
Article Figures & Data
Figures
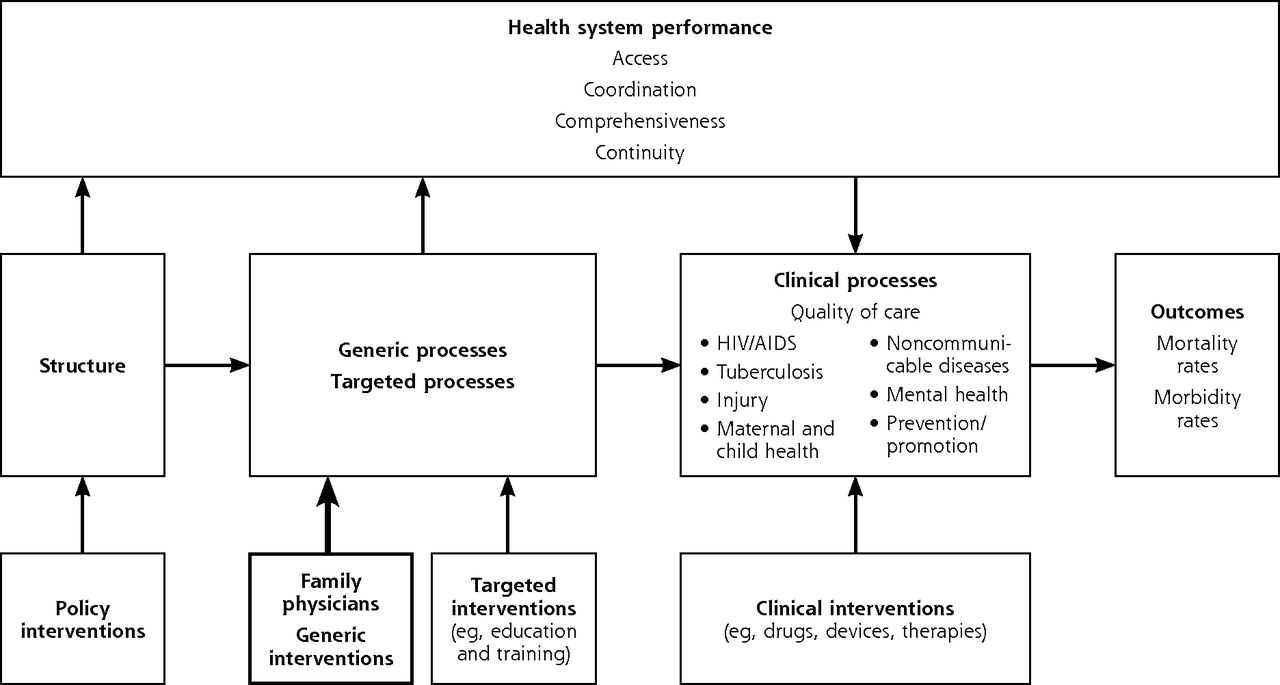
- Figure 1
Conceptual framework of the study (a modified Donabedian causal chain).24,25

Tables
Facility Type Criteria Used for Matching District hospitals Province Rural vs metropolitan setting Size based on number of beds Small (50–150 beds) Medium (150–300 beds) Large (300–600 beds) Community health centers Province Rural vs metropolitan setting Annual number of patient visits (primary health care head count) 24-hr open access Presence of a midwife obstetric unit Facility Type Aspect Measureda Data Collection Instrument/Tool Reliability/ Validity of Tool Data Source Data Collection Method Nature of Variables District hospital Health system performance Signal functions (percentage of essential functions and services available for each clinical domain)28–30 Audit tool used by MRC team (adapted from WHO document, validated for South African context) Staff, managers, and key documents Interviews and review of documents Continuous variables (percentage of total score for each clinical domain) South African National Core Standards (Domain 2, which focuses on aspects of patient safety, clinical governance, and clinical care)31 National tool, validated by Office of Health Standards Compliance Continuous variables (percentage of total score for Domain 2) Quality of clinical care and health outcomes Child PIP and Perinatal PIP32 Validated tools (software based) used in South African health facilities Child PIP and Perinatal PIP national databases Assessment of data at facility level (admissions and deaths of children and perinatal losses) Continuous variables (rates) Community health center Health system performance PCAT: 4-point Likert scale; domains of Primary Health Care33 Pilot study and validation in Western Cape province Patients, practitioners, and managers Interviews, asking respondents to rate their agreement with each item on a 4-point Likert scale Continuous variables (4-point Likert scale options were ordinal values, but variables were treated as continuous) Quality of clinical care and health outcomes Integrated CDM audit tool: percentage score34,35 Valid tool (annual audit in Western Cape provincial facilities) Observation and patient medical records Assessment of facility’s structural components for CDM, as well as audit of 20 records for each of 5 chronic conditions (diabetes, hypertension, asthma, COPD, and epilepsy) Continuous variables (percentage of total score for each chronic condition) CDM = chronic disease management; COPD = chronic obstructive pulmonary disease; MRC = Medical Research Council of South Africa; PCAT = Primary Care Assessment Tool; PIP = Problem Identification Program; WHO = World Health Organization.
↵a From the conceptual framework shown in Figure 1.
Facility Without Family Physicians (n=15) With Family Physicians (n=15) District hospitals Location Rural, No. 15 12 Metropolitan, No. 0 3 Beds, mean (SD), No. 153.5 (92.4) 198.0 (81.7) Size based on number of beds Small, No. 8 6 Medium, No. 7 7 Large, No. 0 2 Community health centers Location Rural, No. 6 6 Metropolitan, No. 9 9 Patient visits per year, mean (SD), No. 152,541 (122,714) 255,094 (178,501) Daily open hours Open 8 hours, No. 6 4 Open 24 hours, No. 9 11 Midwife obstetric unit available Yes, No. 10 12 No, No. 5 3 - Table 4
Comparison of Indicators of Health System Performance and Clinical Processes Between Facilities With and Without Family Physicians
Tool and Indicator Without Family Physicians, Mean Value (SD) With Family Physicians, Mean Value (SD) Mean Difference (95% CI) P Value District hospitals Signal functions (essential services) tool (n = 22) Newborn care, % 92.7 (6.4) 95.0 (6.5) −2.29 (−8.05 to 3.46) .42 Maternal care, % 89.1 (19.2) 96.2 (5.4) −7.05 (−20.21 to 6.11) .28 Surgery, % 63.6 (24.5) 76.4 (16.7) −12.73 (−31.80 to 6.34) .18 General medicine, % 65.8 (17.8) 78.0 (21.0) −12.17 (−29.41 to 5.07) .16 Mental health, % 83.3 (15.1) 80.8 (7.9) 2.50 (−8.55 to 13.55) .64 Pediatric care, % 69.2 (15.1) 85.0 (14.3) −15.83 (−28.99 to −2.67) .02 Emergency care, % 78.3 (20.0) 90.0 (15.6) −11.67 (−27.85 to 4.52) .15 South African National Core Standards tool (n = 19) Score for Domain 2 (focuses on aspects of patient safety, clinical governance, and clinical care) 76.25 (24.79) 89.79 (14.28) −13.54 (−35.20 to 8.11) .19 Child PIP tool (n = 26) In-hospital mortality rate (number of deaths per 100 pediatrics admissions) 2.9 (2.3) 1.4 (1.3) 1.50 (−0.06 to 3.06) .059 Modifiable factor rate per death (number of modifiable factors identified per audited pediatric death, ie, instances of suboptimal care or missed opportunities) 4.7 (3.9) 2.2 (1.9) 2.49 (0.18 to 4.96) .049 Perinatal PIP tool (n = 26) Perinatal mortality rate (number of perinatal deaths per 1,000 total births, all deliveries) 26.74 (12.13) 23.32 (7.79) 3.42 (−4.53 to 11.38) .38 Neonatal mortality rate (number of neonatal deaths per 1,000 live births, all deliveries) 10.75 (7.02) 7.44 (3.53) 3.31 (−1.01 to 7.63) .13 Stillbirth rate (number of stillbirths per 1,000 total births, all deliveries) 17.54 (9.30) 16.64 (5.39) 0.90 (−5.34 to 7.14) .77 Community health centers PCAT tool completed by health care users (n = 30)a First-contact use (care is first sought from the primary care clinician when a new health need arises; a behavioral characteristic) 3.41 (0.42) 3.22 (0.34) 0.19 (−0.10 to 0.50) .19 First-contact access (services must be accessible; a structural characteristic) 2.52 (0.99) 2.48 (0.93) 0.04 (−0.70 to 0.80) .90 Continuous (ongoing) care (longitudinal use of a regular source of care over time, resulting in a long-term relationship between clinician and patient) 3.03 (0.31) 2.79 (0.29) 0.24 (0.02 to 0.50) .03 Coordination of care (linking of health care visits and services so that patients receive appropriate care for all their health problems) 3.51 (0.39) 3.05 (0.55) 0.45 (0.10 to 0.80) .02 Coordination of information (the essence of coordination is the availability of information about prior and existing problems and services) 3.41 (0.43) 3.16 (0.47) 0.25 (−0.10 to 0.60) .14 Comprehensiveness: services available (availability of a wide range of primary care services) 3.32 (0.44) 3.16 (0.43) 0.16 (−0.20 to 0.50) .31 Comprehensiveness: services provided (appropriate provision of primary care services, including services that promote and preserve health) 3.33 (0.62) 3.15 (0.58) 0.18 (−0.30 to 0.60) .41 Family-centeredness (appropriate care that recognizes the family as a major participant in patient assessment and treatment) 3.37 (0.52) 2.97 (0.63) 0.40 (−0.02 to 0.80) .07 Community orientation (care that is delivered in the context of the community) 2.83 (0.58) 2.63 (0.57) 0.20 (−0.20 to 0.60) .34 Cultural competency (care that honors and respects the beliefs, interpersonal styles, attitudes, and behaviors of people as they influence health) 3.52 (0.49) 3.24 (0.49) 0.28 (−0.10 to 0.60) .13 Primary health care team (availability of other members of the primary health care team, such as physiotherapists, social workers, dentists, dietitians, mental health workers, and community health workers) 3.52 (0.52) 3.24 (0.52) 0.28 (−0.10 to 0.70) .15 Integrated CDM audit score Structural aspects required for chronic disease management, % (n=25) 72.45 (19.04) 72.55 (22.57) −0.10 (−17.46 to 17.23) .99 Diabetes score, % (n = 27) 39.48 (10.85) 40.55 (13.79) −1.07 (−10.86 to 8.73) .82 Hypertension score, % (n = 28) 45.96 (10.99) 44.59 (13.66) 1.37 (−8.27 to 11.00) .77 Asthma score, % (n = 25) 47.41 (8.08) 42.28 (8.08) 5.13 (−1.60 to 11.87) .13 COPD score, % (n = 18) 32.24 (16.90) 29.49 (15.98) 2.75 (−13.85 to 19.34) .73 Epilepsy score, % (n = 26) 35.78 (18.51) 39.01 (16.26) −3.23 (−17.45 to 10.99) .64 CDM = chronic disease management; COPD = chronic obstructive pulmonary disease; PCAT = Primary Care Assessment Tool; PIP = Problem Identification Program.
↵a Scored from 1 = definitely not to 4 = definitely; higher scores indicate better care.
Supplemental Appendixes
Supplemental appendixes
Files in this Data Supplement:
- Supplemental data: Appendixes - PDF file
The Article in Brief
The Influence of Family Physicians Within the South African District Health System: A Cross-Sectional Study
Klaus B. von Pressentin , and colleagues
Background Family medicine is relatively new as a formal medical discipline in South Africa. As the country moves toward a national health insurance system, researchers set out to assess the influence of family physicians in community health centers and district (generalist) hospitals.
What This Study Found District (generalist) hospitals with family physicians have better clinical processes and health system performance, while community health centers with family physicians have lower scores in those domains. In a study across seven South African provinces, district hospitals with family physicians had higher availability of essential services, such as pediatric and emergency care, and better child and neonatal health. In contrast, community health centers with family physicians generally had lower scores for health system performance and clinical care and were associated with significantly lower scores for continuity and coordination of care. These findings differ from a large body of literature which finds that family physicians enhance continuity and coordination. The authors hypothesize that the differences might be due to the areas in which family physicians were deployed (areas of greatest need and workload, which were predisposed to perform more poorly) and/or to differing levels of physician influence (hospital teams were led by doctors, community health center teams were led by nurses).
Implications
- The authors call for training programs that have sufficient focus on community health settings and further exploration of family physicians� roles in community health centers.




{kind=link}