
Article Figures & Data
Figures
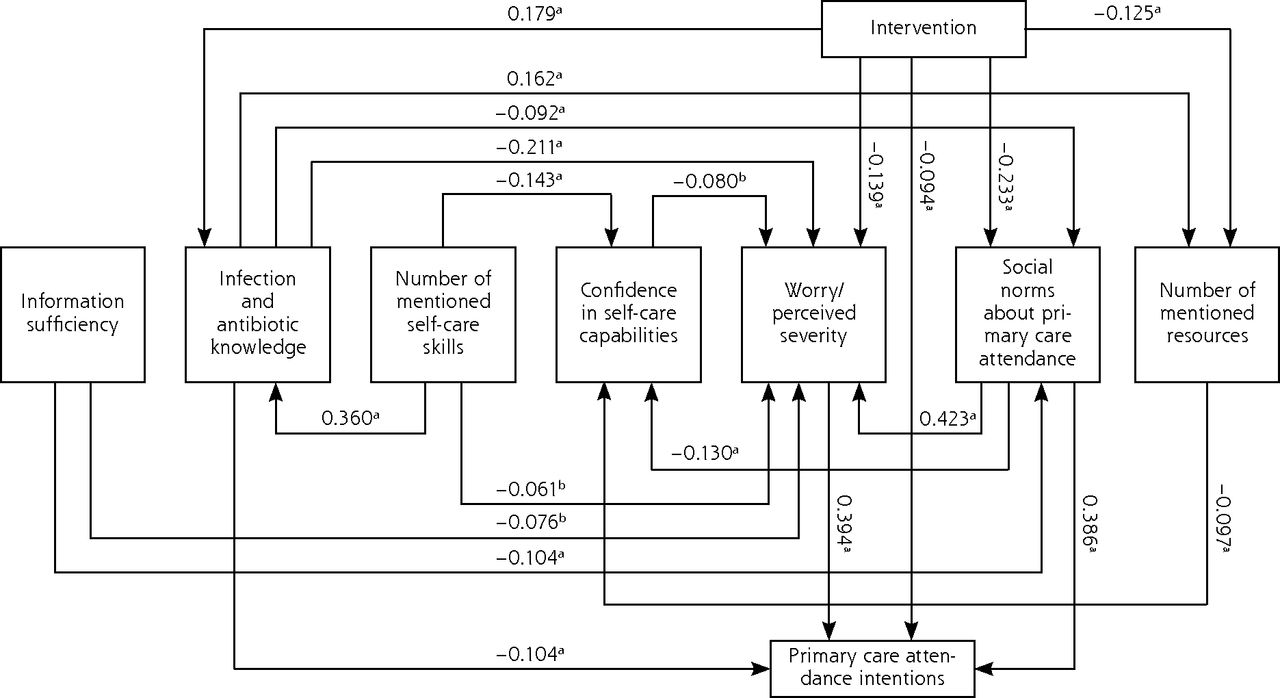
- Figure 1
Standardized estimates for the adjusted intervention path model.
Not statistically significant effects and residual error terms are omitted for ease of interpretation
aP <.01
bP <.05
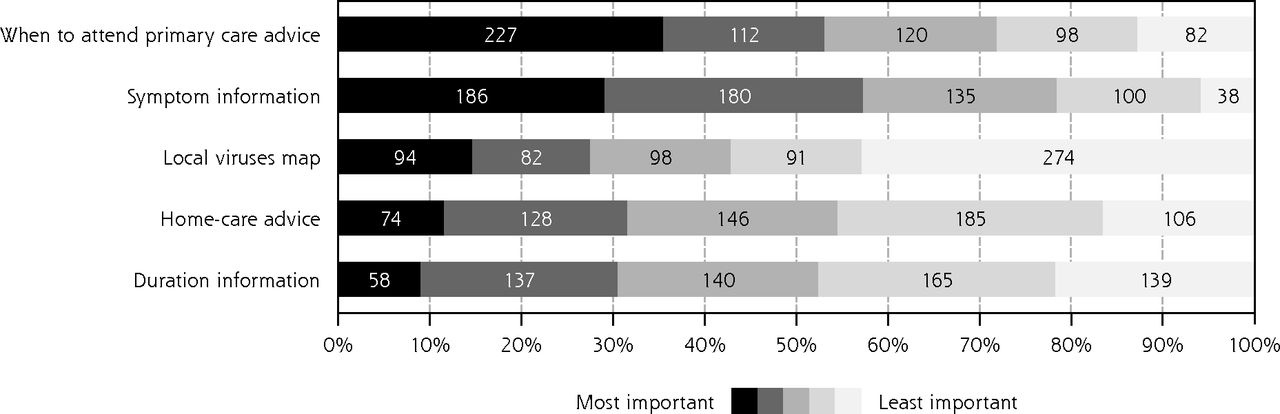
- Figure 2
Information components included in the intervention rated by perceived importance.


Tables
Target Construct/Scalea Items Answer Format Reliability (Cronbach’s α) Main outcome Intentions–primary care attendance intentions29,31–35 I want to visit a GP today/I intend to visit a GP today.b 5-point scale 0.94 Potential mediating factors Social influence-social norms about primary care attendance31,32,35 People around me think I need to visit a GP today/approve of me visiting a GP today/think I do not need to visit a GP today.b 5-point scale 0.81 Emotions-worry/perceived severity of a health threat36 Would you say that your child’s symptoms, as described in the illness scenario, suggest that the illness is severe/serious/significant/worrying/normal (given where I live and time of year)?b 5-point scale 0.84 Knowledge-information sufficiency37,38 How much do you think you currently know about the illness as described in the scenario? Scale of 0 to 100 … How much knowledge would you need to adequately care for your child showing the described symptoms? You might feel you need the same/more/less, information about the topic. Scale of 0 to 100 … What additional information would you need to adequately care for your child showing the described symptoms? Please describe. Open-ended question … Knowledge/skills/resources-viral illness knowledge and home-care test29 Thinking about the illness scenario, do you think the cause of your child’s symptoms is a viral infection/bacterial infection? True/False/I don’t know … Approximately how long do you think the symptoms of illness (fever/high temperature/sore throat/cough) in your child could last, from start to finish without any antibiotics? Estimation in days … How would you care for your child at home? Strategies and further resources? Open-ended question … Reflective motivation-beliefs about home-care capabilities39 When my child shows the symptoms described in the scenario, I feel confident about looking after them at home/taking their temperature/seeing if they need more fluids/checking for a rash/seeking advice from online resources/seeking advice or help from family and friends/seeking advice or help from health care professionals. 5-point scale 0.81 Knowledge/beliefs-antibiotic use40–42 Are most cold, cough, and flu illnesses caused by bacteria or viruses? Multiple choice … Are antibiotics helpful in treating bacterial infections, viral infection, or both? Multiple choice … How often are antibiotics needed for cough or bronchitis/sore throat/fever/earache/tiredness and aching/vomiting? 5-point scale … If my child does not receive an antibiotic for cold, cough, and flu symptoms, they will be sick for a longer time. 5-point scale … Intervention material feedback Clarity43 Not at all understandable/very understandable 7-point scale 0.93 Not at all comprehensible/very comprehensible Does not make sense/makes sense Confusing arguments/clear arguments Unclear information presented/clear information presented Credibility43 Credible information presented/information presented not credibleb 7-point scale 0.85 Valid claims/invalid claimsb Presented accurate information/did not present accurate informationb Cognitive challenge43 Not intellectually stimulating/intellectually stimulating 7-point scale 0.70 Not intellectually engaging/intellectually engaging Would make people think/would not make people thinkb Not at all thought-provoking/thought-provoking Did not really make me think/really made me think Emotional arousal44 Powerful impact/weak impactb 7-point scale 0.87 Emotional/unemotionalb Involving/uninvolvingb Boring/exciting Arousing/not arousingb Stimulating/not stimulatingb Strong visuals/weak visualsb Novelty44 Unique/commonb 7-point scale 0.72 Novel/ordinaryb Unusual/usualb Characteristics Total Sample (N = 806), No. (%) Intervention Group (n = 403), No. (%) Control Group (n = 403), No. (%) Mother Age, y 18–29 145 (18.0) 74 (18.4) 71 (17.6) 30–39 412 (51.1) 208 (51.6) 204 (50.6) 40–65 249 (30.9) 121 (30.0) 128 (31.8) Region Northern England 235 (29.2) 123 (30.5) 112 (27.8) Southern England 223 (27.7) 115 (28.5) 108 (26.8) Midlands 139 (17.2) 75 (18.6) 64 (15.9) Greater London 135 (16.7) 56 (13.9) 79 (19.6) East of England 74 (9.2) 34 (8.4) 40 (9.9) Employment status Employed 578 (71.7) 285 (70.7) 293 (72.7) Full-time parent/homemaker 182 (22.6) 93 (23.1) 89 (22.1) Unemployed 36 (4.5) 22 (5.5) 14 (3.5) Student/pupil 8 (1.0) 1 (0.2) 7 (1.7) Retired 2 (0.2) 2 (0.5) 0 (0.0) Education No official qualification 15 (1.9) 6 (1.5) 9 (2.2) School-leaving qualification 387 (48) 205 (50.9) 182 (45.2) University qualification 404 (50.1) 192 (47.6) 212 (52.6) Ethnicity White 681 (84.5) 347 (86.1) 334 (82.9) Asian 67 (8.3) 31 (7.7) 36 (8.9) Black 27 (3.3) 11 (2.7) 16 (4.0) Mixed 5 (0.6) 10 (2.5) 12 (3.0) Rather not answer 5 (0.6) 2 (0.5) 3 (0.7) Other group 4 (0.5) 2 (0.5) 2 (0.5) Caregiving role for youngest child Primary caregiver 566 (70.2) 282 (70.0) 284 (70.5) Shared caregiving role 240 (29.8) 121 (30.0) 119 (29.5) Youngest child Sex Boy 388 (48.1) 191 (47.4) 197 (48.9) Girl 418 (51.9) 212 (52.6) 206 (51.1) Age, y 0.25–4 282 (35.0) 140 (34.7) 142 (35.2) 5–8 276 (34.2) 148 (36.7) 128 (31.8) 9–12 248 (30.8) 115 (28.5) 133 (33.0) Primary care visits in past year 0 191 (23.7) 94 (23.3) 97 (24.1) 1 250 (31.0) 136 (33.7) 114 (28.3) 2 185 (23.0) 89 (22.1) 96 (23.8) >3 180 (22.3) 84 (20.8) 96 (23.8) Chronic health issues No 724 (89.8) 366 (90.8) 358 (88.8) Yes 82 (10.2) 37 (9.2) 45 (11.2) - Table 3
Bootstrapped Multiple Regression Model Summary Predicting Primary Care Attendance Intentions
Parameter B (95% CI) SE P Value Intercept 9.21 (7.23 to 11.11) 1.05 .001a Intervention −1.62 (−1.97 to −1.30) 0.18 .001a Demographics Age −0.01 (−0.04 to 0.02) 0.01 .408 Region Northern England 1 [Reference] … … Southern England 0.09 (−0.34 to 0.53) 0.23 .711 Midlands −0.27 (−0.82 to 0.24) 0.27 .310 Greater London 0.66 (0.17 to 1.10) 0.24 .001a East of England 0.07 (−0.58 to 0.71) 0.32 .858 Employment status Employed 1 [Reference] … … Full-time parent/homemaker −0.09 (−0.53 to 0.32) 0.22 .663 Unemployed 0.57 (−0.20 to 1.27) 0.40 .150 Student/pupil 0.52 (−0.49 to 1.55) 0.54 .32 Retired 0.29 (−0.88 to 1.43) 0.57 .628 Education No official qualification 1 [Reference] … … School-leaving qualification −0.32 (−1.74 to 1.10) 0.71 .636 University qualification −0.38 (−1.78 to 1.04) 0.72 .581 Ethnicity White 1 [Reference] … … Asian 0.85 (0.30 to 1.32) 0.24 .002b Black −1.98 (−2.80 to −1.09) 0.41 .001a Mixed −0.64 (−1.76 to 0.50) 0.59 .273 Caregiver role 0.30 (−0.11 to 0.72) 0.19 .117 Sex of youngest child 0.03 (−0.30 to 0.38) 0.17 .864 Age of youngest child −0.08 (−0.14 to −0.02) 0.03 .011c Clinical characteristics GP visits with youngest child in past year 0.10 (0.01 to 0.23) 0.06 .083 Chronic health issues of youngest child −0.20 (−0.75 to 0.37) 0.28 .471 - Table 4
Bootstrapped Effects of the Intervention on Mediating Factors and Primary Care Attendance Intentions
Intervention Effects B (95% CI) SE P Value Direct effects Infection and antibiotic knowledge 0.18 (0.12 to 0.24) 0.03 .002a Worry/perceived severity −0.14 (−0.20 to −0.08) 0.03 .002a Social norms concerning primary care attendance −0.23 (−0.30 to −0.17) 0.03 .002a Number of mentioned resources −0.13 (−0.19 to −0.06) 0.03 .002a Primary care attendance intentions −0.09 (−0.14 to −0.04) 0.03 .003a Indirect effects Confidence in home-care capabilities 0.04 (0.01 to 0.07) 0.02 .008a Worry/perceived severity −0.15 (−0.19 to −0.11) 0.02 .002a Social norms concerning primary care attendance −0.02 (−0.04 to −0.01) 0.01 .003a Number of mentioned resources 0.03 (0.02 to 0.05) 0.01 .001b Primary care attendance intentions −0.23 (−0.28 to −0.18) 0.03 .002a
Supplemental Appendixes 1-4
PDF file
Files in this Data Supplement:
- Supplemental data: Appendixes 1-4 - PDF file
- Supplemental data: Appendixes 1-4 - PDF file
The Article in Brief
Reducing Primary Care Attendance Intentions for Pediatric Respiratory Tract Infections
Annegret Schneider , and colleagues
Background Respiratory tract infections are a common reason that children visit a primary care clinician, yet such visits are costly, time-consuming and can lead to unnecessary antibiotic prescribing. This study examines whether providing mothers with actionable information can reduce their intentions to visit primary care for their children's respiratory tract infections.
What This Study Found An online intervention with real-time information on locally circulating viruses may reduce mothers� intentions to visit their primary care doctor. A representative sample of mothers in the United Kingdom (N = 806) was randomized to receive the online intervention, including locally enhanced influenza statistics, symptom information, and home-care advice, either before (intervention group) or after (control group) responding to a hypothetical respiratory tract infection illness scenario. Participants in the intervention group had lower intentions to visit the doctor than those in the control group when adjusted for demographic and clinical characteristics. Intervention material was generally well received, with information on symptoms and when to visit the primary care doctor rated as more important than information on locally circulating viruses.
Implications
- If the intervention were rolled out widely, the authors surmise that it would have impact, given the high rates at which parents of children with respiratory tract infections visit primary care clinicians..
- The authors call for research to evaluate intervention effects on observed behavioral outcomes in real-world settings and examine long-term effects and cost-effectiveness




{kind=link}
{kind=link}