
Article Figures & Data
Figures
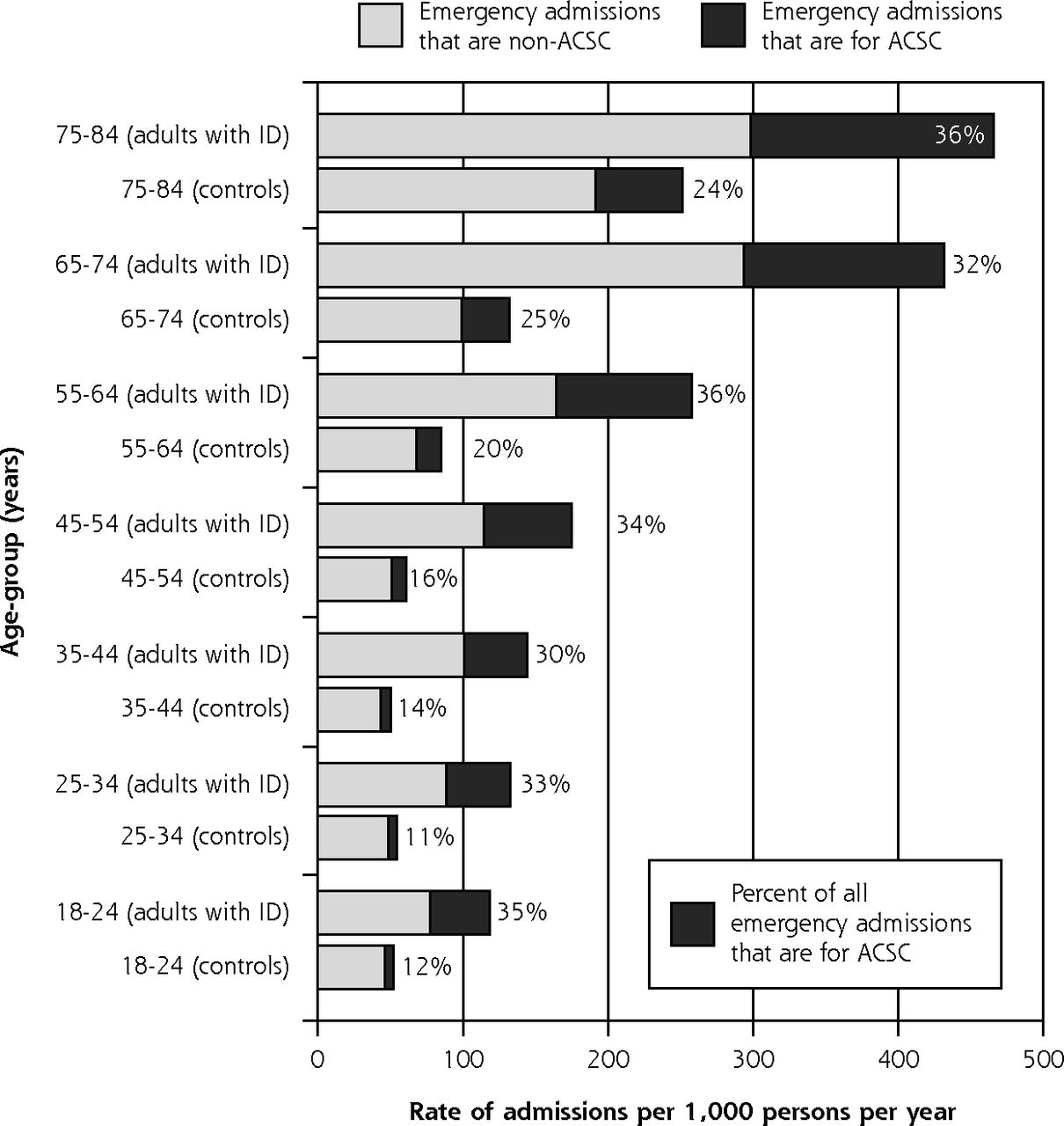
- Figure 1
Emergency admissions, overall and for ACSCs by age-group in adults with intellectual disability and controls, 2009–2013.
ACSC=ambulatory care–sensitive condition; ID=intellectual disability.
Tables
Characteristic Adults With ID Adults Without IDa Unadjusted Modelb Adjusted Modelc Adults, No. Admissions, No. Admission Rated Admission Rated IRR (95% CI) P Valuee IRR (95% CI) P Valuee All adults 16,666 9,026 182.2 67.7 2.82 (2.66–2.98) – 2.16 (2.02–2.30) – Stratified by matching factor Sex Female 6,989 4,250 203.8 73.5 2.90 (2.66–3.15) – 2.09 (1.89–2.30) – Male 9,677 4,776 166.5 63.4 2.75 (2.55–2.96) .36 2.20 (2.01–2.41) .45 Age-group at baseline, y 18–34 6,981 2,374 125.3 50.5 2.54 (2.31–2.80) – 1.81 (1.61–2.04) – 35–54 6,283 3,201 159.3 55.6 2.96 (2.69–3.25) .03 2.10 (1.87–2.37) .09 55–84 3,402 3,451 328.7 116.7 2.90 (2.63–3.19) .06 2.43 (2.19–2.70) <.001 Stratified by characteristic of adults with ID Down syndrome Yes 1,793 804 150.0 62.9 2.61 (2.23–3.05) – 2.37 (1.97–2.84) – No 14,873 8,222 186.1 68.2 2.84 (2.68–3.01) .31 2.11 (1.96–2.26) .27 Communal accommodation Yes 3,392 2,141 205.7 75.0 2.91 (2.63–3.22) – 2.15 (1.88–2.47) – No 13,274 6,885 175.9 65.7 2.79 (2.61–2.98) .50 2.16 (2.00–2.33) .95 High level of support needsf Yes 3,263 2,487 243.9 70.2 3.67 (3.32–4.05) – 3.83 (3.42–4.28) – No 13,403 6,539 166.2 67.1 2.59 (2.42–2.77) <.001 2.32 (2.16–2.49) <.001 ID=intellectual disability; IRR=incidence rate ratio.
↵a Matched on age, sex, and practice.
↵b IRR from conditional Poisson model for patients with vs without ID. Matched on age, sex, and practice only.
↵c Additionally adjusted for comorbidities (atrial fibrillation, cancer, chronic obstructive pulmonary disease, dementia, diabetes, epilepsy, heart failure, severe mental illness, stroke), Index of Multiple Deprivation quintile, and smoking—for all subgroups except for the subgroup with high support needs, among whom epilepsy was not used in the adjustment.
↵d Admissions per 1,000 adults per year.
↵e P values test for difference in IRR between subgroups (for age, 18–34 years is the comparator group).
↵f Had been classified as having severe or profound ID by general practitioner or had 2 or more of the following: epilepsy, cerebral palsy or considerable mobility problem (wheelchair use or greater impairment), severe visual impairment, severe hearing impairment, a continence problem, or use of percutaneous endoscopic gastrostomy feeding.
ACSC Adults With ID Adults Without IDa IRR (95% CI) Admissions, No. Admissions, Rateb Admissions, No. Admissions, Rateb Angina 47 1.0 329 1.0 1.00 (0.60–1.68) Aspiration 152 3.1 25 0.07 85.9 (45.3–162.9) Asthma 91 1.8 233 0.7 2.84 (1.99–4.06) Cellulitis 156 3.1 331 1.0 3.31 (2.56–4.28) Chronic obstructive pulmonary disease 105 2.1 454 1.3 1.68 (1.04–2.70) Congestive heart failure 44 0.9 156 0.5 2.21 (1.44–3.38) Constipation 128 2.6 142 0.4 6.79 (5.17–8.91) Convulsions/epilepsy 1,081 21.8 256 0.8 31.2 (24.6–39.5) Dehydration and gastroenteritis 141 2.9 224 0.7 4.71 (3.60–6.17) Dental conditions 22 0.4 52 0.2 2.80 (1.67–4.71) Diabetes complications 61 1.2 140 0.4 3.26 (1.90–5.58) Ear, nose, and throat 28 0.6 132 0.4 1.42 (0.93–2.17) Gangrene 1 0.02 10 0.03 – Gastroesophageal reflux disease 22 0.4 74 0.2 2.22 (1.35–3.67) Hypertension 3 0.06 32 0.1 – Influenza 8 0.2 18 0.05 – Iron-deficiency anemia 21 0.4 40 0.1 3.97 (2.18–7.20) Nutritional deficiencies 0 0 2 0.01 – Pelvic inflammatory disease 5 0.1 26 0.08 – Perforated/bleeding ulcer 10 0.2 20 0.06 3.78 (1.63–8.75) Pneumonia and other lower respiratory tract infections 566 11.4 772 2.3 5.59 (4.85–6.45) Tuberculosis and other vaccine-preventable conditions 1 0.02 11 0.03 – Urinary tract infections 345 7.0 528 1.5 4.76 (3.99–5.68) Total 3,038 61.3 4,007 11.7 5.62 (5.14–6.13) ACSC = ambulatory care–sensitive condition; ID = intellectual disability; IRR = incidence rate ratio.
Note: Estimates for gangrene, hypertension, influenza, nutritional deficiencies, pelvic inflammatory disease, and tuberculosis and other vaccine-preventable diseases were not generated because of insufficient number of admissions.
↵a Matched on age, sex, and practice.
↵b Admissions per 1,000 adults per year.
Characteristic Adults With ID Adults Without IDa Unadjusted Modelb Adjusted Modelc Adults, No. Admissions, No. Admission Rated Admission Rated IRR (95% CI) P Valuec IRR (95% CI) P Valuec All adults 16,666 3,038 61.3 11.7 5.62 (5.14–6.13) – 3.60 (3.25–3.99) – Stratified by matching factor Sex Female 6,989 1,428 68.5 13.1 5.68 (5.03–6.42) – 3.35 (2.87–3.91) – Male 9,677 1,610 56.1 10.7 5.56 (4.91–6.30) .81 3.89 (3.39–4.46) .16 Age-group at baseline, y 18–34 6,981 805 42.5 6.2 7.12 (5.96–8.51) – 3.06 (2.47–3.79) – 35–54 6,283 1,041 51.8 8.6 6.34 (5.43–7.39) .34 3.25 (2.74–3.87) .67 55–84 3,402 1,192 113.5 26.2 4.56 (4.00–5.20) <.001 4.09 (3.52–4.76) .03 Stratified by characteristic of adults with ID Down syndrome Yes 1,793 392 73.1 9.3 10.00 (7.54–13.28) – 8.28 (5.73–11.98) – No 14,873 2,646 59.9 12.0 5.26 (4.79–5.77) .001 3.21 (2.88–3.58) .002 Communal accommodation Yes 3,392 915 87.9 14.0 6.86 (5.78–8.14) – 4.98 (4.01–6.20) – No 13,274 2,123 54.2 11.1 5.20 (4.70–5.76) .01 3.35 (2.98–3.77) .006 High level of support needsf Yes 3,263 1,154 113.2 12.1 10.31 (8.81–12.07) – 11.78 (9.78–14.19) – No 13,403 1,884 47.9 11.6 4.40 (3.95–4.90) <.001 4.28 (3.80–4.81) <.001 ACSC = ambulatory care–sensitive condition; ID = intellectual disability; IRR = incidence rate ratio.
↵a Matched on age, sex, and practice.
↵b IRR from conditional Poisson model for patients with vs without ID. Matched on age, sex, and practice only.
↵c Additionally adjusted for comorbidities (atrial fibrillation, cancer, chronic obstructive pulmonary disease, dementia, diabetes, epilepsy, heart failure, severe mental illness, stroke), Index of Multiple Deprivation quintile, and smoking—for all subgroups except for the subgroup with high support needs, among whom epilepsy was not used in the adjustment.
↵d Admissions per 1,000 adults per year.
e P values test for difference in IRR between subgroups (for age, 18–34 years is the comparator group).
↵f Had been classified as having severe or profound ID by general practitioner or had 2 or more of the following: epilepsy, cerebral palsy or considerable mobility problem (wheelchair use or greater impairment), severe visual impairment, severe hearing impairment, a continence problem, or use of percutaneous endoscopic gastrostomy feeding.
- Table 4
Comparison of Health Care Use in the 2 Weeks Before Emergency Admission for UTI and for LRTI or Pneumonia, Between Adults With and Without ID
Characteristic UTI LRTI or Pneumonia Adults With ID, No. (%)
(n=276)Adults Without ID, No. (%)
(n=451)Adults With ID, No. (%)
(n=457)Adults Without ID, No. (%)
(n=671)Age-group, ya 18–34 43 (16) 123 (27) 84 (18) 81 (12) 35–54 77 (28) 115 (26) 145 (32) 194 (29) 55–84 156 (57) 213 (47) 228 (50) 396 (59) Sex, male 134 (49) 150 (33) 260 (57) 384 (57) At high risk for infectionb 139 (50) 117 (26) 108 (24) 23 (3) Health care use Consulted primary care practice 156 (56) 251 (56) 277 (61) 368 (55) Did not consult but had emergency encounterc 19 (7) 32 (7) 27 (6) 39 (6) Had other record of encounter onlyd 70 (25) 85 (19) 97 (21) 131 (20) Did not have any record of use 31 (11) 83 (18) 56 (12) 133 (20) Among those who consulted the practice only Diagnosis recorded 22 (14) 45 (18) 60 (22) 80 (22) Urine test performede 44 (28) 75 (30) NA NA Antibiotics prescribed 62 (40) 115 (46) 111 (40) 163 (44) None of the above 76 (49) 118 (47) 151 (55) 187 (51) Among those prescribed antibiotics only Frontline antibioticf only 29 (47) 57 (50) 65 (59) 113 (69) Other antibiotic only 28 (45) 52 (45) 32 (29) 34 (21) Both frontlinef and other antibiotic 5 (8) 6 (5) 14 (13) 16 (10) Antibiotics prescribed, No. 1 55 (89) 94 (82) 88 (79) 130 (80) ≥2 7 (11) 21 (18) 23 (21) 33 (20) ID = intellectual disability; LRTI = lower respiratory tract infection; NA = not applicable for LRTI or pneumonia; UTI = urinary tract infection.
↵a Mean age was 54.8, 51.6, 52.2, and 56.5 years across the row, respectively.
↵b High risk for UTI: history of specific kidney operation, UTI, catheter, or incontinence; high risk for LRTI or pneumonia: history of recurrent chest infections, pneumonitis, percutaneous endoscopic gastrostomy feeding, prescriptions for food thickeners, or ≥2 chest infections in past year.
↵c Included emergency department and other out-of-hours services.
↵d Other records were repeat prescriptions, administrative entries, or routine specialist appointments.
↵e Urine tests included both immediate dipstick and nonimmediate urine microscopy; of those with a test recorded, 37 (84%) of adults with ID and 62 (83%) of adults without ID had urine microscopy.
↵f Frontline antibiotics were nitrofurantoin and trimethoprim for UTI, and amoxicillin, clarithromycin, doxycycline, and erythromycin for pneumonia or LRTI.
The Article in Brief
Preventable Emergency Hospital Admissions Among Adults With Intellectual Disability in England
Iain M. Carey , and colleagues
Background Avoiding acute hospitalization is important for people with intellectual disabilities, who tend to have poorer health than people in the general population. This study describes overall and preventable emergency admissions for adults with intellectual disabilities and assesses differences in primary care management of two common preventable (ambulatory care sensitive) conditions: lower respiratory and urinary tract infections.
What This Study Found Adults with intellectual disabilities have more than twice as many emergency hospital admissions and five times more preventable emergency admissions than other comparable individuals. Researchers linked primary care records with hospital admission data among 16,666 adults with intellectual disabilities and 113,562 age-, sex- and practice-matched controls without intellectual disabilities from England�s general population. In adults with intellectual disabilities, 3,847 (23 percent) had an emergency admission and 1,809 (11 percent) had multiple admissions. In comparison, 12 percent of those in the control group had one or more emergency hospitalizations and 4 percent had multiple admissions. The overall annual rate for emergency hospitalizations in adults with intellectual disabilities was 182 per 1,000 adults, nearly three times higher than their matched controls and more than double the control group when adjusted for comorbidities, smoking and deprivation. The most common ambulatory care sensitive conditions resulting in admission for adults with intellectual disabilities were convulsions/epilepsy (36 percent), lower respiratory tract infection (19 percent) and urinary tract infection (11 percent).
Implications
- This study, the first in the United Kingdom to use an unselected group of adults with intellectual disabilities to accurately quantify differences in emergency admissions, lays the foundation for health interventions for adults with such disabilities, particularly as their life expectancy increases. Higher emergency admission rates represent an area where improvements can be made, the authors suggest.
Supplemental Appendix
Supplemental Appendix
Files in this Data Supplement:
- Supplemental data: Appendix - PDF file
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Admission avoidance in UK healthcare: What works and what doesnt? A hermeneutic review
- Hospitalisations and deaths due to Ambulatory Care Sensitive Conditions (ACSC) among adults with and without Intellectual Disabilities in Scotland
- A qualitative exploration to inform an oral health training for disability care workers in Burkina Faso
- Predictors of specialist somatic healthcare utilization among older people with intellectual disability and their age-peers in the general population: a national register study
- Recording of intellectual disability in general hospitals 2006-2019: cohort study using linked datasets
- Use of health services in the last year of life and cause of death in people with intellectual disability: a retrospective matched cohort study
- In This Issue: Tools to Help Focus on What is Valuable