
Abstract
PURPOSE Providing care in alternative (non-office) locations and outside office hours are important elements of access and comprehensiveness of primary care. We examined the trends in and determinants of the services provided in a cohort of primary care physicians in British Columbia, Canada.
METHODS We used physician-level payments for all primary care physicians practicing in British Columbia from 2006-2007 through 2011-2012. We examined the association between physician demographics and practice characteristics and payment for care in alternative locations and after hours across rural, urban, and metropolitan areas using longitudinal mixed-effects models.
RESULTS The proportion of physicians who provided care in alternative locations and after hours declined significantly during the period, in rural, urban, and metropolitan practices. Declines ranged from 5% for long-term care facility visits to 22% for after-hours care. Female physicians, and those in the oldest age category, had lower odds of providing care at alternative locations and for urgent after-hours care. Compared with those practicing in metropolitan centers, physicians working in rural areas had significantly higher odds of providing care both in alternative locations and after hours.
CONCLUSION Care provided in non-office locations and after office hours declined significantly during the study period. Jurisdictions where providing these services are not mandated, and where similar workforce demographic shifts are occurring, may experience similar accessibility challenges.
INTRODUCTION
Achieving high quality and patient-centered care requires health care system structures that support physician service delivery outside regular office hours and away from regular office locations. For example, when urgent care is required after hours, access to a primary care provider can support improved continuity and reduce costly emergency department visits.1–3 The United States and Canada, however, are the least likely among Organization for Economic Cooperation and Development nations to offer after-hours access arrangements (35% of American and 45% of Canadian practices).4–6 Sixty-three percent of Canadians and 51% of Americans report that they find it very or somewhat difficult to get care after hours without going to an emergency department.7 Furthermore, increasing frailty in the community underlines the importance of providing care at patients’ homes and in long-term care facilities as well as in hospitals, and emergency departments.8 This need will continue to grow as the population ages.
Understanding who is and is not providing these services is critical; however, evidence is limited. The studies that exist suggest that care provision in non-office locations by primary care physicians may be declining9–12; these studies, however, are based on cross-sectional survey data. They did not capture trends over time among the same cohort of providers, nor differences between rural, urban, and metropolitan practices, and also may be subject to recall and selection biases.
Participation in on-call arrangements, and practice in alternative locations are not mandated in British Columbia (BC). However, as part of their Professional Standards and Guidelines, the College of Physicians and Surgeons of BC (the physician licensing body in BC) states that it is “a physician’s ethical, professional and legal obligation to provide appropriate ongoing and after-hours coverage for all patients under his or her care”.13 Broad policy statements also support the provision of comprehensive primary care in multiple locations,14 and there have been some specific efforts to financially incentivize provision of care in alternative locations and after hours, as well as to participate in on-call rota.12
In this longitudinal population-based analysis we examine the trends in and determinants of care provided in non-office locations, after hours, and on-call rota participation among primary care physicians in BC. We compare patterns across rural, urban, and metropolitan areas.
METHODS
Primary care physicians in Canada are typically small business operators remunerated under a fee-for-service model with total fees negotiated between the physician medical association (Doctors of BC) and the BC Ministry of Health. Alternative payments, such as salary or sessional agreements, make up less than 20% of payments.15 Physicians are clinically autonomous, and have discretion over the organization and location of their practices.16
Approach and Data Sources
This study used linked, longitudinal, deidentified administrative data from the BC Ministry of Health and the College of Physicians and Surgeons of BC accessed through Population Data BC for the period of April 1, 2006 through March 31, 2012.17 We used the Medical Services Plan physician payment file to track all fee-for-service payments for each physician.18 We linked this with the alternative payment plan database, which contains records on all non-fee-for-service payments to physicians (eg, salary, service contracts, sessional fees).19 We adjusted all fees and payments in both files to 2012 levels to adjust for any fee or payment level changes. This created a payment variable that is a reliable proxy for levels of service provision. We obtained patient age, sex, location of residence, and neighborhood socioeconomic status from the Medical Services Plan consolidation file20 and chronic conditions status from the Medical Services Plan payment and hospitals separations data.21
Our study cohort included all physicians with a primary care specialty who were paid for clinical care delivery (>$0) in at least 1 of the 7 study years, and whose payments were at least in part fee-for-service. Physicians whose remuneration was 100% non-fee-for-service were excluded as our outcomes of interest are not measurable using the alternative payment plan database.
Outcome Measures
Care in Alternative Locations
We identified visits/consultations in patients’ homes, long-term care facilities, emergency departments, and acute-care hospitals (outside emergency departments) in the fee-for-service data by location codes attached to services rendered.22 We also examined consultations provided at any alternative location (by year). Locations included patients’ homes, long-term care facilities, emergency departments and acute-care hospitals, diagnostic facilities, mental health centers, community locations (eg, school), or other.
After-Hours Care and On-Call Participation
We identified urgent after-hours care in the fee-for-service payment data by the presence of a premium applied to payments when care is provided outside regular office hours.22 Annual payments for time spent on call were assigned to each physician in the alternative payment plan database.19
Explanatory Variables
Physician demographic covariates included age (in 10-year groupings), sex, location of training (Canada or international), and practice rurality (metropolitan, urban, or rural) defined using an existing validated rubric.23 In addition, we included a set of variables that characterize a physician’s patient population, including the proportion of each physician’s patient contacts with: women; individuals aged 65 years and over; individuals in the lowest socioeconomic quintile; and individuals with significant morbidity, assessed using Johns Hopkins’ Aggregated Diagnostic Groupings.24,25
Statistical Analyses
We used the χ2 test for differences in payments for visits at alternative locations (home, hospital, emergency department, and long-term care facilities), urgent after-hours care, and time on call, across rural, urban, and metropolitan practice areas, and by study year. We used analysis of variances to examine variation across physician demographic variables, and patient population characteristics.
Payments for care provided in each alternative location (individually, and a composite measure of no alternative locations), urgent after hours, and on-call programs were modeled as dichotomous variables using mixed effects, multivariate logistic models. Recognizing that rural primary care practice differs substantially from urban and metropolitan practice, we elected to stratify our models by rurality.26,27 We included physician sex, other physician demographics, proportion of total clinical income received through the alternative payment plan, and a random effect for subject level residuals under a first-order autoregressive correlation matrix in each model. We expected some variation in payments for care provided in non-office locations and after office hours associated with the characteristics of a physician’s patient population, and therefore incorporated these variables in those models as well.
As a sensitivity analysis, we assessed the proportion of physicians’ overall payments related to care delivered at alternative locations and examined whether or not this changed over the study period using a mixed effects linear model with a log it-transformed outcome and the same set of independent variables listed above. This addresses the question of whether fewer physicians taking on out-of-office care is offset by increases in the amount of out-of-office provision by those physicians who do provide those services.
All analyses were completed using SAS version 9.2 (SAS Institute, Inc).
RESULTS
We included 6,531 primary care physicians who received clinical service payments in at least 1 study year (Table 1). A total of 38% (n = 2,449) of the physicians self-identified as women, and 30% (n = 1,913) trained internationally. In 2011-2012, physicians were on average aged 51 years, and 16% (n = 871) of those who were active practiced in a rural area.
Physician Demographics
Eighty-five percent of physicians provided services in at least 1 alternative location in at least 1 study year. A majority of physicians provided at least 1: home visit (56%); long-term care facility visit (56%); emergency department visit (51%); and non-emergency department hospital visit (78%) at some point during the study period. Most (64%) were paid for urgent after-hours services, and 42% participated in an on-call arrangement. Physicians located in rural areas were more likely to provide care at all alternative locations and after hours.
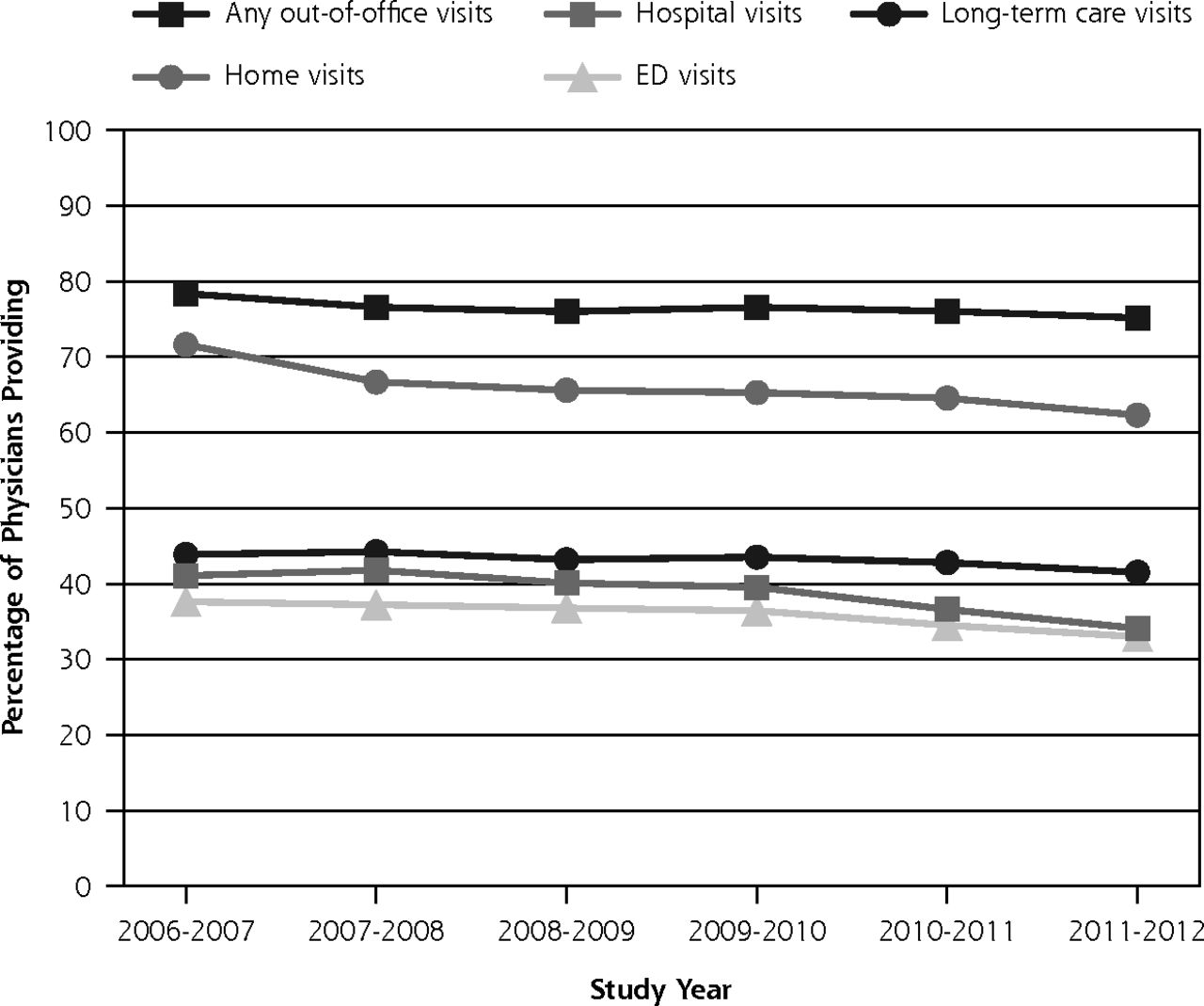
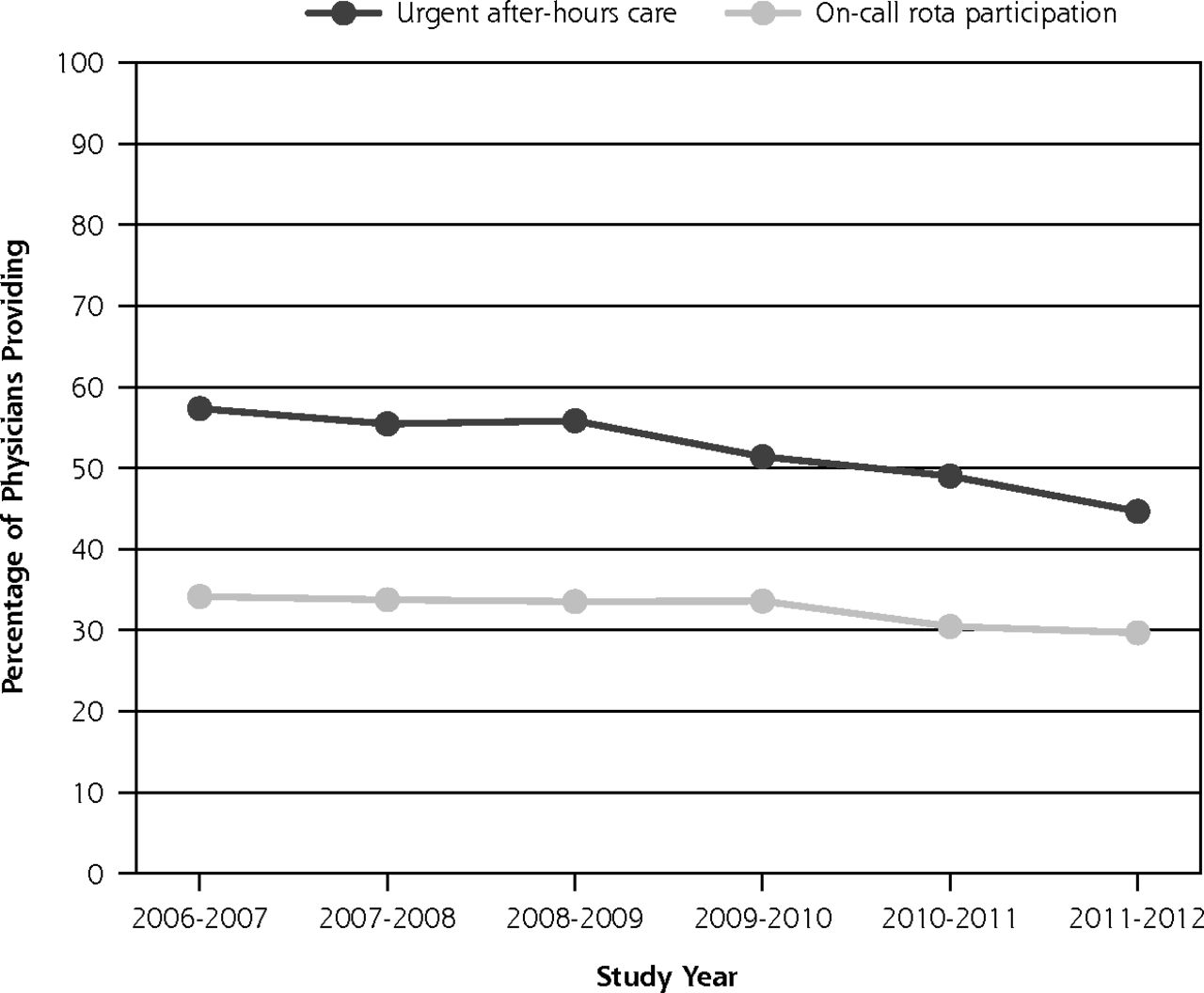
Care provided out-of-office and after-hours declined over the study period (Figures 1 and 2). Declines ranged from 5% for visits to long-term care facilities to 22% for the provision of urgent after-hours care.

Percentage of cohort providing home, long-term care, hospital, or emergency department visits by study year.
ED = emergency department.

Percentage of cohort providing after-hours care and on-call support by year.
Note: Locations included patients’ homes, long-term care facilities, emergency departments and acute-care hospitals, diagnostic facilities, mental health centers, community location (eg, school), or other.
Multivariate Results
Payment for Care Provided in Alternative Locations
Adjusting for physician demographic and patient factors, care provided at home, hospital, and emergency departments declined over the study period in all practice areas, while care provided at long-term care facilities declined in urban areas only. The proportion of physicians’ care provided at alternative locations declined in urban and metropolitan areas but did not change in rural areas (Supplemental Table 1, available at http://www.AnnFamMed.org/content/17/2/116/suppl/DC1/.)
Across all areas, female physicians had significantly lower odds of providing out-of-office care in patient homes, long-term care facilities, emergency departments, hospitals, or overall (Table 2). Physicians in successively older age strata had lower odds of providing emergency department visits and hospital visits, and those aged over 65 years had lower odds of providing home and long-term care facility visits. Compared with physicians aged younger than 35 years, physicians aged 35 to <65 years had higher odds of providing home visits. Training location did not appear to affect the odds of providing home, long-term care facility, or hospital visits; however, physicians who trained outside of Canada had higher odds of providing emergency department visits, and out-of-office care overall, but only in rural areas.
Logistic Modeling Results for the Provision of Out-of-Office Care
The characteristics of primary care physicians’ patient populations were influential predictors of care provided in alternative locations. Physicians whose practices included a larger proportion of contacts with female patients had higher odds of providing care at any out-of-office location and at homes, long-term care facilities, emergency departments (in rural areas only), and hospitals. Physicians whose practices included more visits with patients aged over 65 years had higher odds of providing care at home, long-term care facilities, and hospitals but had lower odds of providing care in emergency departments. Physicians who saw a higher proportion of chronically ill patients had higher odds of providing care in emergency departments and hospitals across all areas, higher odds of providing care in long-term care facilities in urban areas only, and lower odds of providing home visits in rural and metropolitan areas. Physicians whose practices included a larger proportion of visits with individuals in the lowest neighborhood socioeconomic status quintile had lower odds of providing care in hospitals, long-term care facilities, homes, and emergency departments in rural and metropolitan areas but not in urban areas.
Urgent After-Hours Care
The proportion of physicians who received payment for urgent after-hours care or for participation in on-call rota declined significantly over the study period across all areas (Table 3). Female physicians were less likely to provide urgent after-hours care or participate in on-call rota. Physicians in successively older age categories also had lower odds of on-call rota participation, and those aged 55 years and older had lower odds of providing urgent after-hours care. Internationally trained physicians had lower odds of providing urgent after-hours care compared with those trained in Canada, but only in metropolitan areas. They had higher odds of participating in on-call rota in rural and urban areas.
Logistic Modeling Results for the Provision of After-hours Care and On-call Participation
Physicians whose practices included a larger proportion of contacts with female patients had lower odds of providing after-hours care across all areas, and higher odds of participating in on-call rota but only in metropolitan areas. Physicians who saw more individuals aged over 65 years had higher odds of providing urgent after-hours care across all areas, and also on-call rota participation but only in metropolitan areas. Physicians whose practices included a larger proportion of patients with chronic illness had higher odds of providing urgent after-hours care and participating in on-call rota. Those who saw more individuals in the lowest socioeconomic status neighborhood quintile had significantly lower odds of providing after-hours care in rural and metropolitan areas, and higher odds of on-call participation in urban areas.
DISCUSSION
The provision of care in alternative locations or after hours, and participation in on-call rota declined in BC from 2006 through 2012. The decline of care provided in patient homes and long-term care facilities is of particular concern given that an increasing proportion of the population will be moving into age groups where visits in these locations is important for quality primary care. It is also of note that these declines occurred in the context of substantial financial incentives.12
Female physicians and those in the oldest age category (aged ≥65 years) were less likely to provide services at the 4 alternative locations. These results point to increasing accessibility challenges in the future, and are of concern for other jurisdictions (such as the United States) where physician demographics are shifting.15,28,29 Additionally, physicians whose practices included relatively high proportions of contacts with individuals in the lowest neighborhood socioeconomic status quintile were significantly less likely to provide care in alternative locations or after hours. This trend may reflect the fact that patients living in lower income areas are more likely to attend care at strict fee-for-service clinics rather than team-based patient medical homes, the latter of which are more likely to offer after-hours access.30
The extent of the decline, as well as the sociodemographic predictors of provision, varied by practice location, supporting existing literature on the substantial differences between rural and metropolitan practice, with rural primary care physicians providing a broader range of clinical care.27,31,32 This may be the result of either necessity, desire, or both. The presence of hospitalist physicians in metropolitan and some urban areas may explain differences between rural, urban, and metropolitan areas in terms of care provided in emergency departments and inpatient facilities. In the absence of hospitalists, there is a larger need for rural-based physicians to provide these services. Alternatively, it’s possible that the reduction of participation in care provision in hospitals led to an increase in the number of hospitalist physicians hired in some areas.
The model, style, and scope of practice of individual physicians is multifactorial and dependent on a host of structural, system, organization, and personal factors such as geography, remuneration, resource availability, training, intentions, and others.33 An exploration of the rationale for why physicians choose to provide out-of-office or after-hours services is beyond the scope of this analysis but should be the subject of future research. It is increasingly clear that financial incentives will not produce desired outcomes,12,34 so understanding decision-making and practice-style choices must inform future policy innovations.
One limitation of this study is that we were only able to extend the analysis to the end of the 2011-2012 fiscal year to capture non-fee-for-service and on-call payment data. We are not aware, however, of any significant policy, payment, or workforce demographic shifts that occurred following the end of our study period that would have altered the trends we observed here.
Our measure of after-hours care is necessarily incomplete, reflecting only specific financial incentives provided for urgent care provision. We were unable to measure standard clinic operations that occur outside of regular business hours as these are not uniquely identified within the payment data. Furthermore, the central on-call reimbursement program has been designed to pay physicians to be available to respond to emergency care needs of patients other than their own, and some physicians have raised concerns about confusion in how to access those payments.35 Lastly, throughout this paper we have been referring to service provision using underlying payment data. Physician services are fully publicly covered in BC and submitted claims for care provision are rarely permanently rejected; instead, they may be temporarily declined due to billing errors, and then subsequently accepted upon correction. Therefore, we expect that any difference between payment and provision is small and would create random noise in the data rather than bias.
Provision of primary care services outside of physicians’ offices and regular office hours declined in BC across rural, urban, and metropolitan areas during our study period. This trend points to increasing primary care accessibility challenges in future, both within Canada and elsewhere.
Acknowledgments
All inferences, opinions, and conclusions drawn in this manuscript are those of the authors, and do not reflect the opinions or policies of the Data Stewards. We obtained ethics approval for this study from the University of British Columbia Behavioral Research Ethics Board.
Footnotes
Conflicts of interest: authors report none.
Funding support: This study was supported by a Canadian Institutes of Health Research Doctoral Fellowship Award. Dr Law received salary support through a Canada Research Chair in Access to Medicines and a Michael Smith Foundation for Health Research Scholar Award.
Supplemental Materials: Available at http://www.AnnFamMed.org/content/17/2/116/suppl/DC1/.
- Received for publication April 3, 2018.
- Revision received October 23, 2018.
- Accepted for publication December 17, 2018.
- © 2019 Annals of Family Medicine, Inc.
References




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Changes in comprehensiveness of services delivered by Canadian family physicians: Analysis of population-based linked data in 4 provinces
- Characteristics and practice patterns of family physicians who provide home visits in Ontario, Canada: a cross-sectional study
- Declining Comprehensiveness of Services Delivered by Canadian Family Physicians Is Not Driven by Early-Career Physicians
- In This Issue: Minding the Gaps