
Article Figures & Data
Figures
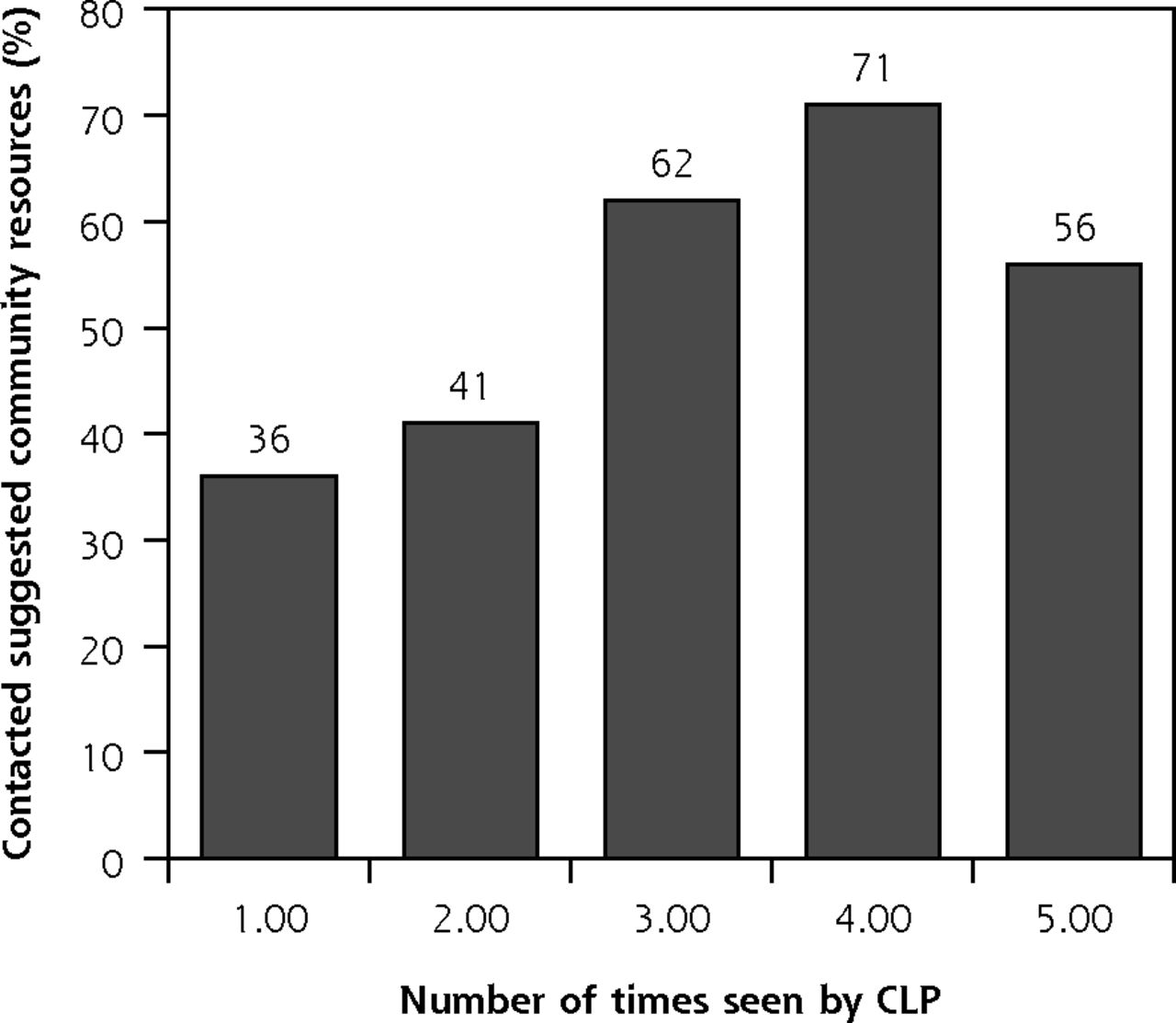
- Figure 1
Relationship between number of times seen by CLP and patient contact with suggested community resource.
CLP = community-links practitioner.
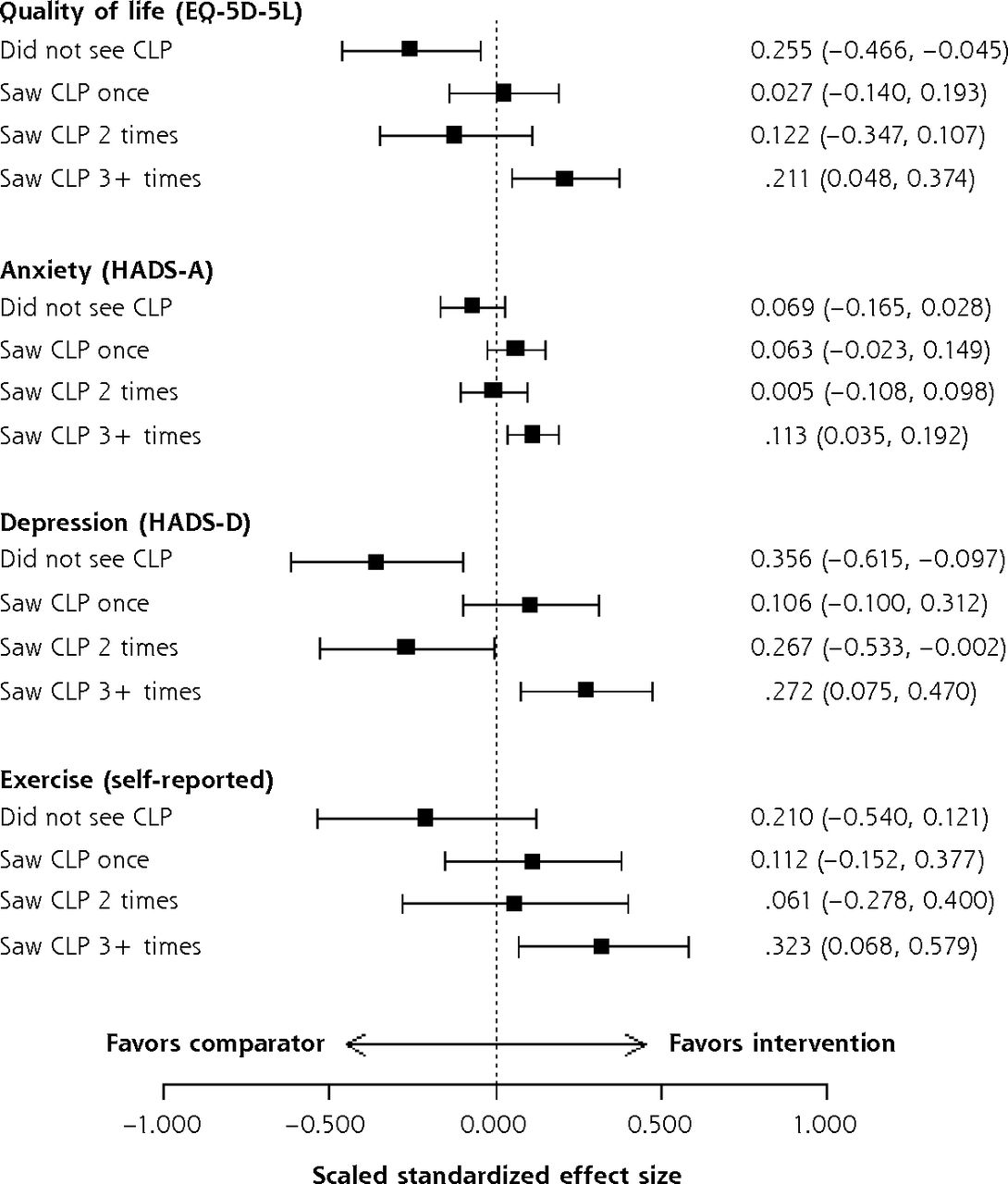
- Figure 2
Effect sizes of frequency of seeing a community-links practitioner on patient outcomes.
CLP = community-links practitioner; EQ-5D-5L = a standardized measure of self-reported health-related quality of life that assesses 5 dimensions at 5 levels of severity; HADS-A = Hospital Anxiety and Depression Scale, Anxiety; HADS-D = Hospital Anxiety and Depression Scale, Depression.


Tables
- Table 1
Description of the Glasgow Deep End Links Worker Program Using the TIDieR Framework12
Name The Glasgow Deep End Links Worker Program Purpose The development of the Glasgow Deep End LWP drew on the theory of community-oriented primary care13 and was based on a report by GPs working in the Deep End.14 Patients attending general practices in deprived areas commonly have multiple problems, many of which are not amenable to medical intervention.
Community organizations offer a wide range of resources, but people in deprived areas with multiple health and social problems can find it hard to access them. Closer links between general practices and community organizations, and support to access to available community resources, could mitigate the effects of deprivation.
Links between general practices and community organizations could be enhanced by adding a nonmedical CLP to the practice team. CLPs would operate from the general practice, forge relationships between general practices and community organizations, and support patients to access the nonmedical services and support on offer. CLPs would act as a catalyst to hope and self-determination, using the strong relationships with patients that exist in general practice. If patients with complex needs feel supported, they would be more likely to respond to information on ways to improve their health.Resources A practice-attached CLP with a previous working background in community development. The CLPs all had previous experience of working with individuals and community organizations and had skills in identifying assets, needs, opportunities, rights, and responsibilities. Management support for the program was provided by the CLPs’ employing organization, the Scottish Alliance for Health and Social Care (Scotland). Support included (1) an experienced program director, overseeing all aspects of the program including the production of detailed records of learninga; (2) a community links manager, with experience in community development and staff management, responsible for establishing protocols and polices for CLP work and line managing the CLPs; (3) a learning and evaluation officer, responsible for establishing local protocols for program monitoring (independent of the evaluation conducted by the research team); (4) administrative staff; and (5) a clinical lead.
A practice development fund (GBP £35,000) to spend on activities to help each practice develop the new LWP approach. The fund was used mainly to “buy time” away from clinical care to focus on the LWP.
The A Local Information System for Scotland (ALISS) website,b which allows individuals and community organizations to make real-time lists of sources of support searchable by locality.Procedures CLPs made links between practices and community organizations in the local area (eg, walking groups, debt management support, welfare rights, drug and alcohol management support, lunch clubs, befriending schemes, crafting clubs, bereavement support).
Practice staff used time away from clinical care to set up systems and learn more about services and support available in community organizations.
Each practice devised its own system for GPs and PNs to identify and refer patients who would benefit from help from a CLP who would link them to community-based resources. The system was devised jointly by clinical staff and CLPs and was customized for each practice. The choice of which patients to refer to the CLP was left open by practices but was based mainly on the presence of social problems that exacerbated long-term health problems.
CLPs met patients. CLPs elicited patients’ main needs and worked flexibly, making links with community organizations for patients and, if necessary, supporting patients to attend the organizations’ services. Services depended on patients’ needs, their enthusiasm to engage, and the availability of local services accessible to patients.
CLPs met together weekly with a manager to share and discuss experiences and problem solve collectively.Providers GPs and PNs referred patients who might benefit to CLPs.
CLPs saw patients and provided support to link patients to existing community organizations.How All contacts were one-to-one and usually face-to-face, although some telephone contacts could occur. Where CLP contacts with patients were usually in the practice, although some home visits could occur, and the CLPs could accompany patients to support their contact with a community organization. When and how much CLPs and patients could meet as many times, and when, they thought necessary. Tailoring The intervention was very flexible and dependent on patient needs, patient wants, and professionals’ judgments as to what help was needed. Modifications The intervention was not modified during the research. How well Given the flexibility of the intervention, we did not assess fidelity. CLP = community-links practitioner; GBP = Great Britain pound sterling; GP = general practitioner; LWP = Links Worker Programme; PN = practice nurse; TIDieR = Template for Intervention, Description, and Replication.
↵a https://www.alliance-scotland.org.uk/blog/resources/links-worker-programme-record-of-learning-series-1/.
Characteristic Intervention Comparison P Value Age, y 49 (16) 56 (15) <.001 Female, % 59.2 61.1 .61 Deprived,a % 79.3 58.1 <.001 Employed, % 24.1 48.7 <.001 Lives alone, % 67.5 45.9 <.001 Current smoker, % 45.2 20.4 <.001 Never exercises, % 58.0 31.0 <.001 Multimorbidity,b % 3.1 (2.1) 2.3 (1.8) <.001 Social problems,c % 3.9 (2.5) 1.8 (2.1) <.001 EQ-5D-5L 0.382 (0.337) 0.683 (0.300) <.001 ICECAP-A 0.563 (0.228) 0.812 (0.212) <.001 WASAS 22.3 (12.2) 9.4 (11.4) <.001 HADS-A >10,d % 71.7 29.0 <.001 HADS-D >10,e % 57.5 19.0 <.001 EQ-5D-5L = a standardized measure of self-reported health-related quality of life that assesses 5 dimensions at 5 levels of severity; HADS = Hospital Anxiety and Depression Scale; HADS-A = Hospital Anxiety and Depression Scale, Anxiety; HADS-D = Hospital Anxiety and Depression Scale, Depression; ICECAP-A = Investigating Choice Experiments for the Preferences of Older People Capability Measure for Adults; WASAS = Work and Social Adjustment Scale.
Note: Characteristics are either shown as mean (standard deviation) or percentages.
↵a Those in the top quintile of deprivation for Scotland as measured by the Scottish Index of Multiple Deprivation.
↵b The count of self-reported chronic conditions.
↵c The count of self-reported social problems.
↵d The HADS percentage scoring above 10 (likely case-ness) for anxiety.
↵e The HADS percentage scoring above 10 (likely case-ness) for depression symptoms.
Outcome Measure Intervention Group vs Comparison Group Adjusted Effect Estimate (95% CI) P Value EQ-5D-5L 0.008 (−0.028 to 0.045) .648 ICECAP-A −0.011 (−0.039 to 0.016) .411 WASAS 0.05 (−1.37 to 1.48) .940 HADS-A −0.41 (−0.99 to 0.18) .172 HADS-D 0.09 (−0.49 to 0.68) .753 Exercise 0.12 (−0.06 to 0.3) .183 EQ-5D-5L = a standardized measure of self-reported health-related quality of life that assesses 5 dimensions at 5 levels of severity; HADS-A = Hospital Anxiety and Depression Scale, Anxiety; HADS-D = Hospital Anxiety and Depression Scale, Depression; ICECAP-A = Investigating Choice Experiments for the Preferences of Older People Capability Measure for Adults; SIMD = Scottish Index of Multiple Deprivation; WASAS = Work and Social Adjustment Scale.
Note: Intention-to-treat analysis. Mixed effects regression models at follow-up in relation to intervention group. Effect estimates represent mean differences. Each model adjusts for age, sex, SIMD, comorbidity, and significant baseline outcome measures as covariates and includes practice identifier as a random effects term.
Outcome Measure Intervention Group vs Comparison Group CLP Variable Adjusted Effect Estimate (95% CI) P Value EQ-5D-5L Saw CLP once 0.009 (−0.047 to 0.065) .755 Saw CLP twice −0.041 (−0.117 to 0.036) .298 Saw CLP 3+ 0.071 (0.016 to 0.126) .011 ICECAP-A Saw CLP once 0.004 (−0.038 to 0.046) .841 Saw CLP twice −0.002 (−0.056 to 0.052) .938 Saw CLP 3+ 0.002 (−0.038 to 0.042) .909 WASAS Saw CLP once −1.097 (−3.361 to 1.168) .342 Saw CLP twice 1.146 (−1.766 to 4.058) .441 Saw CLP 3+ −0.795 (−3.042 to 1.452) .488 HADS-A Saw CLP once −0.768 (−1.815 to 0.278) .150 Saw CLP twice 0.064 (−1.194 to 1.322) .920 Saw CLP 3+ −1.380 (−2.339 to -0.421) .005 HADS-D Saw CLP once −0.497 (−1.465 to 0.471) .314 Saw CLP twice 1.256 (0.009 to 2.504) .048 Saw CLP 3+ −1.280 (−2.209 to –0.352) .007 Exercise Saw CLP once 0.118 (−0.159 to 0.396) .403 Saw CLP twice 0.064 (−0.292 to 0.420) .726 Saw CLP 3+ 0.339 (0.071 to 0.607) .013 CLP = community-links practitioner; EQ-5D-5L = a standardized measure of self-reported health-related quality of life that assesses 5 dimensions at 5 levels of severity; HADS-A = Hospital Anxiety and Depression Scale, Anxiety; HADS-D = Hospital Anxiety and Depression Scale, Depression; ICECAP-A = Investigating Choice Experiments for the Preferences of Older People Capability Measure for Adults; SIMD = Scottish Index of Multiple Deprivation; WASAS = Work and Social Adjustment Scale.
Note: Intention-to-treat analysis. Mixed effects regression models at follow-up in relation to intervention group. Effect estimates represent mean differences.
Each model adjusts for age, sex, SIMD, comorbidity, and baseline outcome level as covariates and includes practice identifier as a random effects term.
Supplemental Appendixes
Supplemental Appendixes
Files in this Data Supplement:
- Supplemental data: Appendixes - PDF file
The Article in Brief
Effectiveness of Community-Links Practitioners in Areas of High Socioeconomic Deprivation
Stewart W. Mercer , and colleagues
Background A common policy response to health inequalities in recent years has been the introduction of different social prescribing programs. However, the evidence base for the effectiveness of social prescribing is extremely limited.
What This Study Found The study assessed the efficacy of a Scottish government-funded program that was developed to target social determinants of health among some of the most socioeconomically vulnerable adults in Glasgow. In the program, "community-links practitioners" connected adult patients with community resources like exercise groups and drug and alcohol management support. The study evaluated the health-related quality of life, at baseline and after nine months, of 288 adults enrolled in the program. The authors compare their scores with 612 non-matched adults in comparison general practices and find no significant benefit in the intervention group. In a subgroup analysis, those who visited the practitioner three or more times showed improved quality of life, but many who enrolled did not fully utilize the program.
Implications
- The findings of this study call into question the effectiveness of such social prescribing programs for improving short-term health-related quality of life. Discovering ways to improve the uptake and engagement rates of the intervention may lead to better overall outcomes.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Cost of Dying Exhibition: public, professional and political reactions to a visual exhibition depicting experiences of poverty at the end of life
- Addressing unmet social needs using a health navigator for patients at a major metropolitan hospital in Australia: a mixed-methods feasibility study
- Equal, equitable or exacerbating inequalities? Patterns and predictors of social prescribing referrals in 160,128 UK patients
- Intervention Characteristics and Mechanisms and their Relationship with the Influence of Social Prescribing: a Systematic Review
- Health inequalities, multimorbidity and primary care in Scotland
- Non-pharmaceutical primary care interventions to improve mental health in deprived populations: a systematic review
- Developing a research agenda for social prescribing in the UK using lessons from the US
- Effect of social prescribing link workers on health outcomes and costs for adults in primary care and community settings: a systematic review
- Global developments in social prescribing
- Implementing social prescribing in primary care in areas of high socioeconomic deprivation: process evaluation of the 'Deep End community Links Worker Programme
- A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance
- Equity, a common goal for primary care
- Link workers providing social prescribing and health and social care coordination for people with multimorbidity in socially deprived areas (the LinkMM trial): protocol for a pragmatic randomised controlled trial
- Are the needs of people with multiple long-term conditions being met? Evidence from the 2018 General Practice Patient Survey
- Prevention in the 2020s: where is primary care?
- Community-Links Practitioners in Scotland