
Abstract
PURPOSE Self-harm is a public health problem that requires a better understanding of mortality risk. We undertook a study to examine premature mortality in a nationally representative cohort of primary care patients who had harmed themselves.
METHODS During 2001–2013, a total of 385 general practices in England contributed data to the Clinical Practice Research Datalink with linkage to Office for National Statistics mortality records. We identified 30,017 persons aged 15 to 64 years with a recorded episode of self-harm. We estimated the relative risks of all-cause and cause-specific natural and unnatural mortality using a comparison cohort of 600,258 individuals matched on age, sex, and general practice.
RESULTS We found an elevated risk of dying prematurely from any cause among the self-harm cohort, especially in the first year of follow-up (adjusted hazard ratio for that year, 3.6; 95% CI, 3.1–4.2). In particular, suicide risk was especially high during the first year (adjusted hazard ratio, 54.4; 95% CI, 34.3–86.3); although it declined sharply, it remained much higher than that in the comparison cohort. Large elevations of risk throughout the follow-up period were also observed for accidental, alcohol-related, and drug poisoning deaths. At 10 years of follow-up, cumulative incidence values were 6.5% (95% CI, 6.0%–7.1%) for all-cause mortality and 1.3% (95% CI, 1.2%–1.5%) for suicide.
CONCLUSIONS Primary care patients who have harmed themselves are at greatly increased risk of dying prematurely by natural and unnatural causes, and especially within a year of a first episode. These individuals visit clinicians at a relatively high frequency, which presents a clear opportunity for preventive action. Primary care patients with myriad comorbidities, including self-harming behavior, mental disorder, addictions, and physical illnesses, will require concerted, multipronged, multidisciplinary collaborative care approaches.
INTRODUCTION
Self-harm is a major public health problem. Deprived populations have a higher incidence of self-harm,1 and national incidence rates have risen in the wake of the economic downturn and subsequent austerity era.2 A greatly reduced life expectancy and an elevated risk of early death have been reported among people who seek care at hospitals after self-harm in Australia,3 Canada,4 Denmark,5 England,6 Finland,7 New Zealand,8 Norway,9 Sweden,10 and Taiwan.11 Very little is known, however, about the risk of death among primary care patients who have harmed themselves. A better understanding of mortality risk in this population is needed because national clinical guidelines in England, issued by the National Institute for Health and Clinical Excellence (NICE), have emphasized the important role of general practitioners and primary health care teams in managing and monitoring risk in these patients over both short-term12 and long-term13 follow-up. We have previously examined clinical management after a recent self-harm episode in the same primary care patient cohort.14 We found an unexpectedly low rate of referral to mental health services, and suboptimal levels of adherence to a specific NICE recommendation against prescribing of tricyclic antidepressant medication after self-harm,13,14 illustrating the clinical importance of examining premature mortality risk in this population.
For the study reported here, we used electronic health data linked to national mortality records to investigate the risk of dying prematurely after self-harm in a large primary care cohort in England. By examining deaths from both unnatural and natural causes, our intention was to highlight the potential clinical and public health benefits of addressing the physical health as well as the psychosocial needs of these patients. We currently know very little about long-term mortality risk in this population because researchers have traditionally tended to examine risk in the immediate post-harm period.4
METHODS
Data Source
The study was conducted using electronic health data extracted from the Clinical Practice Research Datalink (CPRD) obtained under license from the UK Medicines and Healthcare products Regulatory Agency.15 The CPRD is 1 of the world’s largest population-based, longitudinal, primary care databases containing anonymized patient information provided by general practices participating in the CPRD. In the UK National Health Service (NHS), more than 98% of the population is registered with general practitioners in practices providing health care free at the point of access. In December 2013, data were available for 684 general practices and more than 13 million patients with distributions of age and sex comparable to those reported in the UK national population census.15,16 Validation studies on the CPRD have demonstrated that it contains consistent, high-quality data.17 Diagnoses are coded using the Read system that is in standard use in UK general practice.18 An explanation of Read coding, and how diagnostic information is routinely recorded in the CPRD, is provided in Supplemental Appendix 1 (available at http://www.annfammed.org/content/15/3/246/suppl/DC1/).
Self-Harm Definition
We defined self-harm as “any act of self-poisoning or self-injury, irrespective of the apparent purpose,” from NICE clinical guideline number 16.12 Using this broad conceptualization, we developed a list of Read codes to identify all cases of self-harm across the spectrum from milder forms of nonsuicidal behavior to near-fatal suicide attempts. The Read code list is available online (https://clinicalcodes.rss.mhs.man.ac.uk/).19 Self-harm is a commonly used term in the United Kingdom, referring to all episodes irrespective of purpose; cases of attempted suicide with clear intent to die represent a subset among all persons who have harmed themselves. A detailed description of the psychiatric and comorbid physical illness diagnostic categories that we examined is given in Supplemental Appendix 2 (available at http://www.annfammed.org/content/15/3/246/suppl/DC1/).
Study Cohorts
The self-harm cohort consisted of a nationally representative sample of patients who had codes for an incident presentation of self-harm to primary care during 2001–2013 at ages 15 to 64 years. The rationale for imposing these age restrictions was that the determinants and implications of self-harm in children and older adults are distinct from those in the rest of the population, and therefore warrant separate consideration. Among older adults who harm themselves, specific mechanisms such as bereavement, loneliness, and social isolation,20,21 and physical illness, multimorbidity, and impairment21 play a greater role; children younger than 15 years who harm themselves may have less suicidal intent and a relatively low long-term risk of dying by suicide.22 Our intention was to preclude prevalent-cohort bias by delineating an incident cohort,23,24 and we therefore required patients to have been registered with a contributing practice for at least 1 full year before their index episode.
Each “exposed” self-harm patient was matched with up to 20 “unexposed” patients with no record of self-harm in the CPRD at the index episode date by sex, age (year of birth), and registered practice. We applied the same eligibility criteria for entry into both the self-harm cohort and the sampling frame for the matched comparison cohort.
Linked Mortality Data
We obtained linked cause-specific mortality records and examined the underlying cause of death coded at the Office for National Statistics (ONS) using the International Classification of Diseases 10th Revision (ICD-10).25 Death registration records were available for patients registered with 385 practices, approximately 60% of all CPRD practices, that is, those in England that participate in the CPRD scheme linking all patients with a valid NHS identifier. We examined both natural and unnatural causes, with the latter defined as “… external causes, e.g. injury or poisoning, which includes death due to intentional injury, such as homicide or suicide, and death caused by unintentional injury in an accidental manner.”26 Unnatural deaths were classified according to all codes listed in ICD-10 Chapter XX “External Causes of Morbidity and Mortality” (V01-Y98).25 As is accepted practice for UK-based epidemiologic research, our suicide definition included “open verdicts.”27 We examined natural causes because a significant proportion of people who harm themselves have a higher prevalence of lifestyle risk factors, including smoking28 and excessive drinking,29 that predict certain types of natural death, such as deaths from digestive diseases, respiratory diseases, and lung cancer. To examine alcohol-related deaths, which are mostly from natural causes but also include acute alcohol poisonings, we used a standard ONS-endorsed coding range,30,31 and likewise for classification of drug-poisoning deaths, which include all fatal poisonings or overdoses with prescribed medication, medication purchased legally over the counter, or illicit drugs.32 The ICD-10 classifications for alcohol-related death and drug poisoning death are shown in Box 1 of Supplemental Appendix 3 (available at http://www.annfammed.org/content/15/3/246/suppl/DC1/).
Area-Level Deprivation
On the basis of patients’ residential postcodes, we extracted Index of Multiple Deprivation (IMD) quintiles from the CPRD.33 The IMD measures area-level deprivation on the basis of several domains including income, employment, health, education, barriers to services (including housing), crime, and general living environment. It is derived for geographic areas designated as Lower-layer Super Output Areas (LSOAs)34 that contain 1,000 to 3,000 people and are Census derived. The IMD provides a means of ranking and assessing whether an area is more or less deprived than others.
Statistical Analyses
All analyses were performed using Stata software version 13 (StataCorp LP). For all individuals in a matched set, we defined the study entry point as the date of the index self-harm episode. We conducted Cox regression survival analysis35 stratified by matched set. We generated both unadjusted hazard ratios and those adjusted for the following potentially time dependent confounders: calendar year, frequency of contact with a general practitioner in past 12 months, mental illness diagnoses, psychotropic medication prescribed in past 12 months, clinically important alcohol misuse, and current smoking status. The methods used to generate these covariates are described in Supplemental Appendix 4 (available at http://www.annfammed.org/content/15/3/246/suppl/DC1/). Right-censoring was applied at the end of the study period, and also to account for migration from the database for reasons other than death, including geographic relocation or withdrawal of the patient’s practice from the CPRD, and death from causes other than the specific cause being examined.
RESULTS
Descriptive Analyses
Table 1 presents sociodemographic indices for the 30,017 persons in the self-harm cohort vs the 600,258 individuals in the matched comparison cohort on the date of the index episode. Because we matched patients on sex, age, and registered practice, the proportional breakdown in the table was identical for both groups with respect to sex, age, and practice-level deprivation. Female individuals, younger people, and those registered at practices in deprived localities were overrepresented.
Sociodemographic Characteristics at Index Self-Harm Episode
Table 2 compares clinical characteristics between the self-harm and comparison cohorts at baseline, indicating that they differed markedly in terms of their patterns of clinical consultation, with the former tending to visit their practice much more frequently. Additionally, the self-harm cohort had much higher prevalences of a psychiatric history, referral to mental health services, and psychotropic medication use; alcohol misuse, smoking, and physical illness comorbidity were also considerably more prevalent in this cohort.
Clinical Characteristics at Index Self-Harm Episode
Mortality Risk by Follow-up Year
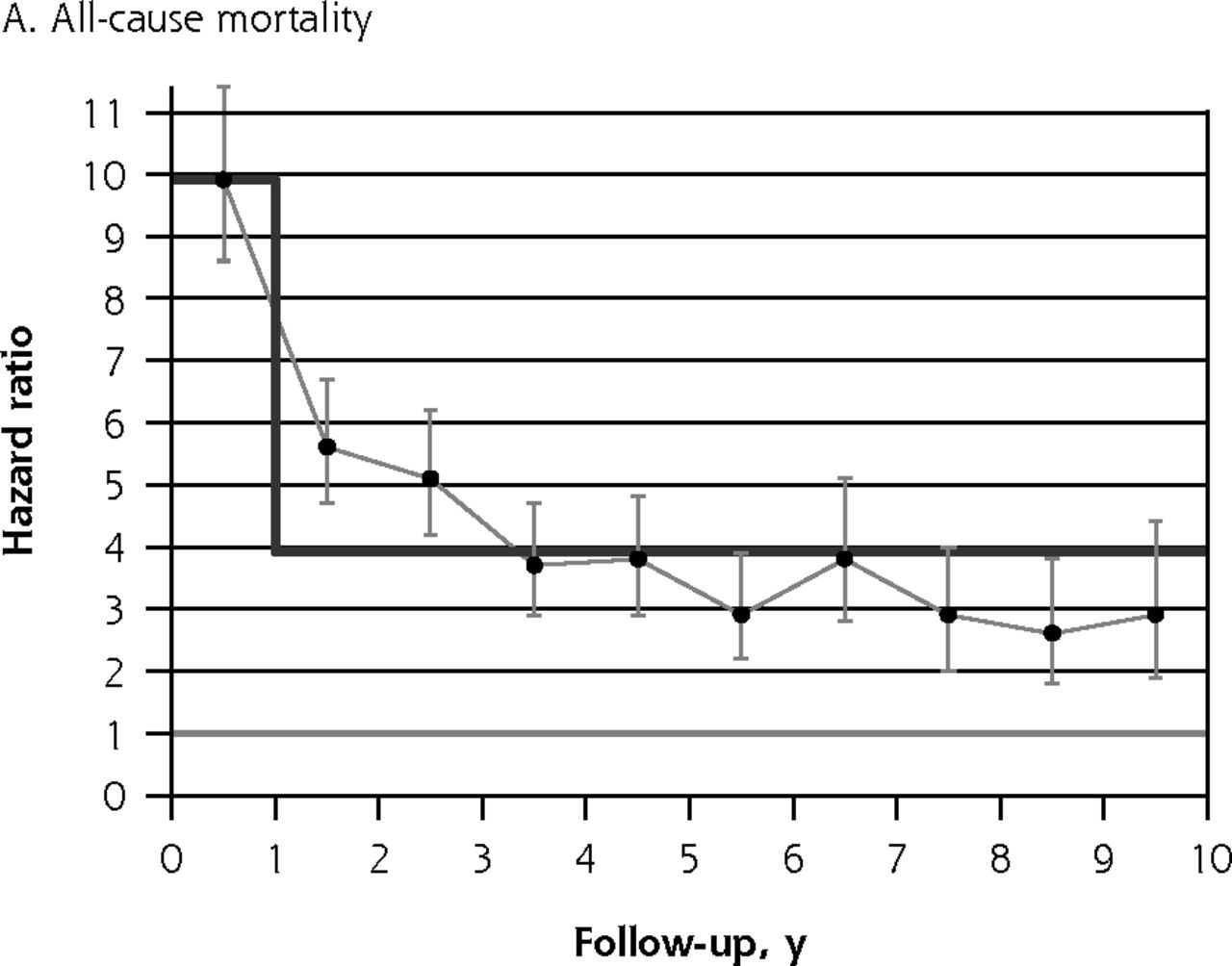
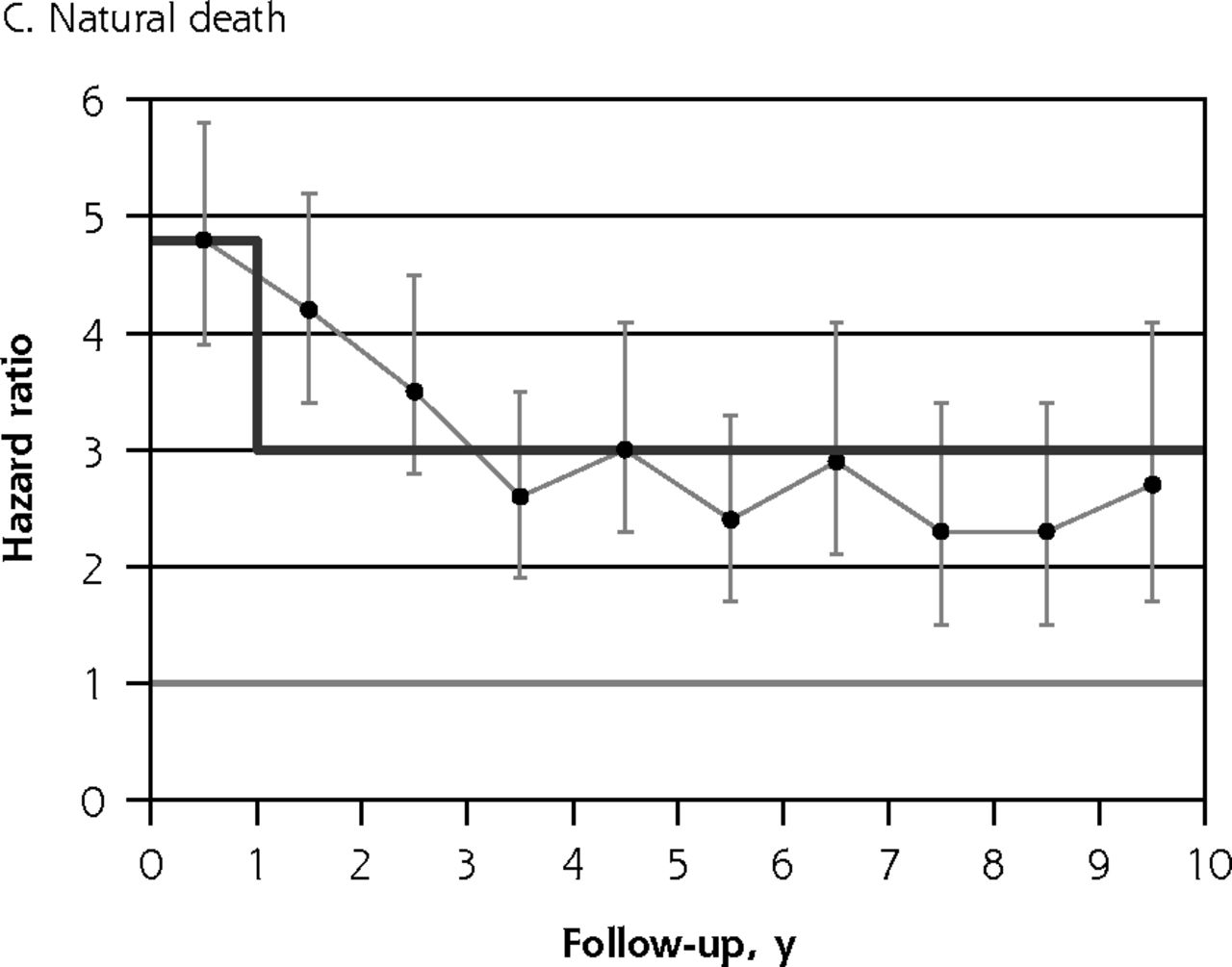
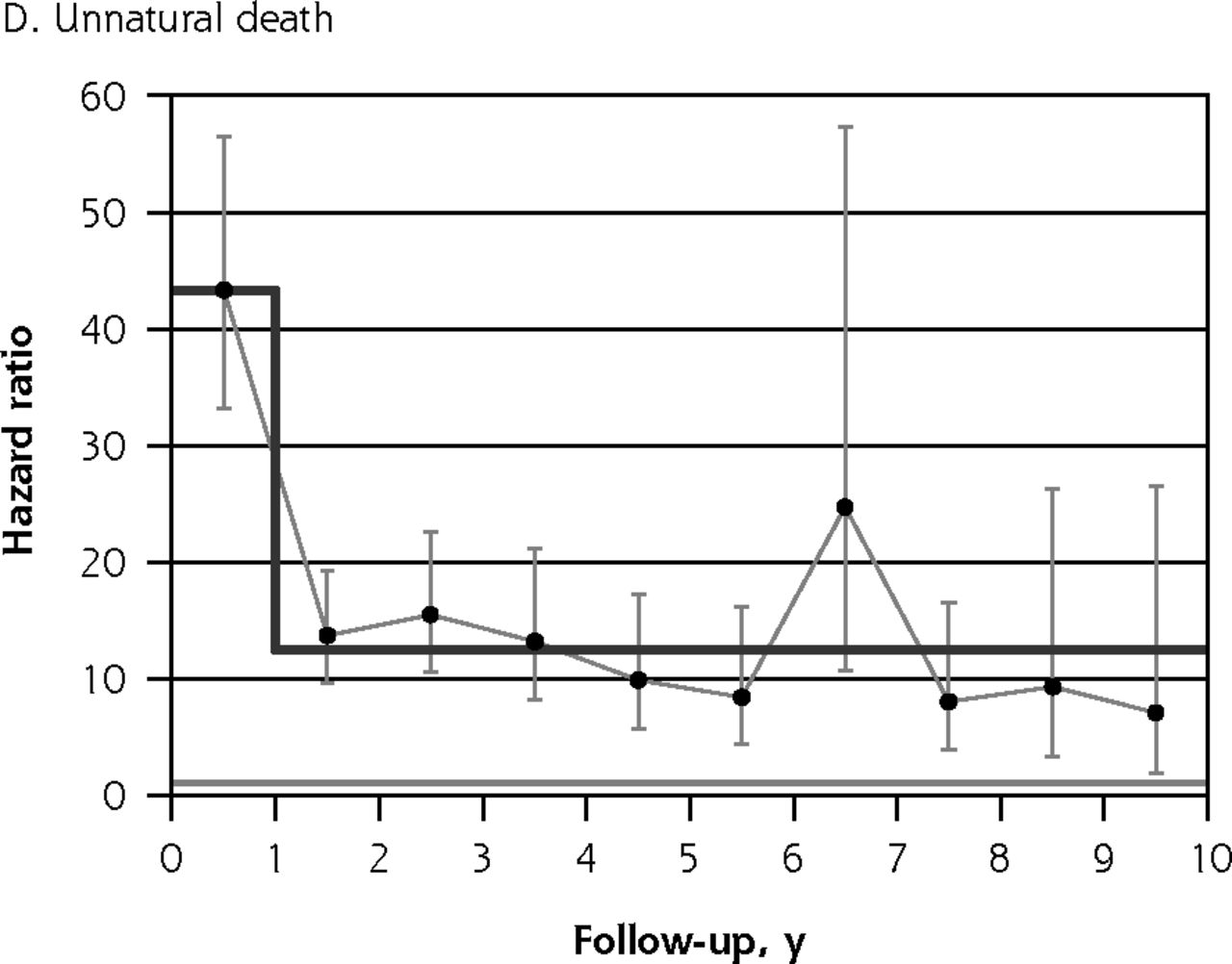
A key consideration when fitting a Cox model is the proportional hazards assumption,35 which requires the hazard ratio to be consistent throughout follow-up. Figure 1 shows plots of hazard ratios and their 95% CIs stratified by individual follow-up year. For all-cause mortality (Figure 1A), suicide (Figure 1B), natural death (Figure 1C), and unnatural death (Figure 1D), by far the greatest elevations in risk occurred during the first follow-up year. For natural death, the magnitude of the observed hazard ratio declined gradually in annual increments from the first to the fourth follow-up year, whereas for suicide and for all unnatural deaths combined, risk was markedly higher for the first year than it was during the ensuing 9 years of follow-up. Because mortality risk was found to be elevated to a greater degree during the first follow-up year than for subsequent years in all 4 of these plots, we accounted for nonproportionality in risk35 over time for all the hazard ratios presented in Tables 3 and 4. For these tabulations, we therefore estimated 2-stage hazard ratios separately, that is, for the first year of follow-up and for follow-up thereafter.



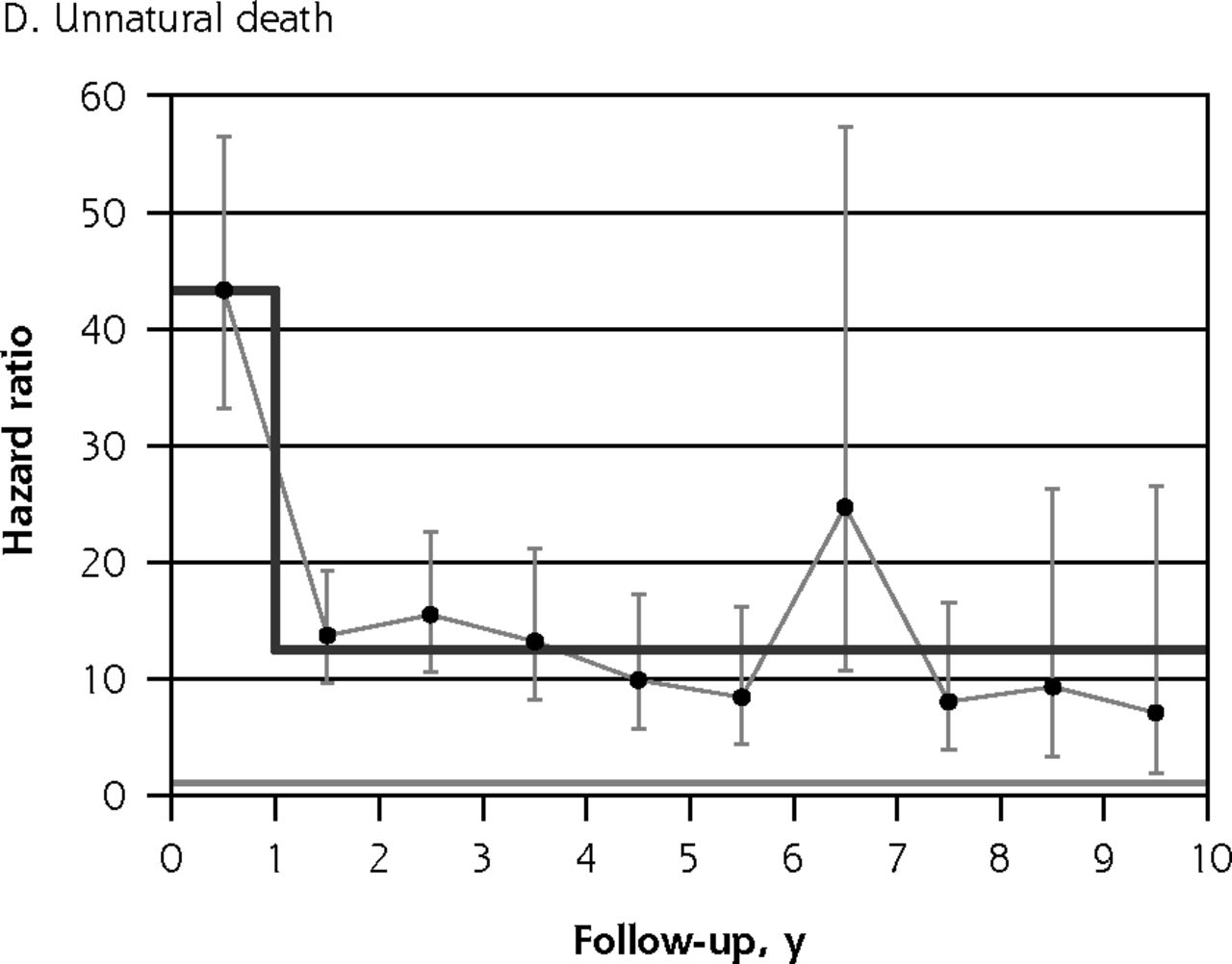
Hazard ratios for death due to various causes, stratified by individual follow-up year.
Notes: Hazard ratios for self-harm cohort vs comparison cohort. Note that y-axis scales differ. Dark gray line indicates modeled 2-stage trend. Light gray line indicates unity (1).
Hazard Ratios for Deaths Due to All Causes, All Natural Causes, and All Unnatural Causes
Hazard Ratios for Deaths Due to Specific Causes
Relative Risk of Early Mortality
Two-stage hazard ratio estimates for all-cause mortality, mortality from all natural causes, and mortality from all unnatural causes are presented in Table 3. We found 2 consistent patterns across these 3 broad mortality categories: (1) much greater risk during the first year vs subsequent follow-up years and (2) attenuated but still significant elevations in risk after covariate adjustment. Although a greater number of natural deaths were observed, the hazard ratios for unnatural death were considerably larger. Smaller effect sizes were observed for natural death, although even with this outcome, an independent statistically significant elevation in risk persisted after adjustment.
In Table 4 we present hazard ratios for the following specific causes of death: suicide, accidents, alcohol-related, drug poisoning, respiratory disease, and lung cancer. Self-harm was a strong and significant predictor for each of these outcomes, and the greatest risk elevations were for suicide. The increase in risk was more pronounced in the first year vs subsequent follow-up years, especially so for suicide. We did not observe any notable sex differences in the observed hazard ratios: likelihood ratio tests on sex interactions were not statistically significant for all causes of death (P = .09), all natural causes (P = .55), all unnatural causes (P = .18), and suicide (P = .14).
Cumulative Incidence of Premature Death
Absolute risks are shown in Table 5. The numbers of deaths are summarized at varying lengths of follow-up after the index self-harm episode for the self-harm and comparison cohorts along with cumulative incidence values (presented as percentages). At 10 years of follow-up, the cumulative incidence values in this predominantly younger cohort of people who had harmed themselves were 6.5% (95% CI, 6.0%–7.1%) for all-cause mortality and 1.3% (95% CI, 1.2%–1.5%) for suicide.
Cumulative Incidence of Deaths Due to All Causes and Specific Causes
DISCUSSION
Summary of Findings
Compared with a matched cohort of unaffected individuals, the self-harm cohort had a markedly increased risk of unnatural death during the first follow-up year. Beyond the first year, risk remained elevated vs the comparison cohort, but to a considerably lesser degree. The largest elevation in risk within a year of the index self-harm episode and over longer term follow-up was for suicide. Risk of dying prematurely from a natural cause was elevated for both follow-up periods, albeit to a much lesser degree than for dying by unnatural causes. Risks were increased across a broad array of cause-specific premature mortality outcomes, including suicide, accident, and alcohol-related, drug poisoning, respiratory disease, and lung cancer death.
Comparison With Existing Evidence
For the first time, we report short- and long-term mortality risk in UK primary care patients whose episodes of self-harming behavior may or may not be known to hospital services. Our findings also confirm those from earlier investigations that have reported an elevated risk of unnatural and natural mortality after self-harm.3–11,36–40 It is important, however, to highlight that almost all previously published studies ascertained index self-harm episodes via secondary care data sources, mostly through emergency department contacts, although a small number of study cohorts were drawn from specialized poisoning treatment centers.36 Virtually all previous studies have reported relative risks for cause-specific mortality without stratifying these estimates by length of follow-up. For some smaller studies, these estimates may have been aggregated across the whole observation period to maximize statistical power. Our proportional hazards assumption testing35 revealed that such data pooling may yield invalid estimates averaged across the whole duration of follow-up if the degree of risk elevation is substantially greater during the first year. Few investigations have reported relative risk restricted to the first follow-up year; 2 Taiwanese studies (1 conducted in Nantou County41 and the other in Taipei City11) found age- and sex-adjusted elevations of risk by 100-fold or more. The Multicentre Study of Self-harm in England, conducted in the cities of Derby, Manchester, and Oxford, reported on the shared characteristics and similarity of risk factors for suicide and accidental death after self-harm.41 It is therefore noteworthy that, in our study, risk of accidental death was also greatly elevated in the self-harm cohort.
Strengths and Limitations
Our study had several major strengths. For the first time, we examined risks of all-cause and cause-specific premature death in a nationally representative primary care cohort, with complete case ascertainment via linkage to national mortality records. We used an optimal study design by comparing risks directly at the individual patient level between an incident self-harm cohort and an unaffected comparison cohort sampled from the same population. This is a more robust approach than comparing risk indirectly via age- and sex-standardized mortality ratios calculated using nationally aggregated data, as was reported in previous studies.5 By delineating an incident cohort design, we precluded prevalent-cohort bias,23,24 which underestimates the strength of exposure-outcome associations, and which could have influenced previous investigations of this topic.3–11 Finally, our design was further enhanced by having up to 20 matched comparison individuals for every person in the self-harm cohort to enable examination of mortality outcomes that are particularly rare in the general population, such as suicide.
The study also had some limitations. First, we lacked the ability to examine confounding or effect modification by ethnicity and individual-level socioeconomic status (beyond a score allocated at the patient postcode level). Second, the mortality record linkage scheme implemented for most CPRD practices in England did not yet exist for CPRD practices in Scotland, Wales, or Northern Ireland when the study was conducted. Our findings may therefore not be generalizable to the entire UK population.
Interpretation and Implications
These findings should dispel any notion that a primary care patient cohort with a recorded history of self-harm would have an appreciably lower risk of dying prematurely by suicide and other unnatural and natural causes of death than individuals identified by hospital emergency department contacts. Our results suggest that secondary care study cohorts, which are the predominant setting for research conducted in the field, do not capture a population of higher-risk individuals compared with all registered primary care patients who have harmed themselves. From this information, we can infer a strong and clinically important message for primary health care teams: these patients have a greatly elevated risk of suicide and other causes of premature death, especially within a year of their known self-harm episode. National guidelines could provide more specific recommendations and training on how primary health care teams can intervene, manage, and monitor risk in these patients more effectively.42 Some of the risk factors identified, particularly alcohol misuse and smoking, are potentially modifiable. Furthermore, people who have harmed themselves visit clinicians much more frequently than their age- and sex-matched peers, which presents a clear opportunity for preventive action. Primary care patients with myriad comorbidities, including self-harming behavior, mental disorders, addictions, and physical illnesses, will require a concerted, multipronged, multidisciplinary collaborative approach to care to enhance management of their complex health needs.43
Acknowledgments
This study is based on data from the Clinical Practice Research Datalink (CPRD) obtained under license from the MHRA. The study was approved by the Independent Scientific Advisory Committee (ISAC) for CPRD-based research (Ref. 13_122ARA2). We would also like to acknowledge the contribution of our Patient and Public Involvement (PPI) partners, whom we liaised with from inception to completion of the study.
Footnotes
Conflicts of interest: Dr Kapur was Chair of the Guideline Development Group for NICE clinical guideline 133 (Self-Harm: Longer-Term Management, 2011), and was Chair of the NICE Self-harm, Quality Standard Topic Expert Group (2013). He is currently Chair of the Guideline Development Group for the NICE Depression in Adults guideline, and he sits on the National Suicide Prevention Advisory Group, England. The other authors report having no conflicts of interest.
Funding support: This work was supported by the Department of Health Policy Research Programme Suicide Prevention call (Self-harm in Primary Care Patients: A Nationally Representative Cohort Study Examining Patterns of Attendance, Treatment and Referral, and Risk of Self-harm Repetition, Suicide and Other Causes of Premature Death; RDD 023/0166). N.K. is funded in part by the Manchester Mental Health and Social Care Trust, and C.C.-G. is funded in part by the National Institute for Health Research (NIHR) Collaborations for Leadership in Applied Health Research and Care West Midlands. E.K.’s time and facilities were also supported by MRC Health eResearch Centre (HeRC) grant no. MR/K006665/1.
Disclaimer: The views expressed in this publication are those of the authors and not necessarily those of the Department of Health or the UK Medicines and Healthcare products Regulatory Agency (MHRA).
Supplementary materials: Available at http://www.AnnFamMed.org/content/15/3/246/suppl/DC1/.
- Received for publication September 16, 2016.
- Revision received December 16, 2016.
- Accepted for publication December 30, 2016.
- © 2017 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Risk factors, impact, and healthcare use related to initial suicide attempts: comprehensive analysis of Swedish population
- How GPs can help young people avoid future self-harm: a qualitative study
- Osteoporosis and fracture as risk factors for self-harm and suicide: a systematic review and meta-analysis
- Improving the management of self-harm in primary care
- Attitudes towards clinical and non-clinical services among individuals who self-harm or attempt suicide: A systematic review
- Assessing and predicting adolescent and early adulthood common mental disorders using electronic primary care data: analysis of a prospective cohort study (ALSPAC) in Southwest England
- 'Relieved to be seen--patient and carer experiences of psychosocial assessment in the emergency department following self-harm: qualitative analysis of 102 free-text survey responses
- Best practice when working with suicidal behaviour and self-harm in primary care: a qualitative exploration of young peoples perspectives
- In This Issue: Innovations in Primary Care and at the Annals