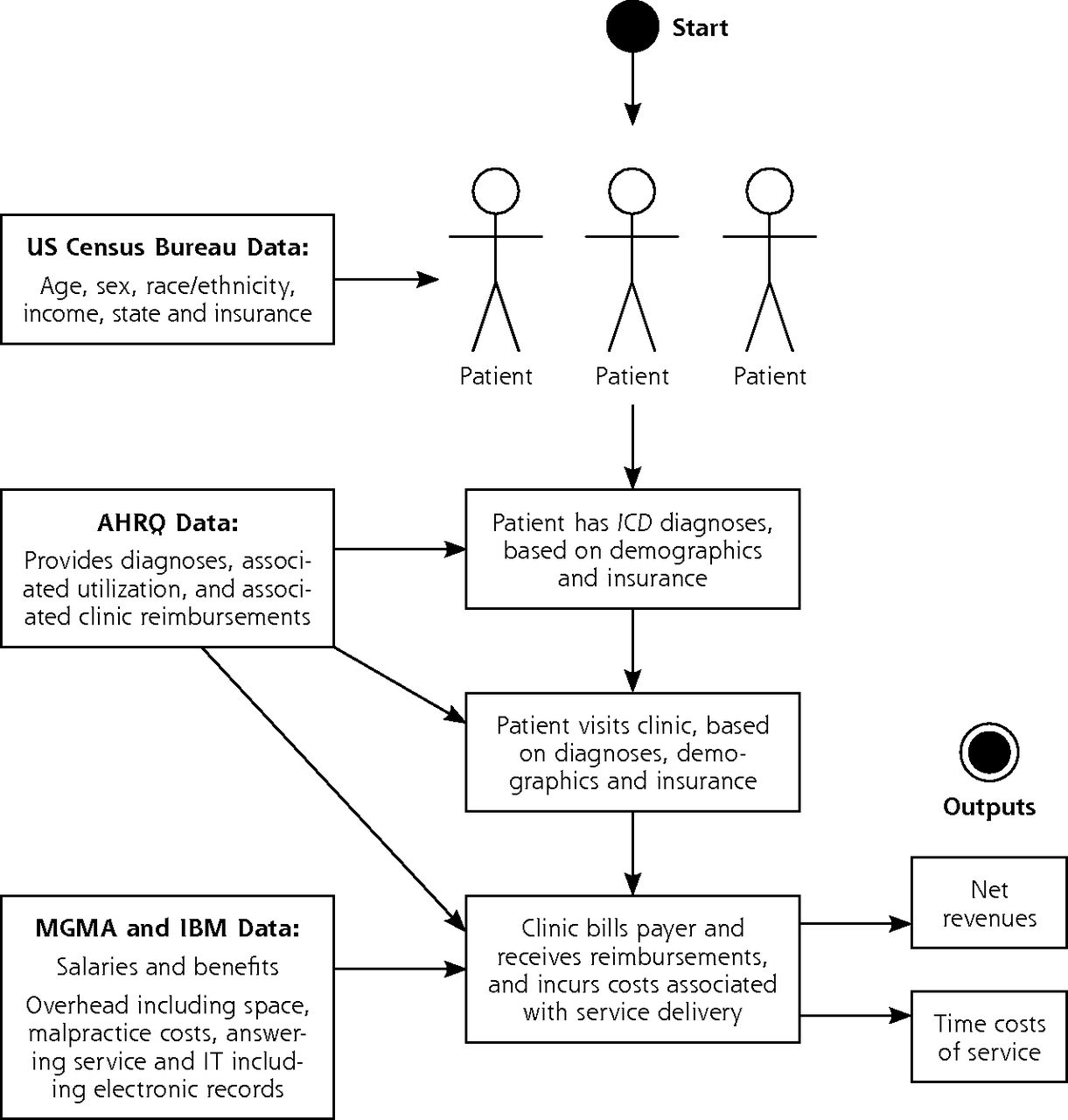
- Figure 1
Model flow diagram.
AHRQ = Agency for Healthcare Research and Quality; IBM = International Business Machines; ICD = International Classification of Diseases; IT = information technology; MGMA = Medical Group Management Association.
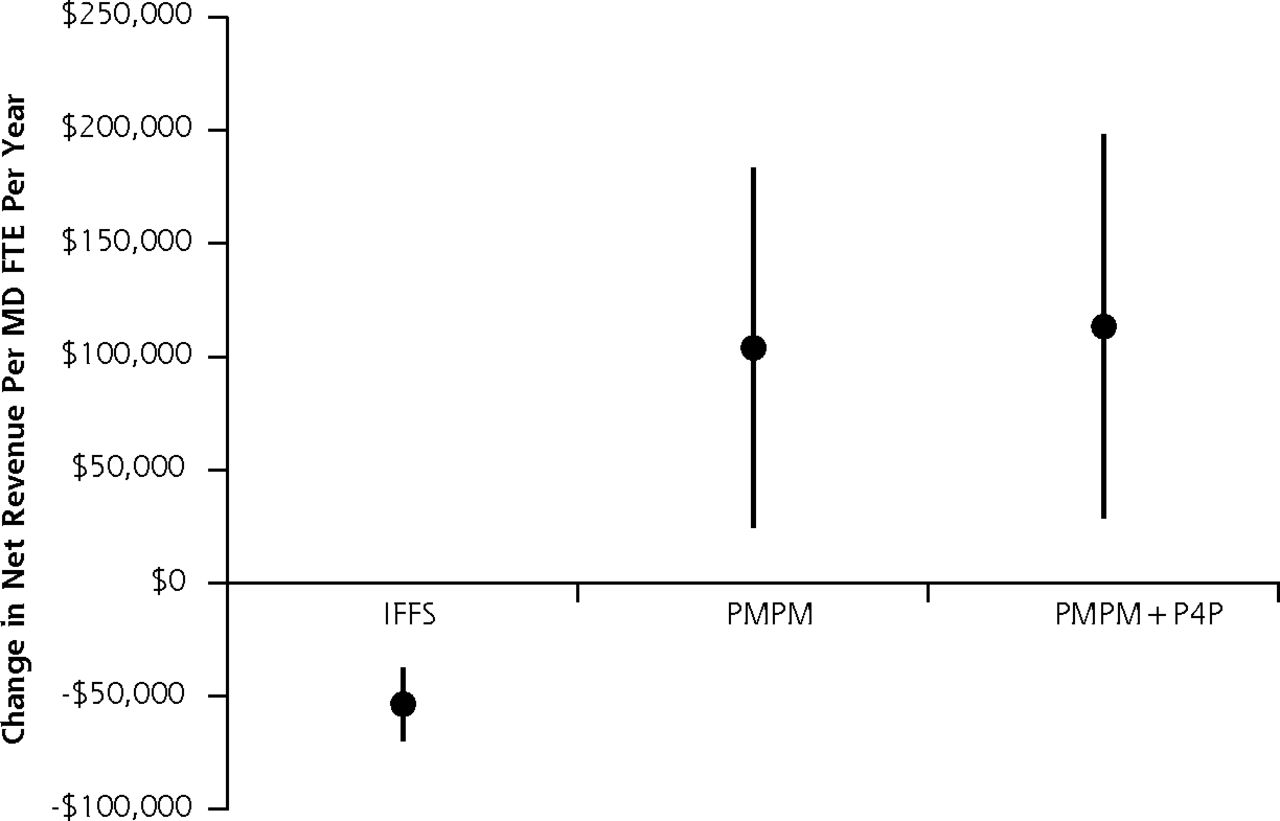
- Figure 2
Net revenue changes per full-time physician per year from clinics meeting minimum requirements to receive PCMH funding, as compared with the clinic operating under traditional fee-for-service payments.
IFFS = increased fee for service; P4P = pay for performance; PCMH = patient-centered medical home; PMPM = per-member-per-month.
Note: The PCMH funding approaches include IFFS rates, PMPM funding, and PMPM plus P4P bonuses (Table 1). The uncertainty ranges portrayed incorporate 3 sets of uncertainty through repeated sampling from the probability distributions of the input parameters: uncertainty in levels of utilization and associated revenue, cost to the practice including staff compensation and other practice costs, and payments through the new PCMH financing approaches (eg, level of payment increase from IFFS).
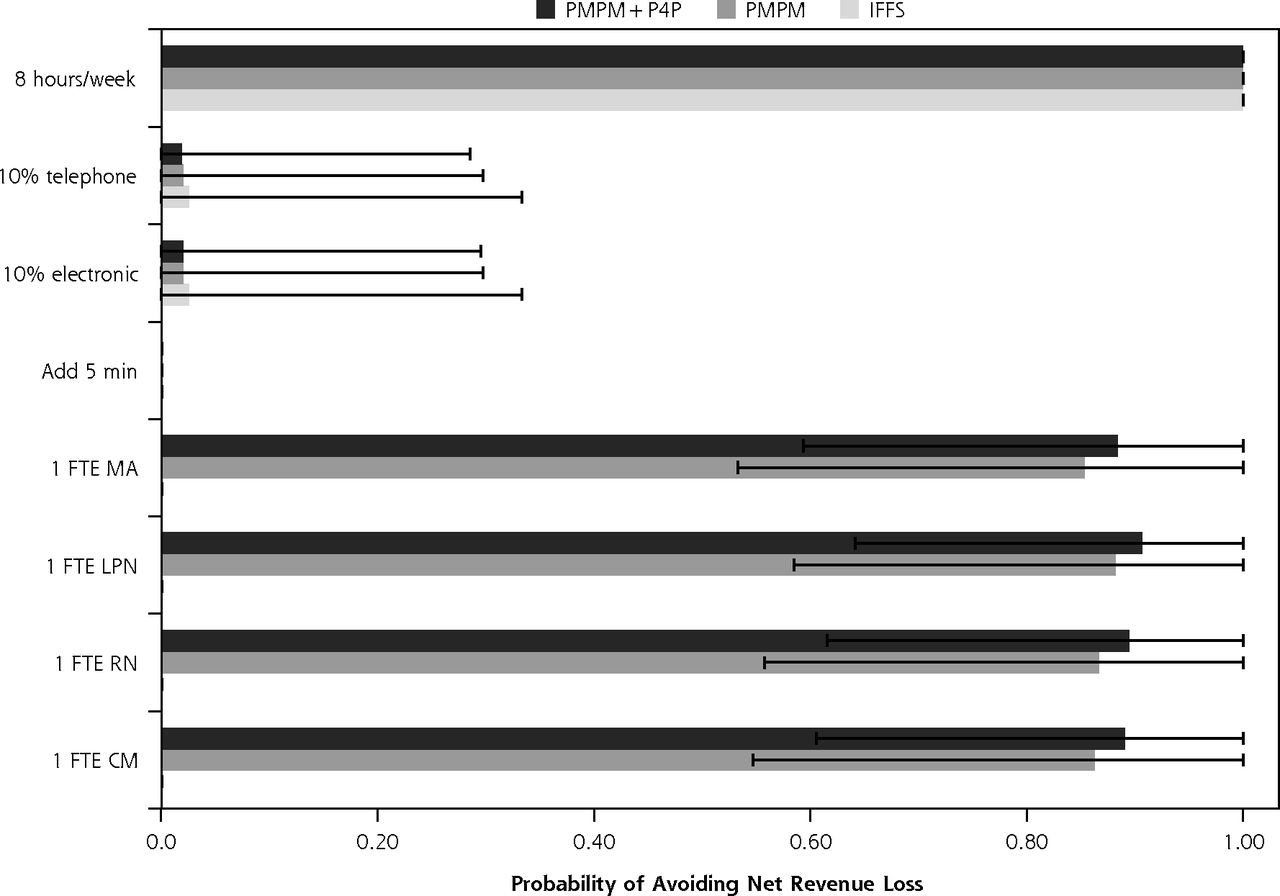
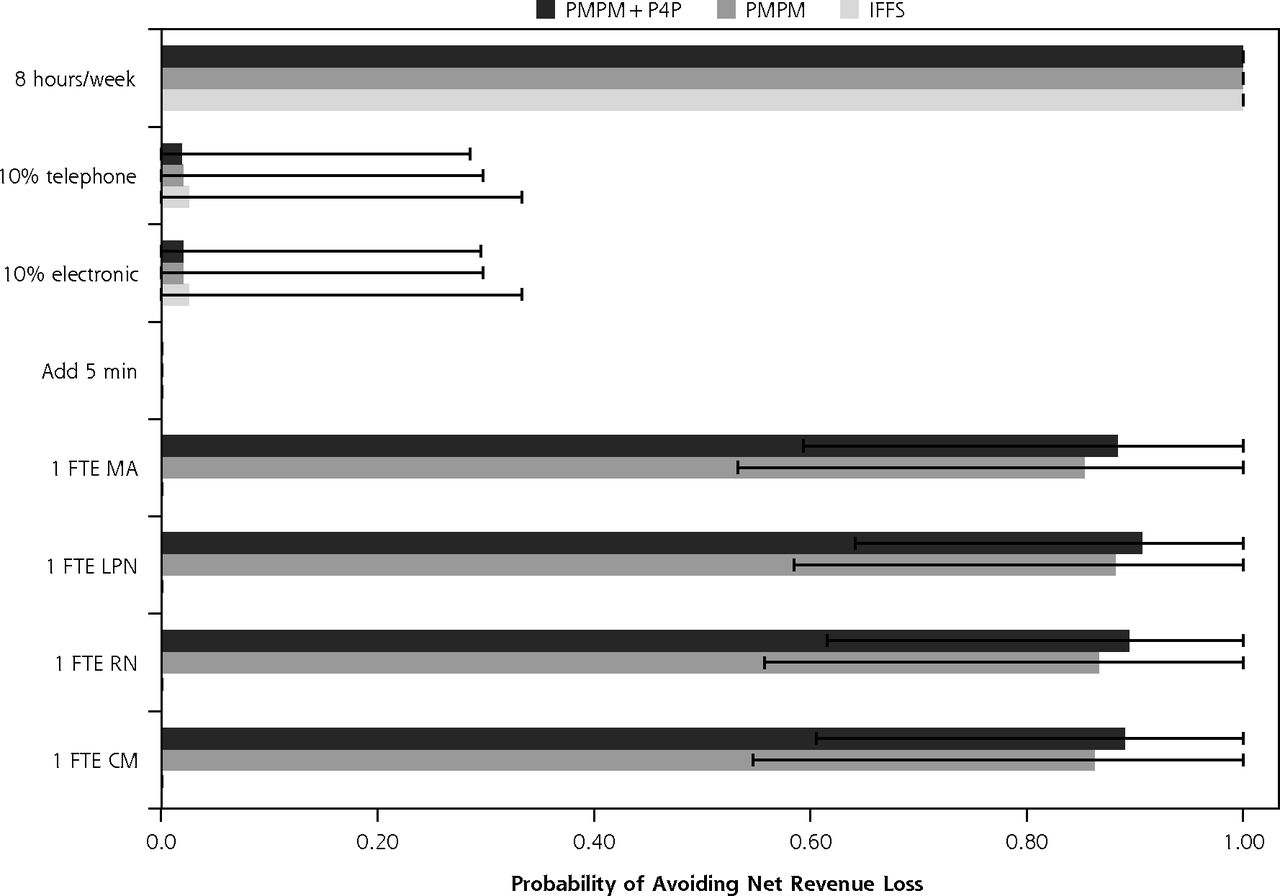
- Figure 3
Break even analysis, which identified the probability with which key medical home services could be supported by a clinic without achieving negative net revenue.
CC = care coordinator; FTE = full-time equivalent; IFFS = increased fee for service; LPN = licensed practical nurse; MA = medical assistant; P4P = pay for performance; PMPM = per member per month; RN = registered nurse.
Note: We specifically calculated the probability that a clinic would not lose net revenue through the addition of 1 FTE for each type of support staff (CC, RN, LPN, and MA); when adding 5 minutes to each visit; when converting 10% of routine visits to electronic or telephone visits; or when adding 1 full business day (8 evening/weekend business hours) per week in a median practice size of 5 FTE physicians.

Tables
Parameter Details Source Population demographics within each state population Age, y Cohorts of <5, 5–13, 14–17, 18–24, 25–44, 45–64, 65–84, and >84 y US Census Bureau24 Sex Cohorts of male or female Race/ethnicity Cohorts of non-Hispanic white, non-Hispanic black, Hispanic, and other Income Housing income relative to household size, expressed relative to federal poverty level Insurance status Cohorts of private, Medicare, Medicaid/CHIP, or self-pay Patient features Diagnoses among each demographic group International Classification of Disease, Ninth Revision Agency for Healthcare Research and Quality25 Per-person utilization of primary care clinics Visits per person per year, conditional on demographics, diagnoses, and state of residence Practice features Reimbursement for each primary care visit Specific to diagnoses and payer Agency for Healthcare Research and Quality25 Productivity of primary care physicians and midlevel clinicians Encounters and empanelment per clinician per year, by clinician type (physician, NP, PA) Medical Group Management Association26 Utilization changes associated with changes in staff Changes in encounters and empanelment given levels of support staffa Staffing ratios of midlevel clinicians and support staff per full-time physician Including NPs, PAs, RNs, LPNs, and MAs Overhead costs Including staff benefits, building and occupancy, information technology, drug and medical supply, equipment and administrative supplies, liability insurance and fees, laboratory and imaging fees, and other ancillary service costs Compensation costs for clinician Salary per full-time physician or midlevel clinician per year Bureau of Labor Statistics27 Compensation costs for support staff Salary per full-time worker per year, by worker type IBM Kenexa Compensation Analysis28 New financing approaches Increased FFS payment rates Median increase of 12% above current CPT codes (95% CI, 10%–14%)b CareFirst BlueCross BlueShield29 PMPM payment rates Median of $4.90 per empaneled patient per month (95% CI, $3.00–$8.00) Survey of patient-centered medical home initiatives4 P4P payment rates Median receipt rate of $2.63 per empaneled patient per annum (95% CI, $1.08–$4.17)c National Academy for State Health Policy1 Empanelment rate among new patient encounters (to charge new PMPM fees during panel expansion) Median of 53% of new encounters (95% CI, 42%–64%) who become additional panel members Medical Group Management Association26 Reimbursement codes for electronic and telephone visits 99444 for electronic, 99441 for telephone, varied by state and payer Center for Connected Health Policy30 Additional infrastructure costs for electronic visits $240 per year (95% CI, $0–$360) Telehealth Resource Center31 Encounter rate per extended business hour Regression model of utilization per extended hourd Agency for Healthcare Research and Quality25 CHIP = Children’s Health Insurance Program; CPT = Current Procedural Terminology; FFS = fee for service; IBM =International Business Machines; LPN = licensed practical nurse; MA = medical assistant; NP = nurse practitioner; PA = physician assistant; P4P = pay for performance; PMPM = per-member-per-month; RN = registered nurse.
Note: See Supplemental Appendix Tables 1 and 2 and Supplemental Appendix Figure 1 for full parameter values, http://www.annfammed.org/content/14/5/404/suppl/DC1.
↵a See the Supplemental Appendix Figure 1, http://www.annfammed.org/content/14/5/404/suppl/DC1.
↵b Confidence intervals are estimates of the distribution of input data, not the results of a model of population data estimates, and are used to construct normal probability distributions from which to perform repeated sampling in our probabilistic uncertainty analyses.
↵c Receipt rate incorporates the observed rate of performance target achievement, which we varied in sensitivity analyses from a baseline estimate of 10% to a lower and upper bound of 0% to 100%.32
↵d See the Supplemental Appendix, http://www.annfammed.org/content/14/5/404/suppl/DC1.
- Table 2
Model-Based Estimates of Changes in Net Revenue per Full-Time Physician for Primary Care Clinics Delivering PCMH Services Compared With the Net Revenue in the Traditional FFS Clinic Before PCMH Transformation
Change in Net Revenue ($/FTE physician/year) Traditional FFS $ (95% CI) Increased FFS $ (95% CI) PMPM $ (95% CI) PMPM plus P4P Bonuses $ (95% CI) Maximizing Net Revenues Under PCMH Payment Initiatives Minimum required changes for PCMH fundinga N/A −53,464
(−69,725 to −37,203)103,835
(24,462 to 183,208)113,343
(28,511 to 198,176)N/A Service delivery enhancements Optimize staff ratiob 46,722
(25,737 to 155,577)−53,464
(−69,725 to −37,203)103,835
(24,462 to 183,208)113,343
(28,511 to 198,176)FTEs: 0.23 CC, 0.31 RN, 0.53 LPN, 1.11 MA Extend visit length by 5 minc −119,092
(−170,874 to −83,002)−184,925
(−255,049 to −149,057)−62,771
(−156,974 to −57,134)−55,390
(−152,320 to −52,719)Not in optimal result Replace 10% of visits with electronic visitsd −16,175
(−17,134 to −15,165)−71,497
(−83,935 to −59,960)80,427
(11,394 to 145,836)89,610
(15,611 to 159,704)Not in optimal result Replace 10% of visits with telephone visitsd −16,151
(−17,107 to −15,144)−71,473
(−83,915 to −59,931)80,451
(11,413 to 145,868)89,634
(15,629 to 159,736)Not in optimal result Extend evening/weekend hourse 380 (373 to 386) −52,959
(−69,227 to −36,692)104,781
(25,402 to 184,160)114,321
(29,482 to 199,159)3.0–3.8 h/wk Net revenue-maximizing combinationf 47,101
(26,110 to 155,963)−52,959
(−69,227 to −36,692)104,781
(25,402 to 184,160)11,4321
(29,482 to 199,159)FTEs: 0.23 CC, 0.31 RN, 0.53 LPN, 1.11 MA + 3.0–3.8 h/wk evening/weekend service CC = care coordinator; FFS = fee for service; FTE = full-time equivalent; LPN = licensed practical nurse; MA = medical assistant; P4P = pay for performance; PCMH = patient-centered medical home; PMPM = per member per month; RN = registered nurse.
Note: Revenues include 4 funding scenarios: traditional FFS, increased FFS, PMPM, and PMPM plus P4P bonus. Confidence intervals in parentheses are from probabilistic sensitivity analyses in which the model was rerun 10,000 times while sampling from the probability distributions of all input parameters to generate confidence intervals around model results.
↵a Meets basic criteria of PCMH funding initiatives, cataloged previously,4 incorporating changes in communication, care management, external coordination, patient tracking, test/referral tracking, and quality improvement at an inflation-adjusted cost of $2.51 per patient per month (95% CI, $0.95–$4.57).35 Staffing ratios include a minimum of 0.23 FTE for a CC (0.21–0.25), 0.31 FTE for an RN (0.28–0.34), 0.53 FTE for an LPN (0.50–0.56), and 1.11 FTE for an MA per FTE physician (1.09–1.13).40 Probabilistic sensitivity and uncertainty analyses performed across the listed CIs through repeated sampling from corresponding normal distributions of minimum staffing levels to assess robustness of results. All costs expressed in 2015 US dollars.
↵b Adjusted support staff (CC, RN, LPN, and MA) levels per full-time physician, determined by repeated sampling from observed joint probability distributions linking staffing levels across clinicians and support staff to encounters and empanelment (Supplemental Appendix Figure 1, http://www.annfammed.org/content/14/5/404/suppl/DC1), then detecting which combinations of staffing levels maximized net revenue while still meeting the minimum PCMH funding requirements. Note that maximum net revenue was achieved by minimum staffing in all PCMH funding scenarios.
↵c Increasing visits by 5 minutes each from the baseline length at each simulated clinic.
↵d Simulated as replacing 10% of regular in-person encounters.
↵e Optimization involved finding the number of evening or weekend hours per week that would maximize net revenues for the clinic, calculating medical revenue from each additional business hour of providing service availability during nights and weekends via a midlevel practitioner, and subtracting the costs of compensation and overhead expenditure for those hours.
↵F Includes optimized clinic activities in all above-mentioned domains.
Supplemental Appendix, Tables, & Figures
Supplemental Appendix, Tables 1-13, and Figures 1-2
Files in this Data Supplement:
The Article in Brief
Effects of New Funding Models for Patient-Centered Medical Homes on Primary Care Practice Finances and Services: Results of a Micro-Simulation Model
Sanjay Basu , and colleagues
Background Given the tenuous financial sustainability of many primary care practices, the decision to make investments in the patient-centered medical home is influenced by financial outcomes as well as the benefits to patient care. With this in mind, researchers used a microsimulation model to test the effects of new payment strategies on patient-centered medical home practices' net annual revenue and service delivery.
What This Study Found Evaluating three different funding initiatives--increased fee-for-service payments, traditional fee-for-service with additional per-member-per-month payments and traditional fee-for-service with per-member-per-month and pay-for-performance payments--the study found that practices gained substantial additional revenue under per-member-per-month or per-member-per-month with pay-for-performance payments ($104,000 and $113,000 per full-time physician per year, respectively) but not under increased fee for service payments (-$53,500) after accounting for the costs of meeting PCMH funding requirements. Expanding services beyond minimum levels required for PCMH requirements decreased net revenue because of lost traditional fee-for-service revenues.
Implications
- The authors conclude that achieving goals of the PCMH will likely require more radical payment reforms, including more robust non-visit-based payment mechanisms specifically targeting funding toward the delivery of desired services.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Visit Entropy Associated with Diabetic Control Outcomes
- Shifting Implementation Science Theory to Empower Primary Care Practices
- Direct Primary Care: Applying Theory to Potential Changes in Delivery and Outcomes
- Finding a Parsimonious Path for Primary Care Practice Transformation
- High Levels Of Capitation Payments Needed To Shift Primary Care Toward Proactive Team And Nonvisit Care
- Costs of Transforming Established Primary Care Practices to Patient-Centered Medical Homes (PCMHs)
- Synthesis Of Research On Patient-Centered Medical Homes Brings Systematic Differences Into Relief
- In This Issue: Different Paths to Discovery
- Time to Do the Right Thing: End Fee-for-Service for Primary Care