
Abstract
Board certification is associated with higher quality care. We sought to determine the rates and predictors of attrition from certification among family physicians who achieved initial certification with the American Board of Family Medicine from 1980 through 2000. In this period, 5.6% of family physicians never attempted recertification, with the rate increasing from 4.9% between 1990 and 1995 to 5.7% from 1996 to 2000. Being male, an international medical graduate, or 30 years of age or older at initial certification was associated with not recertifying. With information about those likely to leave certification, the board can design and implement interventions that minimize attrition.
INTRODUCTION
Crossing the Quality Chasm publicized widespread gaps in quality1 and called for medical certification boards to evolve from assessors of competency to facilitators of lifelong learning. In response, medical boards launched maintenance of certification (MOC) programs.2 In 2003, the American Board of Family Medicine (ABFM) transitioned to its MOC program, allowing diplomates to extend their original 7-year certificates by 3 years through demonstration of professionalism, knowledge assessment, and performance improvement.2 As of 2011, certification depends on meeting specific requirements every 3 years and passing the examination at least every 10 years.
Although board certification has been associated with benefits, such as improved clinical knowledge, higher quality care, and less disciplinary action, some physicians leave the certification process.3–5 Of the diplomates who certified or recertified in 2003, 23% did not maintain certification. Reasons included not completing MOC, failing the examination, and retirement.6 Independently, Lipner and Freed found that internists and general pediatricians left MOC because of the perceived time, expense, and lack of necessity.7,8 These perceptions have resulted in circumvention of established certifying boards by certification through alternative, upstart boards.9 Given this situation, we sought to determine the percentage of physicians not attempting recertification after their initial certification, and to describe their characteristics.
METHODS
Data Sources
In this cross-sectional analysis, we used ABFM data to determine whether family physicians initially certifying from 1980 through 2000 recertified. Our starting year is after the 1977 closing of an ABFM pathway that allowed general practitioners who had never completed residencies to obtain certification.
Variables
We categorized all diplomates who live in the United States and initially certified between 1980 and 2000 as either successfully recertifying or not attempting recertification as of December 31, 2015. Diplomates attempting but not achieving recertification were excluded. We recorded the number of initial certification examination failures, diplomate age at initial certification (<30, 30–34, 35–39, and ≥40 years), sex, and current region. We distinguished doctors of medicine from doctors of osteopathy and international medical graduates from US medical graduates We divided our study period into 3 initial certification year cohorts: 1980–1989, 1990–1995, and 1996–2000. At recertification, those in the 1996–2000 cohort were aware of the MOC transition.
Analytic Plan
We grouped physicians by initial certification year and calculated the percentage not attempting recertification. We conducted bivariate analyses and used χ2 to identify differences between those who recertified and those who did not attempt recertification. Finally, we used a logit model where the dependent variable was not attempting recertification. Our covariates were the aforementioned characteristics. We conducted the analysis with Stata 14.0 (Stata Corp, LLC), and the American Academy of Family Physicians Institutional Review Board deemed the protocol exempt.
RESULTS
Of the 51,678 family physicians included, 5.6% did not attempt recertification. Across time periods, the rate was 6.6% for 1980–1989 before falling to 4.9% for 1990–1995 and then rising to 5.7% for 1996–2000 (Figure 1).

Percentage not attempting recertification, by initial certification year (unadjusted).
The percentage not attempting recertification increased with each additional failed initial certification attempt, rising to 24% for the diplomates who failed 3 or more times (Table 1). There was also a regional trend, ranging from 4.7% of Midwestern diplomates to 6.4% of Southern diplomates not attempting recertification. International medical graduates, men, and diplomates aged 30 years or older were more likely to not attempt recertification.
Demographic Characteristics of Diplomates Passing or Not Attempting Recertification
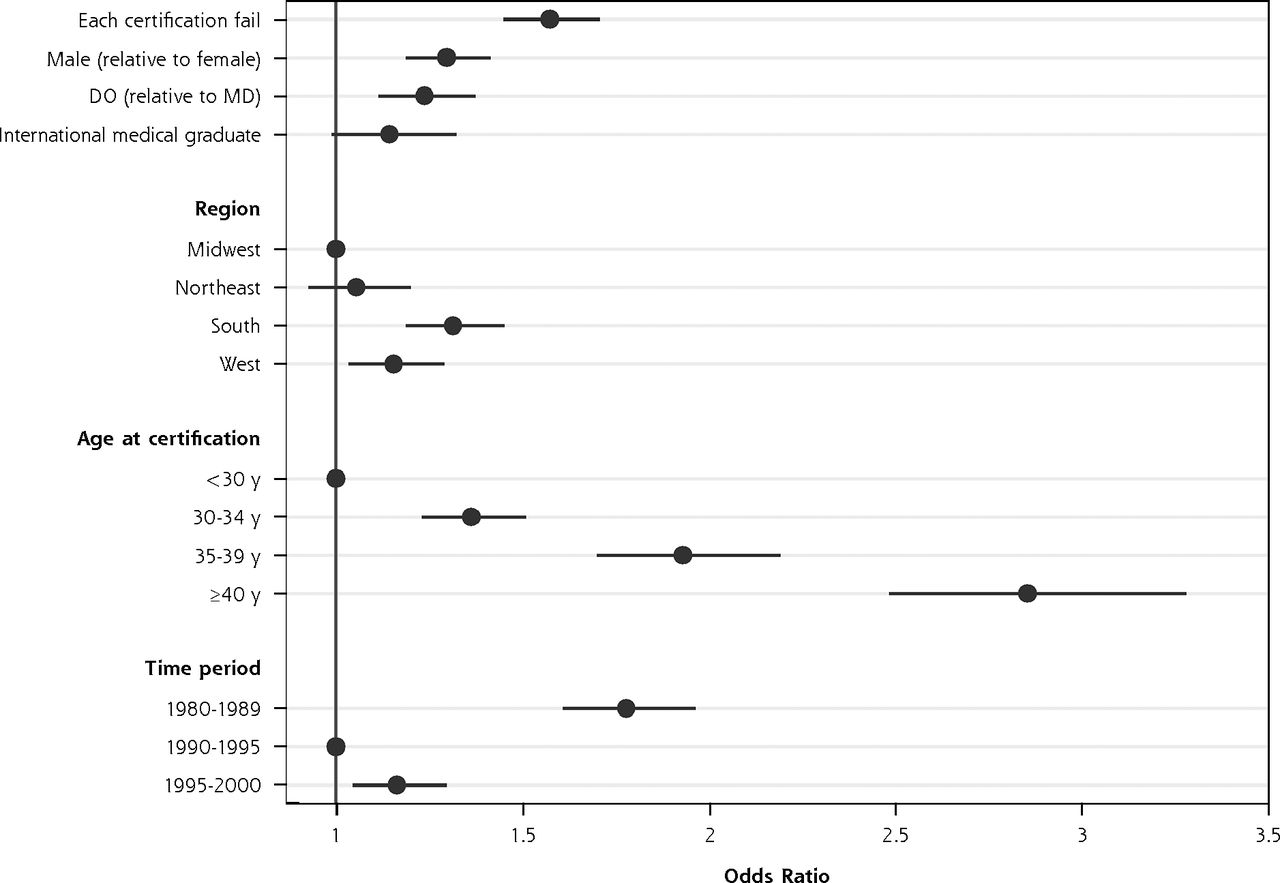
These associations (initial certification failures, region, international medical graduate status, sex, and age) remained significant in our regression model. Compared with the 1990–1995 group, physicians certifying in 1996–2000 had 16% higher odds of not attempting to recertify (P <.01) whereas diplomates who certified before 1990 had 78% higher odds (P <.001) (Figure 2, Supplemental Table 1, http://www.annfammed.org/content/16/1/55/suppl/DC1).

Logit regression of factors associated with not attempting recertification.
DO = doctor of osteopathic medicine; MD = medical doctor.
Note: 95% CIs shown.
DISCUSSION
We found that 5.6% of those initially certifying from 1980 through 2000 did not attempt to recertify. Men, international medical graduates, those in the South, and diplomates 30 years of age or older were more likely to not attempt recertification. These estimates differ from other reports. For example, of all diplomates successfully recertifying in 2003, 23% did not maintain certification,6 indicating that diplomates eligible to recertify for the second, third, or fourth times are less likely to do so.
Our findings are important for 2 reasons. First, the primary care workforce is facing projected shortages and increasing burnout.10 We hypothesize that certification attrition is a transitional step between burnout and leaving the primary care workforce although future studies should elucidate the relationship. Second, MOC is a shift that has provoked fears of attrition.9 Although we confirmed that later cohorts are leaving certification at higher rates, the absolute numbers are small.
The ABFM has pursued several strategies to minimize attrition. Its PRIME Registry has the potential to simplify reporting for certification and payment. The ABFM is also assessing burnout and partnering with the American Academy of Family Physicians to provide resources for those at risk. Finally, family medicine residents are completing certification activities during training to better acquaint them with MOC.
Several limitations should be considered. First, we only examined the first recertification. A diplomate who initially certifies in 1980, recertifies in 1987, but leaves clinical practice or recertifies in a different specialty was therefore categorized as successfully recertifying. Second, it is possible that more recent cohorts do not follow these trends. We ended in 2000 to accommodate the time it takes to capture certification lapses. Finally, although those physicians initially certifying in 2000 knew about the forthcoming MOC changes, they were not subject to them.
In conclusion, 5.6% of family physicians did not attempt recertification, and the percentage increased slightly among the most recent cohort. We recommend following these trends, uncovering the underlying motivations, and identifying additional interventions that minimize attrition.
Footnotes
Conflicts of interest: Drs Peterson and Puffer are employed by the American Board of Family Medicine.
Funding support: The Robert Graham Center received support for this study from the American Board of Family Physicians in the form of a contract for ongoing collaborative research.
Previous presentation: North American Primary Care Research Group; Nov 12–16, 2016; Colorado Springs, Colorado.
Supplemental materials: Available at http://www.AnnFamMed.org/content/16/1/55/suppl/DC1/.
- Received for publication March 6, 2017.
- Revision received July 26, 2017.
- Accepted for publication August 25, 2017.
- © 2018 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}