
Article Figures & Data
Figures
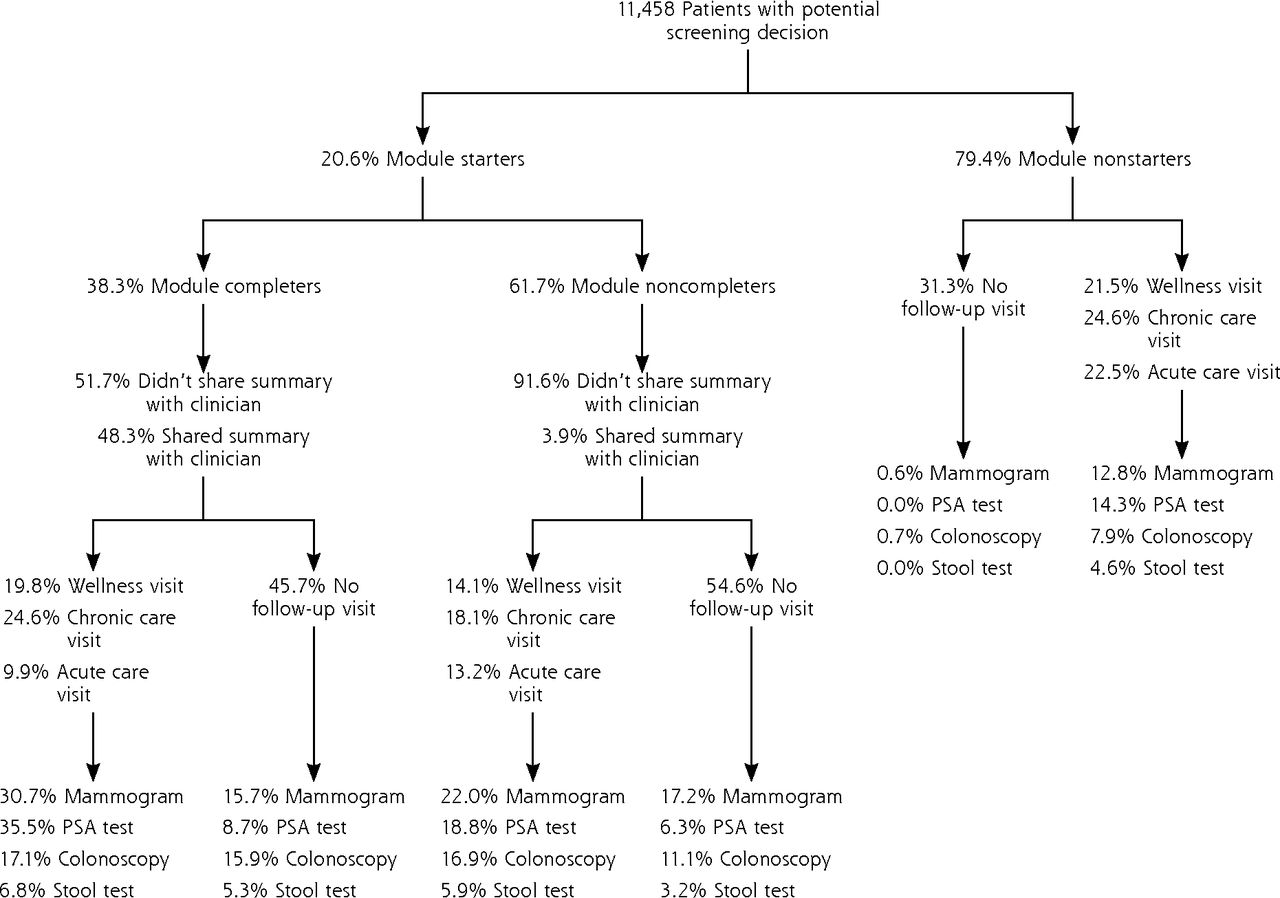
- Figure 1
Conceptual model for engaging patients through an informed decision-making module embedded in a patient portal and electronic health record.
Note: To engage patients in their decision, the informed decision-making (IDM) module guides patients and clinicians through a series of 7 steps that can be applied to a wide range of decisions beyond the test case (cancer screening) investigated in this study. The IDM module (1) reaches patients outside the confines of an office visit to explore a potential decision by completing the module; (2) walks patients through an intake that assesses personal preferences, knowledge, and needs, and patients’ readiness to make a decision; (3) provides personalized educational material tailored to patients’ stated preferences and decision stage; (4) allows patients to share their preferences and decision needs with their clinician; (5) prompts patients and clinicians to use the reported information to make a decision; (6) guides the patient to make a choice, which can include deferring the decision; and (7) invites patients and clinicians to provide input after the encounter.
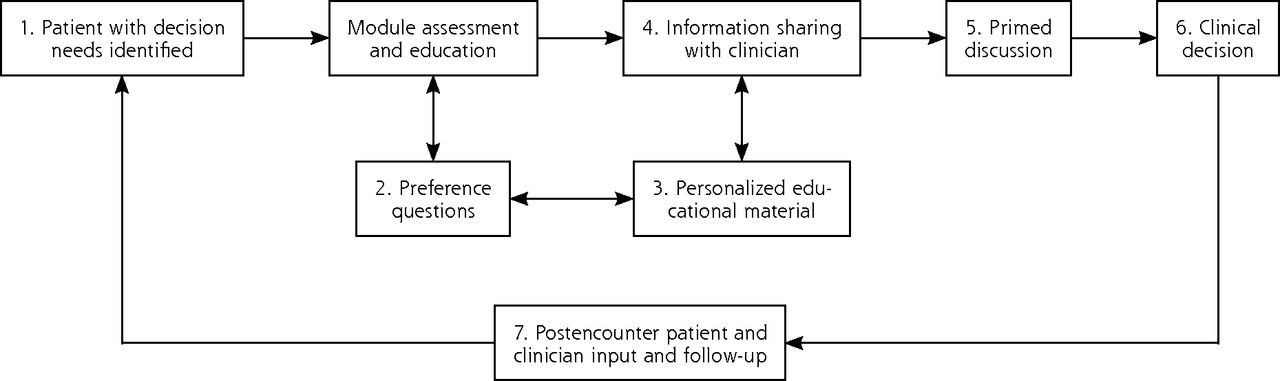
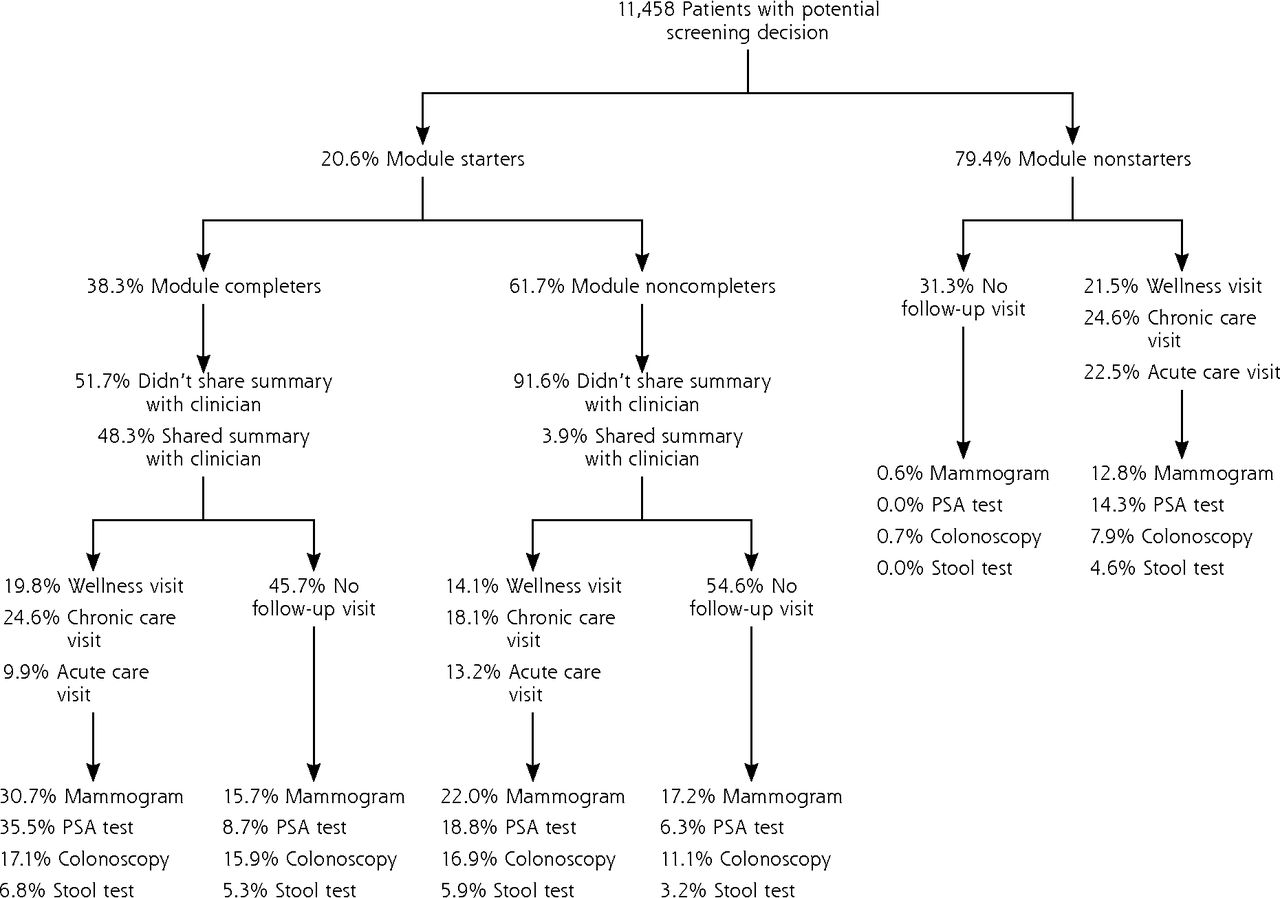
- Figure 2
Relationship of the informed decision-making module with follow-up visits and with breast, colorectal, and prostate cancer screening.
PSA = prostate-specific antigen.
Note: Percentages of patients who received screening tests were derived from electronic health record data for a period of 3 months after completion of the decision module. Although the colorectal cancer screening rate appears low, this study included only the subset of practice patients overdue for that screening. On the basis of prior studies and practice quality program participation, about 70% of patients in the study practices have been screened for colorectal cancer.46

Tables
- Table 1
Patients Starting and Completing the Informed Decision-Making Module by Study Phase and Cancer Screening Decision
Module Use Cancer Screening Decision Colon Breast Prostate Total Overall use: phases 1, 2, and 3 combineda Eligible, No. 6,329 3,733 1,396 11 ,458 Starters, No. (%) 1,249 (19.7) 638 (17.1) 468 (33.5) 2,355 (20.6) Completers, No. 489 190 224 903 Of starters, % 39.2 9.8 47.9 38.3 Of eligible, % 7.7 5.1 6.0 7.9 Phase 1: prompt on MyPreventiveCare log-ina Eligible, No. 542 297 171 1,010 Starters, No. (%) 154 (28.4) 70 (23.6) 86 (50.3) 310 (30.7) Completers, No. 39 12 21 72 Of starters, % 25.3 17.1 24.4 23.2 Of eligible, % 7.2 4.0 12.3 7.1 Phase 2: prompt via e-mail before appointmenta Eligible, No. 354 171 85 610 Starters, No. (%) 140 (39.5) 53 (31) 53 (62.4) 246 (40.3) Completers, No. 75 19 35 129 Of starters, % 53.6 35.9 66.0 52.4 Of eligible, % 21.2 11.1 41.2 21.1 Phase 3: prompt via e-mail without an appointmenta Eligible, No. 5,136 3,220 1,080 9,436 Starters, No. (%) 469 (9.1) 264 (8.2) 189 (17.5) 922 (9.8) Completers, No. 174 77 87 338 Of starters, % 37.1 29.2 46.0 36.7 Of eligible, % 3.4 2.4 8.1 3.6 ↵a Phases 1, 2, and 3 combined: January 2, 2014, through August 15, 2014. Phase 1: January 2, 2014, through February 16, 2014. Phase 2: February 17, 2014, through May 25, 2014. Phase 3: May 26, 2014, through August 15, 2014.
Note: The difference in starting and completing the decision module was statistically different for breast vs colorectal (P =.001), breast vs prostate (P <.001), and colorectal vs prostate cancer (P <.001) screening decisions. The difference in starting and completing the decision module was statistically different for phase 1 vs phase 2 (P <.001), phase 1 vs phase 3 (P <.001), and phase 2 vs phase 3 (P <.001).
Characteristic Module Starters Module Nonstarters Noncompleters Completers Age, mean (SD), y 53.5 (8.3) 54.9 (8.2) 52.4 (8.2) Total, No. (%) 1,452 (12.7) 903 (7.9) 9,103 (79.4) Sex Male 595 (13.9) 472 (11.1) 3,201 (75.0) Female 857 (11.9) 431 (6.0) 5,902 (82.1) Race, No. (%) Asian 132 (11.4) 60 (5.2) 966 (83.4) African American 62 (12.6) 63 (12.8) 368 (74.6) White 1,019 (13.7) 618 (8.3) 5,788 (78.0) Other 67 (11.7) 43 (7.5) 464 (80.8) Unreported 172 (9.5) 119 (6.6) 1,517 (83.9) Ethnicity, No. (%) Hispanic 43 (9.7) 38 (8.5) 364 (81.8) Non-Hispanic 1,065 (13.5) 658 (8.4) 6,153 (78.1) Unknown 344 (11.0) 207 (6.6) 2,586 (82.4) Language, No. (%) English 1,249 (13.3) 770 (8.2) 7,375 (78.5) Other 203 (9.8) 133 (6.5) 1,728 (83.7) Insurance type, No. (%) Commercial 1,304 (13.8) 782 (8.3) 7,349 (77.9) Medicare 92 (17.2) 69 (12.9) 374 (69.9) Medicaid 1 (20.0) 0 (0) 4 (80.0) None 55 (3.7) 52 (3.5) 1,376 (92.8) Prior screening, No. (%) Yes 538 (14.3) 347 (9.3) 2,861 (76.4) No 914 (11.9) 556 (7.2) 6,242 (80.9) Note: Given the large sample size, all differences across groups (noncompleters, completers, and nonstarters) were statistically significant (P <.001) with the exception of Medicaid insurance type.
Statement or Measure Patient Agreement, % (n = 277)a Clinician Agreement, % (n = 281)b Doctor believed to have seen response summary at time of appointment Yes 57.8 50.0 No 21.1 50.0 Cannot remember 21.1 0 Doctor discussed screening test at visit Yes 70.7 65.5 No 20.7 24.6 Cannot remember 8.6 9.9 How use of module changed the conversation Motivated patient to talk with doctor 39.0 41.3 Prompted doctor to talk with patient 28.1 39.7 Did not change anything 47.3 33.3 Other 2.1 9.5 How conversation helped patient with fears or worries ranked as most important on module Reduced fears or worries 80.9 NA Did not help with fears or worries 19.1 NA Doctor recalled addressing patients’ fears or worries about cancer screening Yes NA 39.0 No NA 29.3 Cannot remember NA 31.7 Strongly/somewhat agree vs strongly/somewhat disagree regarding completion of module and forwarding of summaryc Look and layout were easy to understand 56.0 vs 9.7 NA Took too long to complete 34.3 vs 29.2 NA Was easy to complete 72.2 vs 11.1 NA Helped patient with cancer screening decision 42.6 vs 20.4 44.9 vs 8.2 Made visit more productive 40.7 vs 17.6 38.1 vs 16.3 Got patient more involved with the decision 47.7 vs 17.6 51.7 vs 6.1 Helped to change patient’s screening plans 22.7 vs 30.1 13.6 vs 17.0 Improved patient-doctor communication 37.5 vs 16.7 42.2 vs 12.2 Improved patient’s knowledge before visit 48.1 vs 15.7 45.6 vs 6.1 Made the doctor more sensitive to patient’s needs 27.3 vs 11.6 48.3 vs 10.2
The Article in Brief
Harnessing Information Technology to Inform Patients Facing Routine Decisions: Cancer Screening as a Test Case
Alex H. Krist , and colleagues
Background In this study, researchers examine the potential of health information technology to systematically guide patients through decision making processes for three cancer screening choices. Specifically, the study evaluated how clinicians and patients used an automated decision module that promoted the 2012 prostate, 2009 breast and 2008 colon cancer screening recommendations made by the U.S. Preventive Services Task Force and how that module effected care.
What This Study Found Although automated decision aids have the potential to make office visits more efficient and effective, cultural, workflow and technical changes are needed before widespread implementation. Practices had a large decision burden -- with one in five patients facing a cancer screening decision over the one-year study period. Yet, of the 11,458 patients who faced a screening decision for colorectal cancer, breast cancer or prostate cancer, only 21 percent started and 8 percent completed the decision module. User data showed patients reviewed a range of topics while in the module and 47 percent of the module completers elected to forward a summary to their clinician. After their next office visit, both patients and clinicians reported that module completion helped with decisions: 41 percent said it made their appointment more productive, 48 percent said it helped engage them in the decision, 48 percent said it broadened their knowledge and 38 percent said it improved communication.
Implications
- The authors conclude that while the model is appealing, a clear challenge is getting patients to use such a system. If future research confirms the benefits of this approach -- yielding more informed patients, better decisions and wiser use of encounter time --the return on investment could offset the implementation costs and improve care.
Supplemental Appendixes
Supplemental Appendixes
Files in this Data Supplement:
- Supplemental data: Appendixes - PDF file




{kind=link}
{kind=link}