
Abstract
To ascertain changes in shared decision making (SDM), we analyzed data from the nationally representative Medical Expenditure Panel Survey. We aggregated responses to questions into a 7-point SDM composite score. Between 2002 and 2014, the mean SDM composite score increased from 4.4 to 5.0 (P <.01), indicating greater patient-perceived SDM. In multivariate modeling, SDM scores were higher for black vs white patients (+0.33 points) and those with a same-race/ethnicity usual source of care (+0.24 points; both P <.05). Scores were lower for patients with poor-perceived health (−0.41 points), Asian vs white race/ethnicity (−0.28 points), and no insurance (−0.17 points; all P <.05). Improvement efforts should target Americans without a same-race/ethnicity usual source of care and with poor-perceived health.
- shared decision making
- patient-centered care
- clinical decision-making
- decision support techniques
- primary care
INTRODUCTION
Shared decision making (SDM) occurs when a patient and clinician both participate in medical decision making, jointly weighing medical evidence and patient preferences. The 4 components of SDM are that both the clinician and patient are involved in decision making, share information, build consensus, and agree on treatment.1
SDM has benefits, including improved patient knowledge and reduced uncertainty and overuse.2–4 Consequently, this form of decision making has been endorsed by professional societies and legislation.5,6 Despite considerable efforts to improve SDM, however, scant data exist on how it has changed nationally over time.
METHODS
We analyzed data from adults aged 18 years and older participating in the 2002 to 2014 Medical Expenditure Panel Survey (MEPS), a nationally representative survey of repeated cross-sections of the noninstitutionalized US civilian population.7 Each year, 21,915 to 26,509 participants completed this survey (response rate = 49% to 65%). The MEPS includes an additional mail-back component, the adult self-administered questionnaire, which contains additional items measuring respondents’ attitudes about health care (annual response rate range = 91% to 94%).
Participants self-reported having a usual source of care by naming a specific clinician to which “you usually go if you are sick or need advice about your health” and the race/ethnicity of that clinician.
We determined use of SDM as perceived by participants from their responses to 7 questions (annual response rate = 91% to 94%).8,9 Three questions were presented only if the participant had a usual source of care; others were presented if the participant had visited a clinic at least once in the past year. We included only respondents who answered all 7 questions: 12,138 in 2002 and 9,049 in 2014.
Six of the questions on the MEPS questionnaire had a never/sometimes/usually/always response scale: how often did your clinician (1) ask you to help decide; (2) show respect for alternative treatments; (3) listen carefully to you; (4) explain things so they were easy to understand; (5) show respect for you; and (6) spend enough time with you. The final question on the MEPS questionnaire had yes/no response options and asked did your clinician present all the options to you (for verbatim questions, see Supplemental Appendix 1, available at http://www.annfammed.org/content/15/6/552/suppl/DC1/). We computed an SDM composite score for each participant, defined as his or her total number of “always” or “yes” responses (for analysis of scores as continuous variables, see Supplemental Appendix 2, available at http://www.annfammed.org/content/15/6/552/suppl/DC1/). Possible composite scores therefore ranged from 0 to 7, with higher scores indicating greater SDM.
To assess whether patient-reported SDM changed over time, we compared the mean SDM composite between 2002 and 2014 with a χ2 test adjusted for the survey design.10 To evaluate independent predictors of SDM, we used multivariate linear regression analysis, adjusting for all variables (see Table 1). The dependent variable was the linear SDM composite score. In all analyses, we accounted for the complex design of the MEPS and present weighted percentages.11,12 We performed all analyses with SAS version 9.4 (SAS Institute, Inc). The Harvard Medical School Institutional Review Board determined that this study did not constitute human subjects research.
Characteristics of the Medical Expenditure Panel Survey Participants and Independent Predictors of Shared Decision Making, 2002–2014
RESULTS
From 2002 to 2014, participants in MEPS became older, less white, more Hispanic, and more educated, and they less often had private insurance and a usual source of care (all P <.05; Table 1).
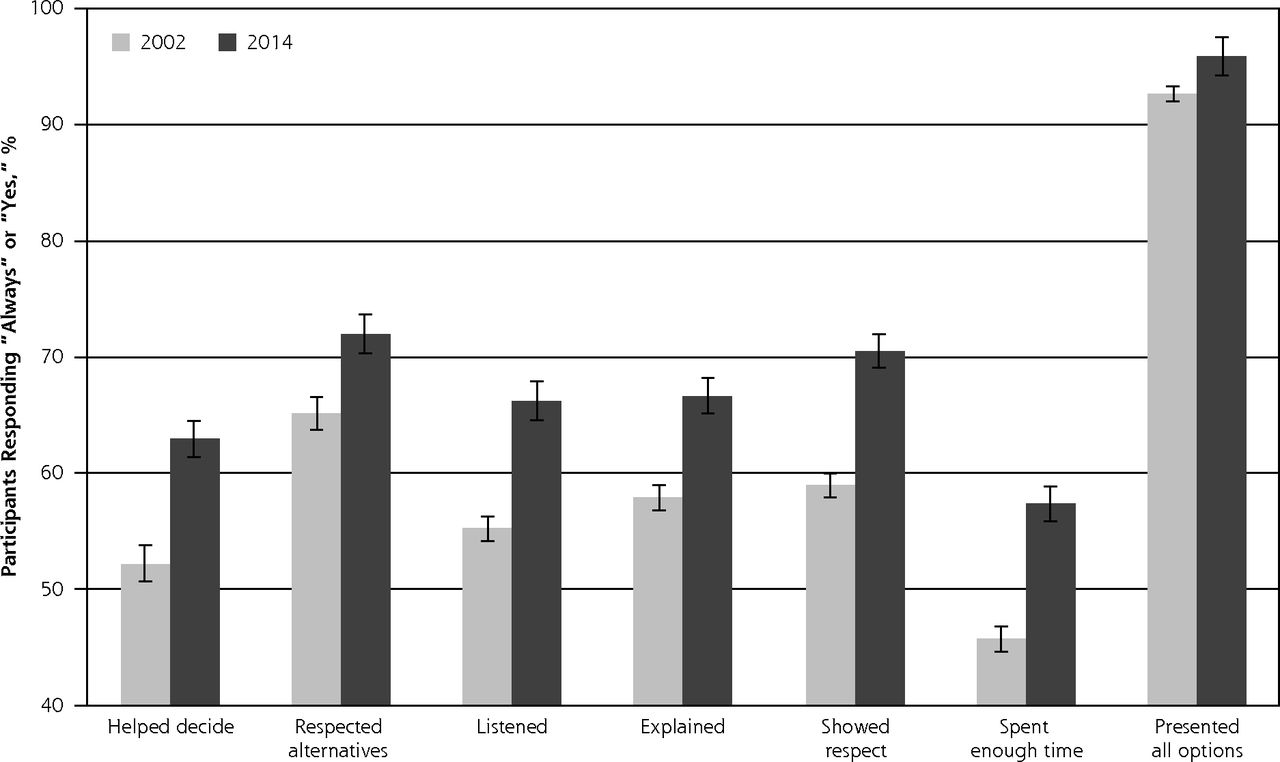
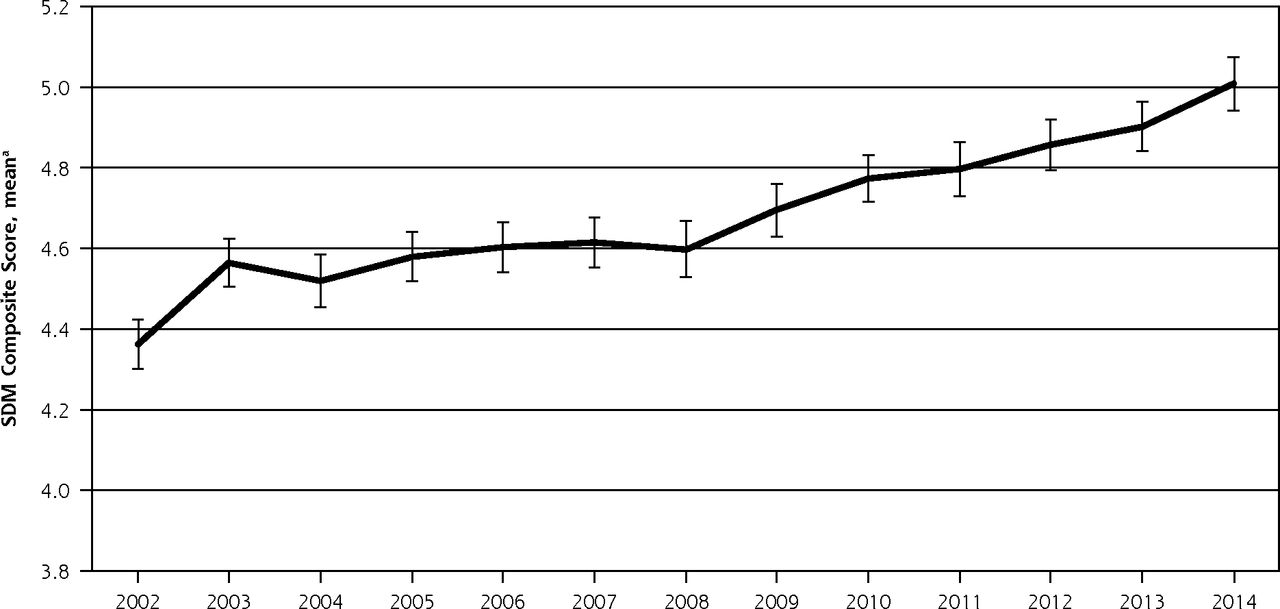
The proportion of participants giving “always” or “yes” responses increased significantly from 2002 to 2014 for all 7 of the SDM questions exploring patient-clinician interactions (Figure 1a). For instance, the proportion increased from 52% to 63% for “helped decide,” from 65% to 72% for “respected alternatives,” and from 93% to 96% for “presented all options” (all P <.05). The mean SDM composite score increased from 4.4 (95% CI, 4.3–4.4) to 5.0 (95% CI, 4.9–5.1; P <.01; Figure 1b) out of 7 points.
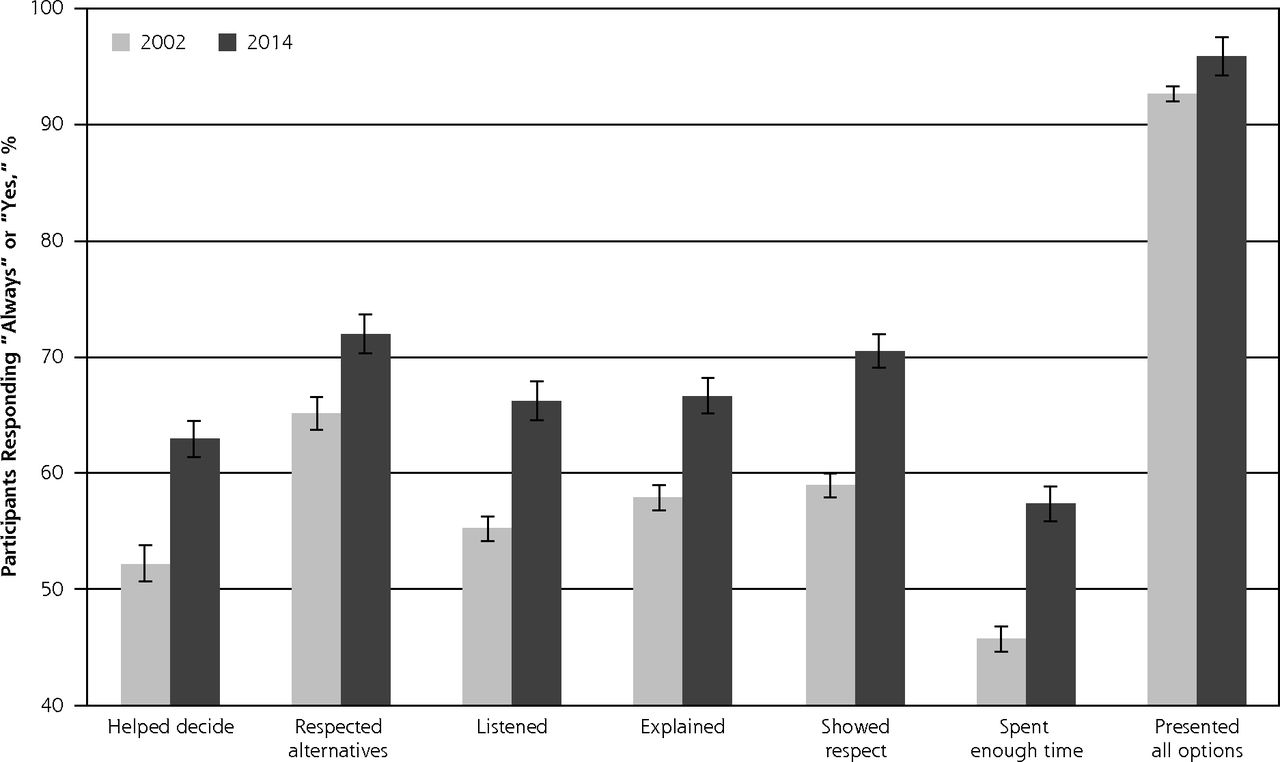
Trends in components of shared decision making, 2002–2014.
Note: Change between 2002 and 2014 for each question included in the SDM composite. All comparisons P <.01.
Error bars represent 95% CIs (for verbatim questions, see Supplemental Appendix, available at http://www.AnnFamMed.org/content/15/6/552/suppl/DC1/).

Trend in shared decision-making composite score, 2002–2014.
SDM=shared decision making.
a Number of points out of 7.
Note: Change from 2002 to 2014 in the SDM composite score. Comparison of 2002 to 2014: P <.01.
Error bars represent 95% CIs (for verbatim questions, see Supplemental Appendix, available at http://www.AnnFamMed.org/content/15/6/552/suppl/DC1/).
In multivariate analyses, independent predictors of higher SDM scores included calendar year (+0.04 points/ year), black vs white race/ethnicity (+0.33 points), and having a same-race/ethnicity usual source of care (+0.24 points) (all P <.05; Table 1). Characteristics independently associated with lower SDM scores included Asian vs white race/ ethnicity (−0.28 points), being uninsured (−0.17 points), and poor perceived health (−0.41 points) (all P <.05).
DISCUSSION
Between 2002 and 2014, patient-reported SDM increased significantly among adult Americans. There were increases in all 4 core components of SDM (joint involvement in decisions, sharing of information, building of consensus, and agreeing on treatment), although sociodemographic disparities and relatively poor performance for certain aspects of SDM persisted.
To improve SDM, interventions might focus on factors associated with low SDM scores. SDM was lower when participants’ usual source of care was of different race/ethnicity. Lower scores of those with more education may reflect different expectations among this population.13 Lower SDM scores among individuals with worse health status suggest interventions to improve SDM should target these patients, as they might stand to gain the most from this joint approach to decision making.
Our study has limitations. First, although SDM likely translates into improved patient knowledge and better decisions regarding use of services with marginal, unclear, or no benefit,2,3 the impact of these improvements on overall outpatient quality of care is unclear.14 Second, additional items or direct observation (vs self-report), or both may better capture SDM. Others have found low rates of SDM (eg, 3 to 50 points out of 100 with a different instrument).15 Third, we could not assess SDM for specific clinical questions (eg, mammography before age 50) that might vary based on patient preferences. Fourth, we were unable to capture some factors that might influence SDM, such as time pressure or inadequate reimbursement. Fifth, unmeasured confounding precludes a definitive answer as to whether the observed independent predictors of SDM in fact play a causal role. Finally, not all patients desire SDM, so the ideal level of this form of decision making is unknown.13
Among adult Americans, patient-reported use of SDM increased significantly from 2002 to 2014, despite sociodemographic disparities and poor performance in some areas. Beyond increasing insurance coverage, efforts to improve SDM should target Americans without a same-race/ethnicity usual source of care and with poor perceived health.
Footnotes
↵* Dr Landon and Dr Linder contributed equally to this manuscript
Conflicts of interest: authors report none.
Funding support: Dr Levine received funding support from an Institutional National Research Service Award (T32HP10251), the Ryoichi Sasakawa Fellowship Fund, and the Brigham and Women’s Hospital Division of General Internal Medicine and Primary Care.
Disclaimer: All funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Previous presentation: Presented at the Society of General Internal Medicine – New England Regional Meeting; March 9, 2017; Boston, Massachusetts.
Author contributions: D.M.L. had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis; Study concept and design: D.M.L.; Acquisition, analysis, or interpretation of data: all authors; Drafting of the manuscript: D.M.L.; Critical revision of the manuscript for important intellectual content: all authors; Statistical analysis: D.M.L.; Administrative, technical, or material support: D.M.L.; Study supervision: B.E.L. and J.A.L.
Supplementary materials: Available at http://www.AnnFamMed.org/content/15/6/552/suppl/DC1/.
- Received for publication January 27, 2017.
- Revision received June 14, 2017.
- Accepted for publication July 7, 2017.
- © 2017 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}