
Article Figures & Data
Figures
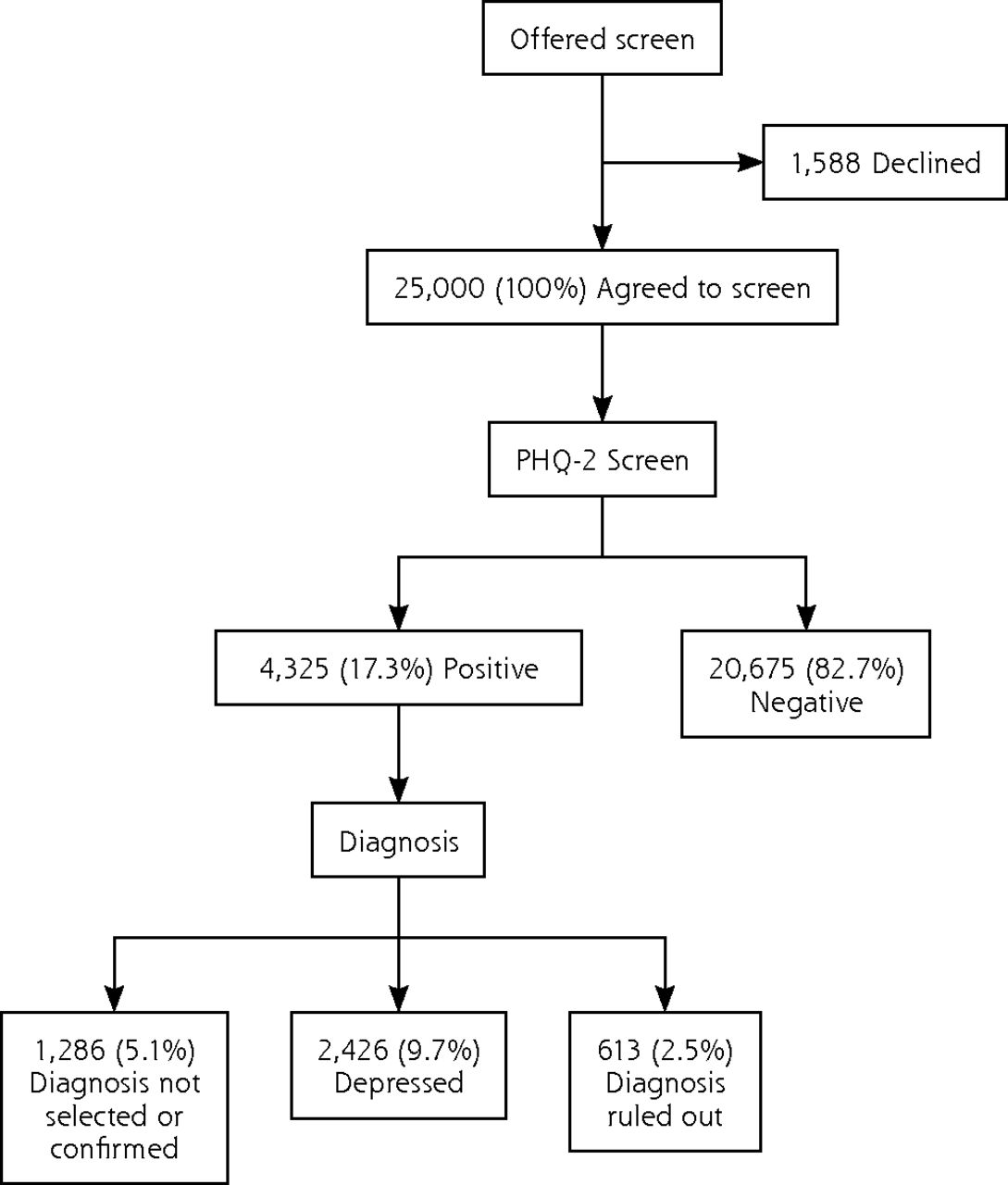
- Figure 1
Rates of positive screen and diagnosis of depression in primary care patients.
PHQ-2 = Patient Health Questionnaire 2-item scale.
Note: PHQ-2 positive was defined as a PHQ-2 score >2. Patients who were diagnosed with either major depressive disorder, adjustment disorder with depression, persistent depressive disorder, or unspecified depressive disorder were grouped as depressed.
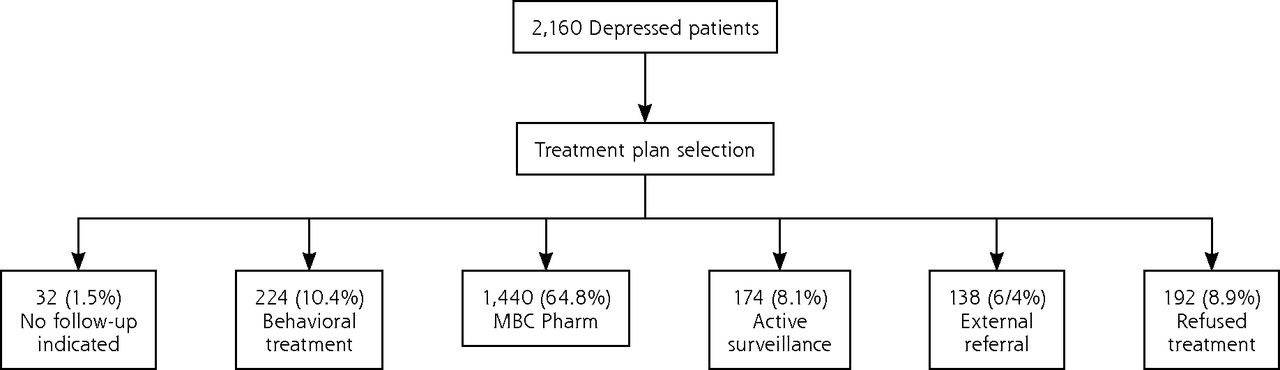
- Figure 2
Selection of treatment plan for depressed outpatients enrolled for at least 18 weeks of study.
MBC Pharm = Pharmacotherapy prescribed by the primary care provider using measurement-based care approach.
Note: Treatment was selected by the primary care providers for depressed patients diagnosed as having either major depressive disorder, adjustment disorder with depression, persistent depressive disorder, or unspecified depressive disorder.
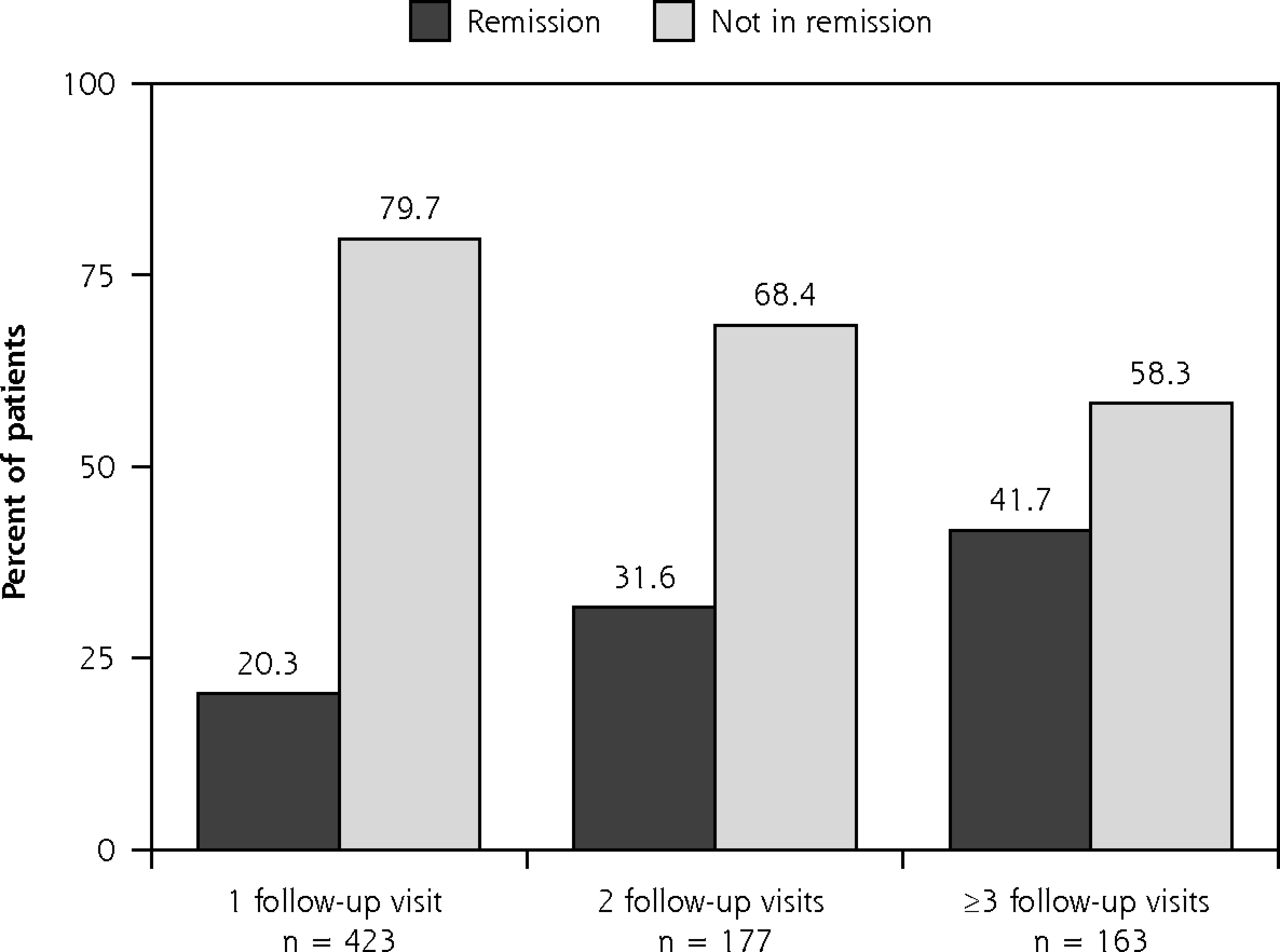
- Figure 3
Outcomes of depressed patients treated with pharmacotherapy with any follow-up visits.
Note: Remission was defined as a score of <5 on the Patient Health Questionnaire 9-item scale.


Tables
Characteristics Total (n = 25,000), No. PHQ-2 Negative (n = 20,675), No. (%) PHQ-2 Positive (n = 4,325), No. (%) Positive vs Negative Missing Data, No. χ2 (df) P Value Sex 8.98 (1) 0.003 9,115 Female 11,266 9,199 (81.65) 2,067 (18.35) Male 4,619 3,864 (83.65) 755 (16.35) Language 229.05 (1) <.001 0 English 11,770 9,282 (78.86) 2,488 (21.14) Spanish 13,230 11,393 (86.11) 1,837 (13.89) Race 149.39 (3) <.001 17,942 African American 892 631 (70.74) 261 (29.26) White 3,142 2,449 (77.94) 693 (22.06) American Indian or Native Alaskan 312 228 (73.08) 84 (26.92) Other 2,712 2,359 (86.98) 353 (13.02) Ethnicity 115.75 (1) <.001 17,724 (70.9) Hispanic 5,911 4,911 (83.08) 1,000 (16.92) Non-Hispanic 1,365 960 (70.33) 405 (29.67) PHQ-2 = Patient Health Questionnaire 2-item scale; df = degrees of freedom.
Notes: PHQ-2 positive was defined as a PHQ-2 score >2.
- Table 2
Baseline Characteristics of PHQ-2 Positive Patients by Depression Severity (N = 4,235)
Characteristic Depression Severity Missing Data, No. Minimal (n = 167), No. (%) Mild (n = 971), No. (%) Moderate (n = 1,257), No. (%) Moderately Severe (n = 1,084), No. (%) Severe (n = 846), No. (%) Categorical variables Sex 1,503 Female 69 (3.3) 407 (19.7) 620 (30.0) 538 (26.0) 433 (21.0) Male 41 (5.4) 191 (25.3) 219 (29.0) 170 (22.5) 134 (17.8) Language 0 English 91 (3.7) 428 (17.2) 682 (27.4) 696 (28.0) 591 (23.7) Spanish 76 (4.1) 543 (29.6) 575 (31.3) 388 (21.1) 255 (13.9) Race 2,934 African American 18 (6.9) 45 (17.2) 71 (27.2) 64 (24.5) 63 (24.1) White 18 (2.6) 170 (24.5) 217 (31.3) 161 (23.2) 127 (21.1) American Indian or Native Alaskan 0 (0.0) 8 (9.5) 19 (22.6) 26 (31.0) 31 (36.9) Other 20 (5.7) 90 (25.5) 108 (30.6) 76 (21.5) 59 (16.7) Ethnicity 2,920 Hispanic 30 (3.0) 240 (24.0) 317 (31.7) 227 (22.7) 186 (18.6) Non-Hispanic 16 (4.0) 64 (15.8) 103 (25.4) 110 (27.2) 112 (27.7) Diagnosis 0 Major depressive disorder 2 (0.1) 184 (9.8) 499 (26.5) 628 (33.3) 571 (30.3) Adjustment disorder with depression 1 (0.7) 52 (37.7) 47 (34.1) 24 (17.4) 14 (10.1) Persistent depressive disorder 0 (0.0) 11 (18.0) 23 (37.7) 13 (21.3) 14 (23.0) Unspecified depressive disorder 0 (0.0) 84 (24.5) 132 (38.5) 94 (27.4) 33 (9.6) No psychiatric disorder 82 (19.3) 206 (48.6) 96 (22.6) 29 (6.8) 11 (2.6) Other psychiatric disorder 3 (1.6) 36 (19.1) 55 (29.1) 56 (29.6) 39 (20.6) No diagnosis selected 75 (24.7) 65 (21.4) 51 (16.8) 65 (21.4) 48 (15.8) Unable to confirm 3 (0.3) 320 (35.6) 329 (36.6) 149 (16.6) 97 (10.8) Currently in treatment 1 (1.2) 13 (15.5) 25 (29.8) 26 (31.0) 19 (22.6) Alcohol screen 2,102 Negative 64 (4.0) 369 (22.9) 465 (28.8) 382 (23.6) 335 (20.7) Positive 13 (2.1) 95 (15.6) 178 (29.3) 174 (28.6) 148 (24.4) Drug use screen 2,102 Negative 73 (3.9) 428 (22.8) 561 (29.9) 445 (23.7) 371 (19.7) Positive 4 (1.2) 36 (10.4) 82 (23.8) 111 (32.2) 112 (32.4) Continuous variables Mean (SD) Mean (SD) Mean (SD) Mean (SD) Mean (SD) PHQ-9 3.43 (0.5) 7.29 (1.4) 11.99 (1.4) 16.9 (1.4) 22.65 (2.1) 0 GAD-7 1.74 (2.8) 5.4 (4.1) 9.16 (4.6) 12.84 (4.8) 16.93 (4.1) 383 P-FIBS 5.47 (7.1) 11.11 (8.9) 13.64 (8.9) 16.41 (9.3) 19.03 (9.3) 2,019 Age 41.93 (17.8) 40.43 (15.6) 41.02 (15.1) 41.2 (14.7) 41.06 (13.9) 0 PHQ-2 = Patient Health Questionnaire 2-item; PHQ-9 = Patient Health Questionnaire 9-item; GAD-7 = generalized anxiety disorder 7-item scale; P-FIBS = pain frequency, intensity, and burden scale.
Notes: Severity of depression26 was defined using PHQ-9 as minimal (0-4), mild (5-9), moderate (10-14), moderately severe (15-19), and severe (20-27). Alcohol32 and drug use33 during the past year were screened with self-report measures.
Characteristic Follow-Up Visits, No. (%) Overall Follow-Up Visits: 0 vs ≥1 Missing Data, No. 0 (n = 1,123) 1 (n = 612) 2 (n = 225) ≥3 (n = 200) P Value χ2 P Value χ2 Categorical variables Sex 2.89 .41 0.15 .70 814 Female 524 (50.7) 274 (26.5) 113 (10.9) 123 (11.9) Male 162 (51.9) 91 (29.2) 25 (8.0) 34 (10.9) Language 0.98 .81 0.09 .76 0 English 683 (52.3) 375 (28.7) 130 (9.9) 119 (9.1) Spanish 440 (51.6) 237 (27.8) 95 (11.1) 81 (9.5) Race 39.68 <.001 22.73 <.001 1,471 African American 74 (49.3) 46 (30.7) 17 (11.3) 13 (8.7) White 168 (45.9) 93 (25.4) 57 (15.6) 48 (13.1) American Indian or Native Alaskan 20 (58.8) 10 (29.4) 0 (0.0) 4 (11.8) Other 96 (69.1) 33 (23.7) 8 (5.8) 2 (1.4) Ethnicity 3.42 .33 0.66 .42 1,436 Hispanic 233 (46.5) 123 (24.5) 67 (13.4) 78 (15.6) Non-Hispanic 111 (49.8) 62 (27.8) 23 (10.3) 27 (12.1) Alcohol screen 2.49 .48 0.02 .89 1,080 Negative 423 (53.3) 204 (25.7) 78 (9.8) 89 (11.2) Positive 151 (52.8) 75 (26.2) 21 (7.3) 39 (13.6) Drug screen 4.23 .24 3.91 .05 1,080 Negative 478 (51.9) 243 (26.4) 86 (9.3) 114 (12.4) Positive 96 (60.4) 36 (22.6) 13 (8.2) 14 (8.8) Follow-up 105.24 .0001 3.81 <.06 0 MBC Pharm T/t 637 (45.5) 423 (30.2) 177 (12.6) 163 (11.6) Behavioral T/t 142 (63.4) 44 (19.6) 16 (7.2) 22 (9.8) Active Surveillance 113 (64.9) 45 (25.9) 9 (5.2) 7 (4.0) No follow-up 27 (84.4) 3 (9.4) 2 (6.2) 0 (0.0) External Referral 94 (68.1) 37 (36.8) 4 (2.9) 3 (2.2) Refused T/t 110 (57.3) 60 (31.3) 17 (8.8) 5 (2.6) Continuous variables Mean (SD) Mean (SD) Mean (SD) Mean (SD) F P Value F P Value PHQ-9 15.33 (5.46) 15.82 (5.38) 16.76 (5.23) 17.15 (4.90) 9.46 <.001 25.45 <.001 0 GAD-7 11.93 (5.76) 11.98 (5.90) 12.74 (5.48) 13.7 (5.24) 6.15 <.001 10.73 .001 142 P-FIBS 16.5 (9.44) 15.81 (9.53) 17.67 (8.58) 14.98 (9.29) 1.94 .13 0.37 .55 1,044 Age 41.72 (14.78) 43.53 (14.58) 43.95 (12.56) 42.61 (13.04) 2.92 .04 6.12 .02 0 T/t = treatment; PHQ-9 = Patient Health Questionnaire 9-item; GAD-7 = generalized anxiety disorder 7 item scale; P-FIBS = pain frequency, intensity, and burden scale.
The F statistic is a ratio of variation among the group means to the total variation within the samples and large values of the statistic imply larger differences among the group means.
Supplemental Appendix
Supplemental Appendix
Files in this Data Supplement:
- Supplemental data - PDF file
The Article in Brief
A Structured Approach to Detecting and Treating Depression in Primacy Care: VitalSign6 Project
Madhukar H. Trivedi , and colleagues
Background Major Depressive Disorder affects 5-10% of adults in the United States every year. This report describes outcomes of an ongoing quality-improvement project in a large US metropolitan area to improve recognition, treatment, and outcomes of depressed patients in sixteen primary care clinics.
What This Study Found A questionnaire-based management algorithm for major depressive disorder in primary care is feasible to implement, though attrition from treatment is high. Among 25,000 patients in primary care clinics in a large metropolitan area, 4,325 (17%) screened positive for depression with 2,426 having a clinician-diagnosed depressive disorder. Of the 2,160 patients who had 18 weeks of follow-up care, 65% were treated with medication. Remission, defined as a PHQ-9 score of less than 5, was more common in patients who experienced 3 or more follow-up visits. Of those who returned for 3 or more visits, 41.7% achieved remission. However, more than one-half of those diagnosed did not return for any follow-up care.
Implications
- The findings of this study suggest that patients suffering from depression can be successfully treated using measurement-based care within the primary care setting, and stronger emphasis on patient education and other approaches to reduce attrition may be needed for patients who fail to return for follow-up care.
Visual Abstract
Files in this Data Supplement:
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.