
Article Figures & Data
Figures
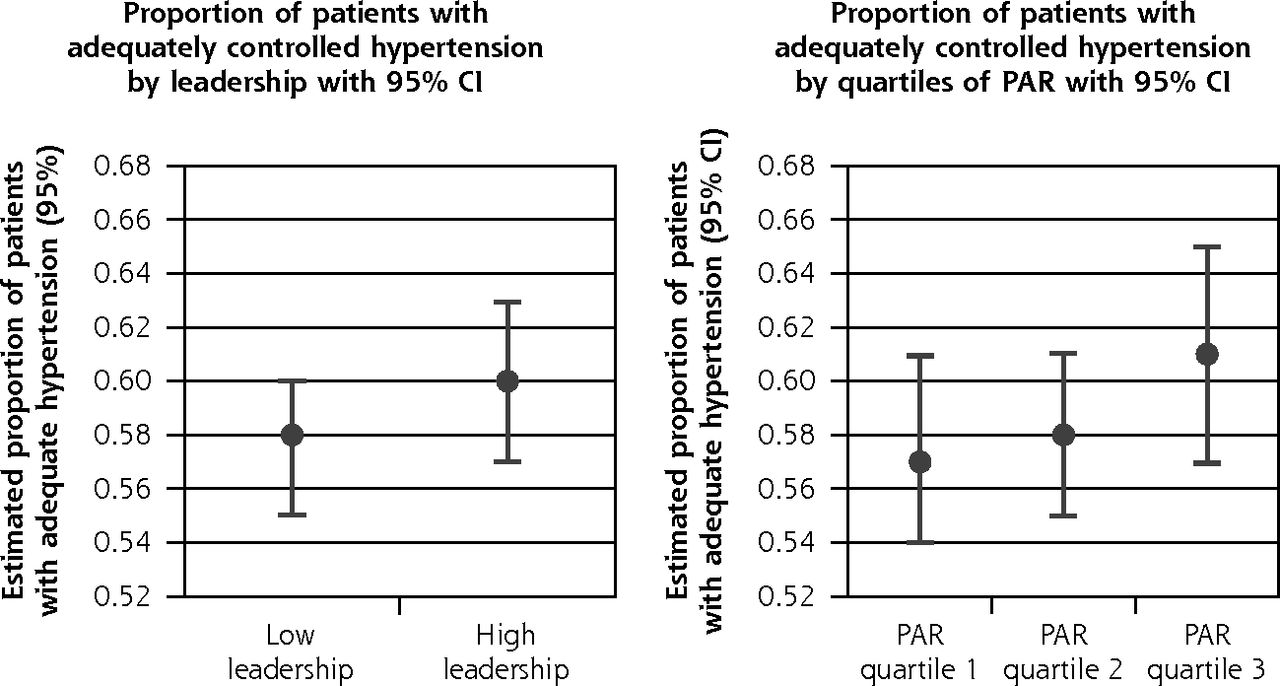
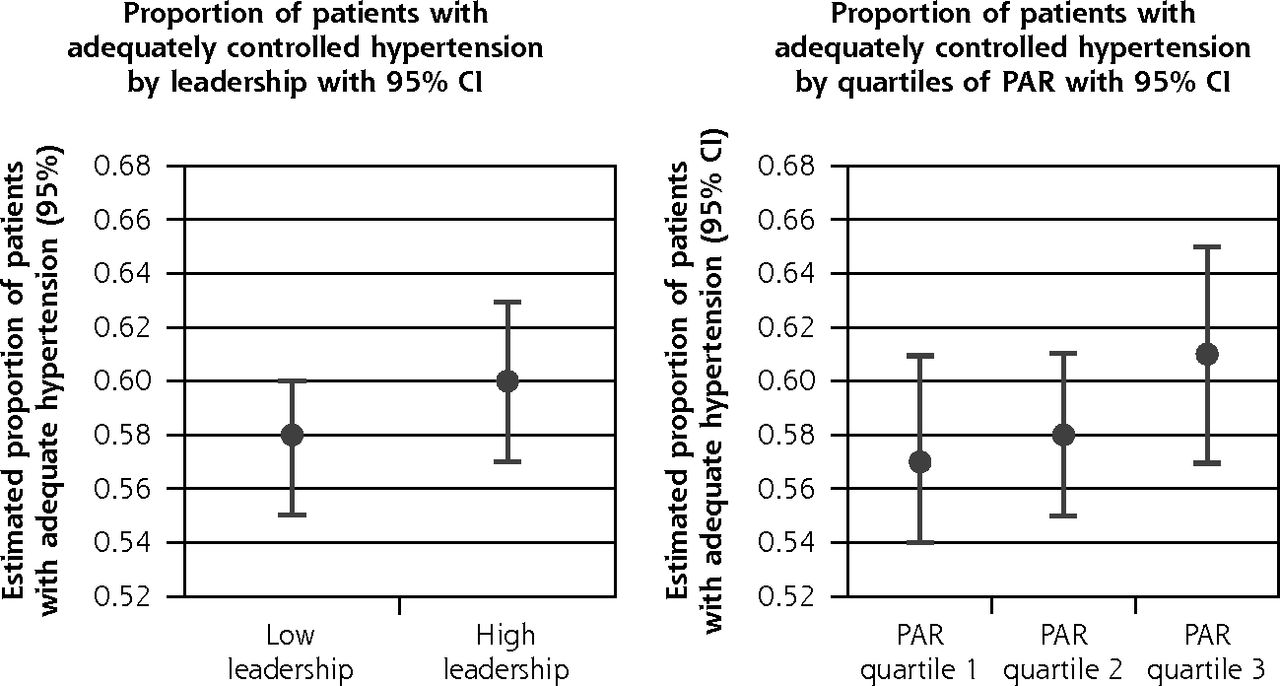
- Figure 1
Predicted practice-level performance on blood pressure control measure stratified by organizational quality improvement characteristics.
KDIS = Key Drivers of Implementation Scale; PAR =practice adaptive reserve.
Note: Unadjusted linear regression models were used to estimate predicted proportion of hypertension control.
aPredicted mean practice-level adequate hypertension control calculated using linear regression models.
bNo statistical difference between mean adequate hypertension control and higher leadership quality improvement capability (P =.321).
cNo statistical difference between mean adequate hypertension control and higher quartiles of PAR (P =.504).
Tables
Characteristic Valuea Adequate hypertension control Patient-level, No. (%)b 104,473 (61) Top quartile control, No. (% controlled)c 46 (>68) Clinicians per clinic, mean No. (SD)d 6.5 (8.5) Office staff per clinic, mean No. (SD) 9.4 (18.5) Ownership structuree Physician owned, No. (%) 77 (58) Health or hospital system ownership, No. (%) 56 (42) Payer mixf Medicare, mean % 29 Medicaid, mean % 16 Commercial insurance, mean % 29 Uninsured, mean % 12 Clinician practice visits per day, mean No. 21 Practice type PCMH, No. (%) 89 (61) FQHC, No. (%) 34 (30) Rural, No. (%) 19 (17) Staff role of survey respondentsg Physician, nurse practitioner, physician assistant, No. (%) 98 (14) Nurse, medical assistant, No. (%) 378 (54) Billing, receptionist, office manager, No. (%) 218 (31) FQHC = federally qualified health center; PCMH = patient-centered medical home.
Note: Total number of patients with hypertension among the practices = 171,570.
↵a Percentages and mean numbers listed may reflect rounding.
↵b Percentages represent patients that met adequate hypertension control among all the practices included in our analysis (last clinic blood pressure was <140/90 mm Hg).
↵c Primary care clinics among top quartile for adult adequate hypertension control.
↵d Practice size information was not available for 48 practices, and information displayed is among practices for which data were available.
↵e Practice ownership was not available for 43 practices and information displayed is among practices for which data were available.
↵f The total of payer mix values is 86% because 14% of the payer mix was dual or outside the payer categories described in Table 1.
↵g The total of subvalue is 99% because staff were able to specify more than 1 role (n=6).
Top Quartile Hypertension Practice-Level Characteristic Top Quartile Achieved
n=46Top Quartile Not Achieved
n=135P Value Clinicians, mean No. (SD) 5 (5.4) 5.6 (4.8) .596 Office staff, mean No. (SD) 8.6 (11.4) 8.3 (7.8) .917 Physician owned, No. (%) 27 (35) 50 (65) .015 Payer mix Medicare, % (SD) 28 (19.2) 29 (14.8) .776 Medicaid, % (SD) 15 (11.6) 17 (11.7) .477 Commercial insurance, % (SD) 37 (15.9) 26 (18.3) .002 Uninsured, % (SD) 8 (9.5) 14 (14.7) .055 Practice delivery model PCMH, No. (%) 29 (33) 60 (67) .014 FQHC, No. (%) 5 (15) 29 (85) .179 Organizational quality improvement quality PAR score, mean (SD)a 0.72 (0.11) 0.67 (0.11) .165 KDIS leadership scoreb,c 0 7 9 … 1 17 59 … 2 14 42 … 3 8 25 … FQHC = federally qualified health center; KDIS = Key Driver Implementation Scale; PAR = practice adaptive reserve; PCMH = patient-centered medical home; QI = quality improvement.
↵a PAR scores are scaled from 0 to 1, with 1 being a perfect score of agreement for organizational adaptiveness.
↵b KDIS Leadership scores are scaled from 0 to 3, with 3 being a perfect score that leadership recognizes QI work as part of the daily routine and practice culture.
↵c P=.356, estimated from χ2 analysis comparing ordinal leadership scores for all practices achieving top quartile hypertension control vs not achieving top quartile hypertension control.
- Table 3
Association of Practice Adaptive Reserve and Advance Leadership in Quality Improvement Capability With Target Hypertension
Quality Improvement Contextual Factors PR (CI) P Value Adjusted PR (CI)a P Value Leadershipb Low leadership (score 0–1) 1 [Referent] 1 [Referent] High leadership (score 2–3) 0.94 (0.57–1.56) .833 0.81 (0.48–1.37) .429 PAR scorec 0.00 to <0.66 1 [Referent] 1 [Referent] 0.65 to <0.76 1.47 (0.71–3.03) .297 1.25 (0.52–2.99) .611 0.76 to 1.00 1.92 (0.9–4.1) .091 1.45 (0.56–3.76) .440 High leadership+PAR scoresd High leadership 0.93 (0.57–1.53) .776 PAR (0.65 to <0.76) 1.48 (0.72–3.05) .289 PAR (0.76 to 1.00) 1.92 (0.9–4.09) .089 PAR=practice adaptive reserve; PR=prevalence ratio.
↵a Modified Poisson regression models adjusted for the following: proportion of commercially insured patients, practice designation as a patient-centered medical home, and clinician-owned practices
↵b PR: prevalence for top quartile hypertension control among practices with high leadership support for quality improvement implementation divided by the prevalence for top quartile hypertension control among practices with less leadership support for quality improvement implementation.
↵c PR: prevalence for achieving top quartile hypertension control among practices with higher quartiles of PAR divided by the prevalence for top quartile hypertension control among practices with the lowest quartile of PAR.
↵d PR reflects adjustments for both high leadership support for quality improvement implementation and higher quartiles of PAR when compared to the referent (low leadership support for quality improvement implementation and lowest quartile of PAR).




{kind=link}