
Article Figures & Data
Figures
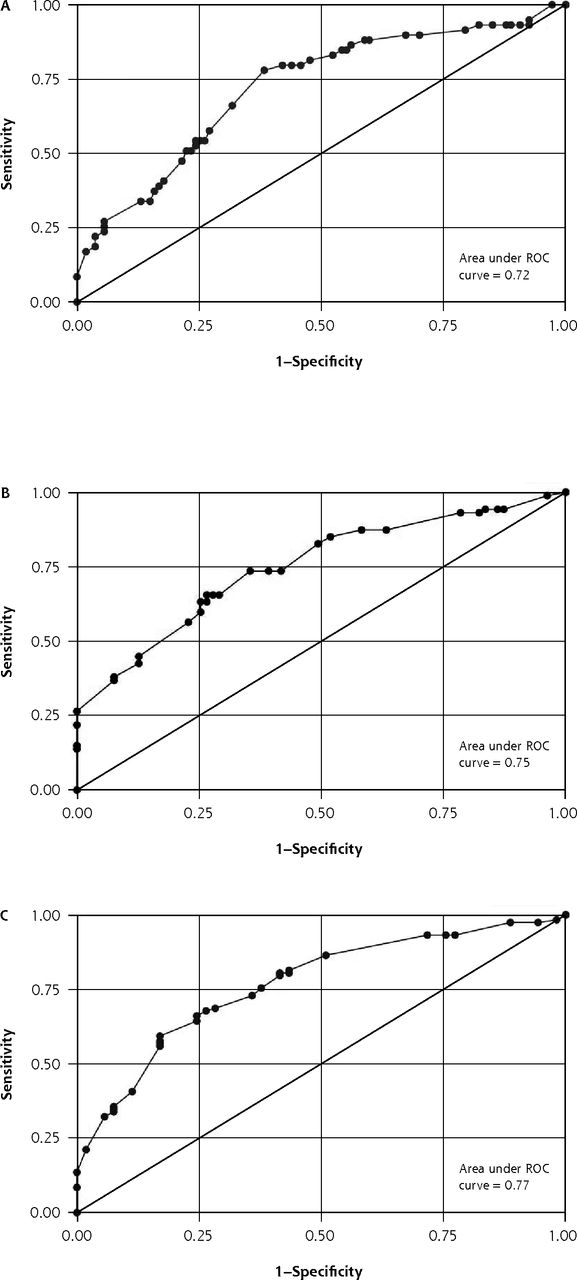
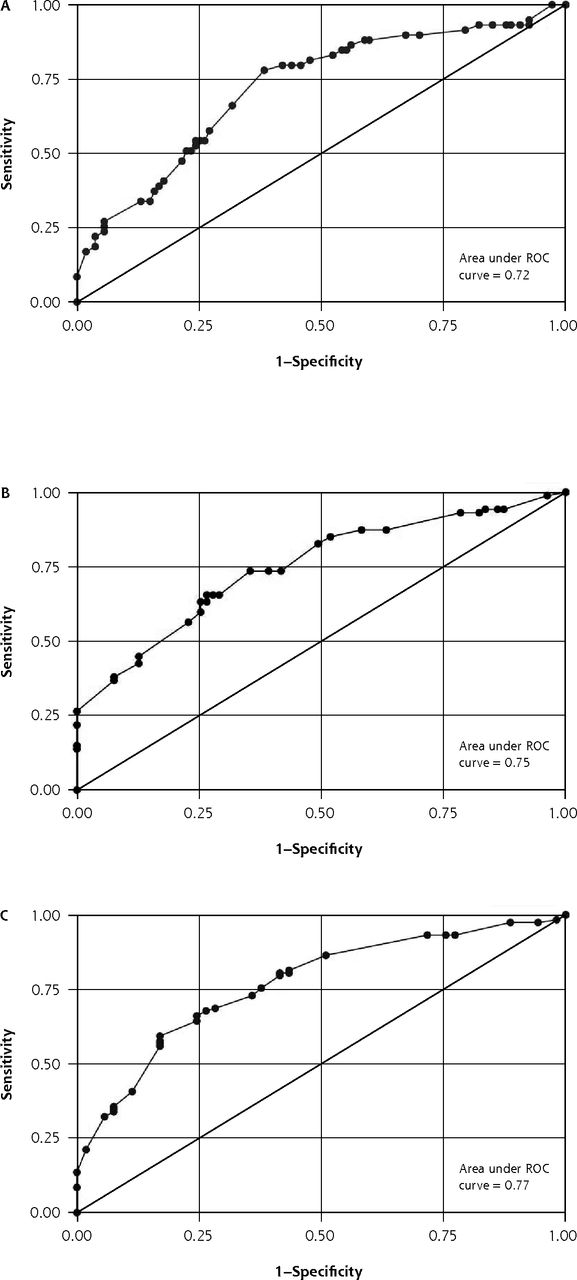
- Figure 1
Receiver operating characteristic (ROC) curves for logistic regression models using (A) abnormal bacterial culture, (B) abnormal finding on computed tomography, and (C) antral puncture revealing purulent fluid as reference standards.
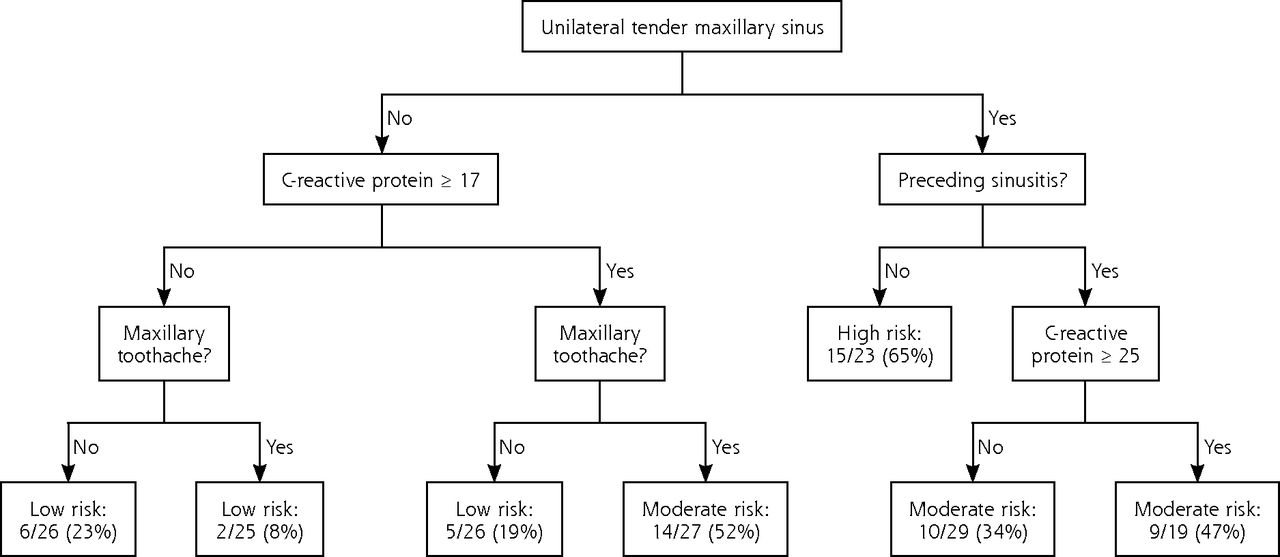
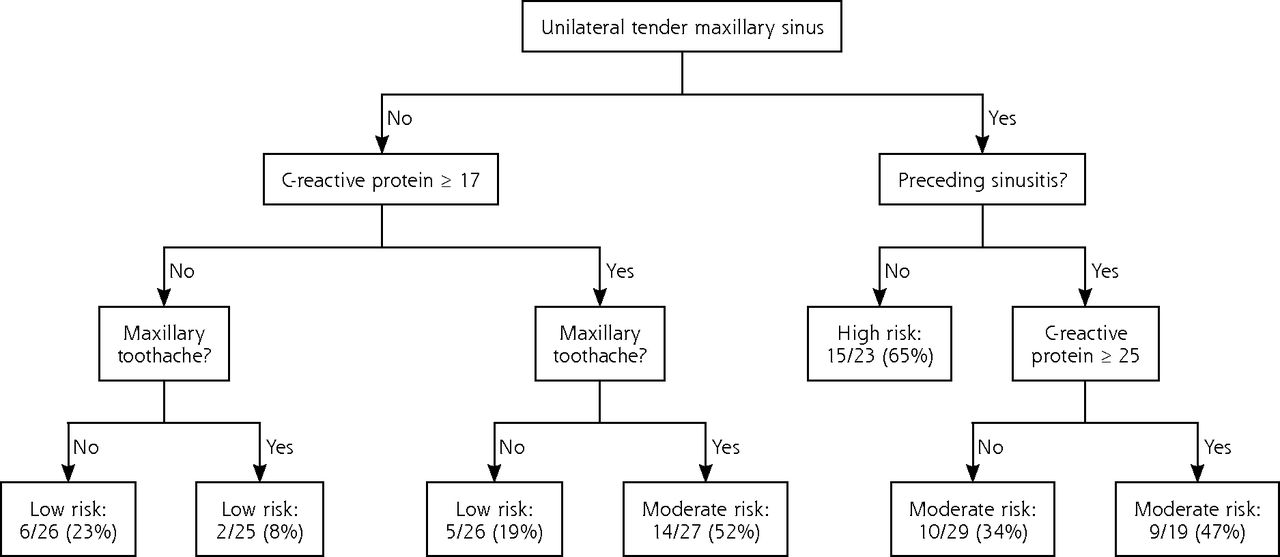
- Figure 2
Classification and regression tree model for positive bacterial culture as the reference standard.
Tables
- Table 1
Univariate Logistic Regression of the Association Between Signs, Symptoms, C-Reactive Protein (CRP), and Erythrocyte Sedimentation Rate (ESR) With Antral Puncture Revealing Purulent or Mucopurulent Fluid
Finding OR (95% CI) P Value Symptoms Preceding upper respiratory tract infectiona,b 2.09 (0.90–4.86) .088 Maxillary toothachea 1.99 (1.06–3.72) .031 Maxillary pain Any 0.42 (0.08–2.22) .307 Unilaterala,b 1.66 (0.91–3.03) .099 Bilateral 0.53 (0.29–0.97) .040 Cacosmia 1.37 (0.75–2.49) .309 Anosmiab 1.23 (0.67–2.27) .500 Cough 1.23 (0.66–2.30) .516 Nasal congestion 1.03 (0.50–2.14) .929 Pain bending forward 0.86 (0.43–1.73) .681 Previous diagnosis of sinusitis 0.43 (0.22–0.84) .014 Signs Purulent nasal dischargea,b 1.52 (0.77–2.99) .226 Tenderness of maxillary sinus Anya,b 1.93 (0.97–3.85) .063 Unilaterala,b 2.19 (0.18–4.08) .013 Bilateral 0.76 (0.40–1.43) .391 Tender tapping on teeth 1.30 (0.69–2.44) .415 Purulent pharyngeal discharge 1.30 (0.61–2.73) .497 Swollen inflamed turbinate 1.01 (0.54–1.91) .966 Edema over maxillary sinus Any 0.64 (0.34–1.20) .165 Unilateral 0.78 (0.39–1.57) .486 Bilateral 0.48 (0.15–1.49) .203 Laboratory tests C-reactive protein >10 mg/L 4.29 (2.27–8.11) <.001 >15 mg/La,b 4.75 (2.50–9.02) <.001 >20 mg/L 3.92 (2.02–7.61) <.001 Erythrocyte sedimentation rate >10 mm/h 3.30 (1.77–6.15) <.001 >20 mm/h 3.81 (1.92–7.53) <.001 OR=odds ratio.
Note: This analysis was also performed for abnormal CT finding and positive bacterial cultures as the reference standard; data available on request from the author.
↵a Included in initial models for abnormal finding on antral puncture and positive bacterial culture as the reference standard.
↵b Included in the initial model for abnormal computed tomographic finding as the reference standard.
- Table 2
Final Logistic Regression Models to Predict the Likelihood of Sinusitis as Defined by 3 Different Diagnostic Reference Standards
Independent Variable Abnormal CT Finding Antral Puncture Finding Positive Bacterial Culture β-Coefficient Score Point β-Coefficient Score Point β-Coefficient Score Point Preceding URTI 0.598 2 0.461 1 0.415 1 Preceding sinusitis −0.824 −2 −0.828 −2 −0.621 −1 Tender maxillary sinusitis (unilateral) 0.584 2 0.470 1 0.746 2 Maxillary toothache … … 0.636 1 0.741 2 Purulent nasal discharge … … … … 0.559 1 Anosmia 0.363 1 … … … … CRP >15 mg/L 1.602 4 1.467 3 0.754 2 Constant −0.277 … −1.087 … −1.936 … AUROCC 0.767 … 0.748 … 0.721 … Hosmer-Lemeshow χ2 test 4.74a … 10.88b … 8.22c … - Table 3
Accuracy of Point Scores Based on Logistic Regression Models for the Diagnosis of Acute Rhinosinusitis and Acute Bacterial Rhinosinusitis Using 3 Different Reference Standards
Reference Standard Score Points Sinusitis/Total No. (%) Likelihood Ratio Abnormal CT finding Low risk −2 to 1 17/43 (39.5) 0.29 Moderate risk 2 to 4 32/50 (64.0) 0.80 High risk 5 to 9 69/78 (88.5) 3.40 Total 118/171 (69.0) Classified as low or high risk 121/171 (70.8) Abnormal antral puncture finding Low risk −2 to 0 11/44 (25.0) 0.30 Moderate risk 1 to 4 53/99 (53.5) 1.10 High risk 5 to 6 23/23 (100.0) 42.00 Total 87/166 (52.4) Classified as low or high risk 67/166 (40.4) Positive bacterial culture Low risk −1 to 3 13/80 (16.3) 0.35 Moderate risk 4 to 6 35/71 (49.3) 1.80 High risk 7 to 8 11/15 (73.3) 5.00 Total 59/166 (35.5) Classified as low or high risk 95/166 (57.2) CT=computed tomography.
Note: Number with sinusitis and total are different from values for full data set, as cases with missing data were omitted.
- Table 4
Performance of CART Models for Outcomes of Abnormal CT Finding, Abnormal Antral Puncture Fluid Finding, and Abnormal Bacterial Culture
Reference Standard Sinusitis/Total No. (%) Likelihood Ratio Abnormal CT finding Low risk (−2 to 1) 13/42 (31) 0.20 Moderate risk (2 to 4) 42/60 (70) 1.07 High risk (5 to 9) 65/73 (89) 3.72 Total 120/175 (69) AUROCC 0.795 Classified as low or high risk 115/175 Abnormal antral puncture finding Low risk (−2 to 0) 13/56 (23) 0.28 Moderate risk (1 to 4) 36/67 (54) 1.07 High risk (5 to 6) 42/52 (81) 3.88 Total 91/175 (52) AUROCC 0.772 Classified as low or high risk 108/175 Positive bacterial culture Low risk (−1 to 3) 13/77 (17) 0.38 Moderate risk (4 to 6) 33/75 (44) 1.47 High risk (7 to 8) 15/23 (65) 3.50 Total 61/175 (35) AUROCC 0.731 Classified as low or high risk 100/175 AUROCC = area under the receiver operating characteristic curve; CART = classification and regression tree; CT = computed tomography.
Supplemental Appendixes and Figures
Supplemental Appendixes and Figures
Files in this Data Supplement:
- Supplemental data: Appendixes & Figures - PDF file
The Article in Brief
Proposed Clinical Decision Rules to Diagnose Acute Rhinosinusitis Among Adults in Primary Care
Mark H. Ebell , and colleagues
Background Practice guidelines only recommend the use of antibiotics in patients with prolonged, severe, or worsening symptoms of acute rhinosinusitis (ARS), when the likelihood of a bacterial cause is thought to be higher. However, it is common practice for patients diagnosed with acute rhinosinusitis to be prescribed an antibiotic regardless of the duration of symptoms or their severity. One strategy to reduce inappropriate prescribing is to give physicians tools that can help them more confidently diagnose or rule out acute bacterial rhinosinusitis (ABRS). This study set out to develop a clinical decision rule to diagnose acute rhinosinusitis and acute bacterial rhinosinusitis.
What This Study Found Researchers developed a series of clinical decision rules integrating signs, symptoms, and C-reactive protein that diagnose acute rhinosinusitis and acute bacterial rhinosinusitis with good accuracy. They developed a point score and algorithm for each of 3 reference standards: abnormal CT scan, abnormal antral puncture, or positive bacterial culture. They found that the most appropriate reference standard is positive bacterial culture of antral puncture fluid. The point score using this reference standard successfully identified groups with a low (16 percent), moderate (49 percent) and high (73 percent) likelihood of acute bacterial rhinosinusitis.
Implications
- By identifying patients at low risk for a bacterial infection, this clinical decision rule can lead to more conservative use of antibiotics and help reduce inappropriate antibiotic prescribing.
- According to the authors, prospective validation of the findings and an assessment of their effect on clinical and process outcomes are important next steps.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Diagnostic prediction models for CT-confirmed and bacterial rhinosinusitis in primary care: individual participant data meta-analysis
- Identifying adults with acute rhinosinusitis in primary care that benefit most from antibiotics: protocol of an individual patient data meta-analysis using multivariable risk prediction modelling
- Accuracy of signs, symptoms and blood tests for diagnosing acute bacterial rhinosinusitis and CT-confirmed acute rhinosinusitis in adults: protocol of an individual patient data meta-analysis
- Clinical gestalt to diagnose pneumonia, sinusitis, and pharyngitis: a meta-analysis
- Accuracy of Signs and Symptoms for the Diagnosis of Acute Rhinosinusitis and Acute Bacterial Rhinosinusitis
- C-reactive protein: guiding antibiotic prescribing decisions at the point of care
- In This Issue: Trends, Prescribing, Deprescribing