
Article Figures & Data
Figures
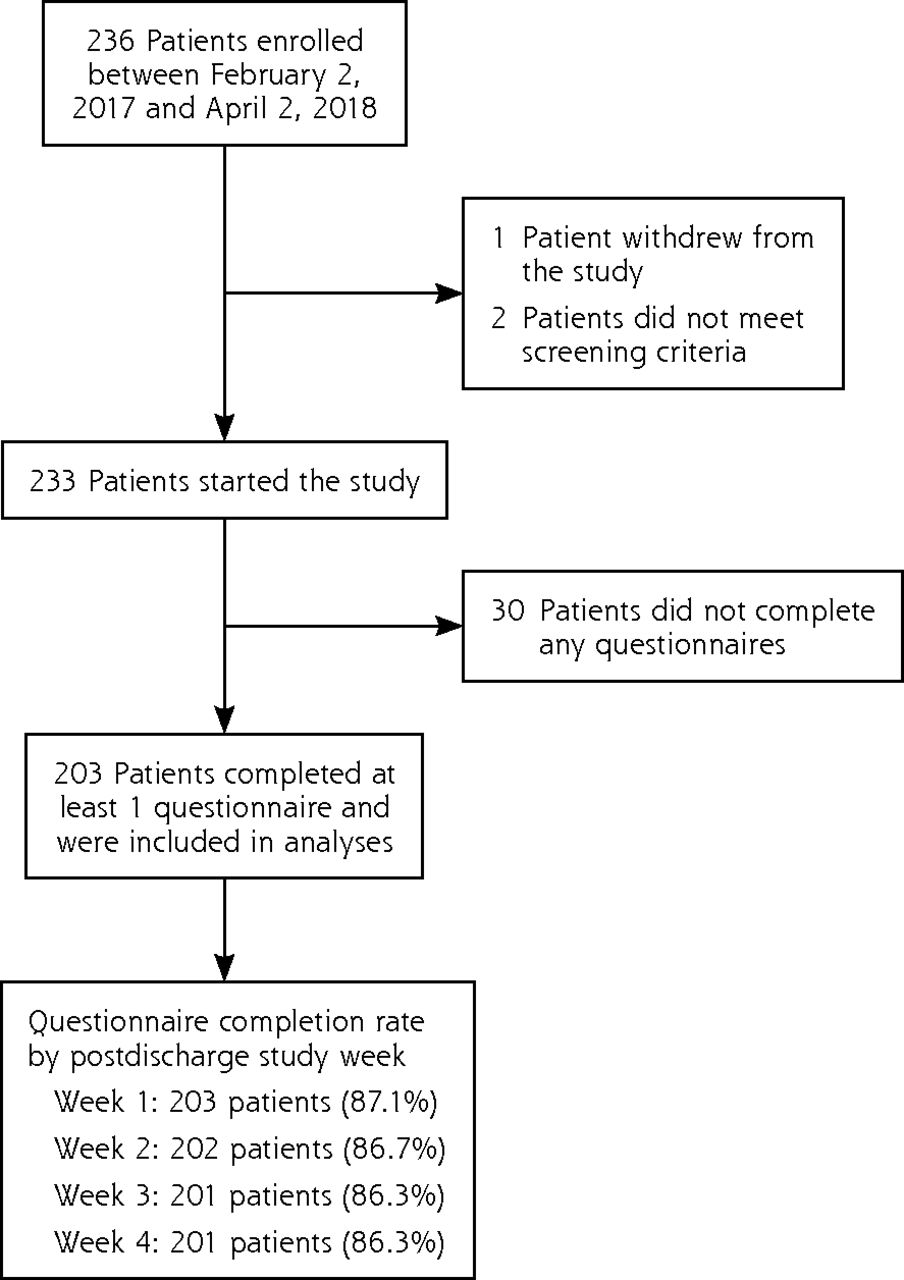
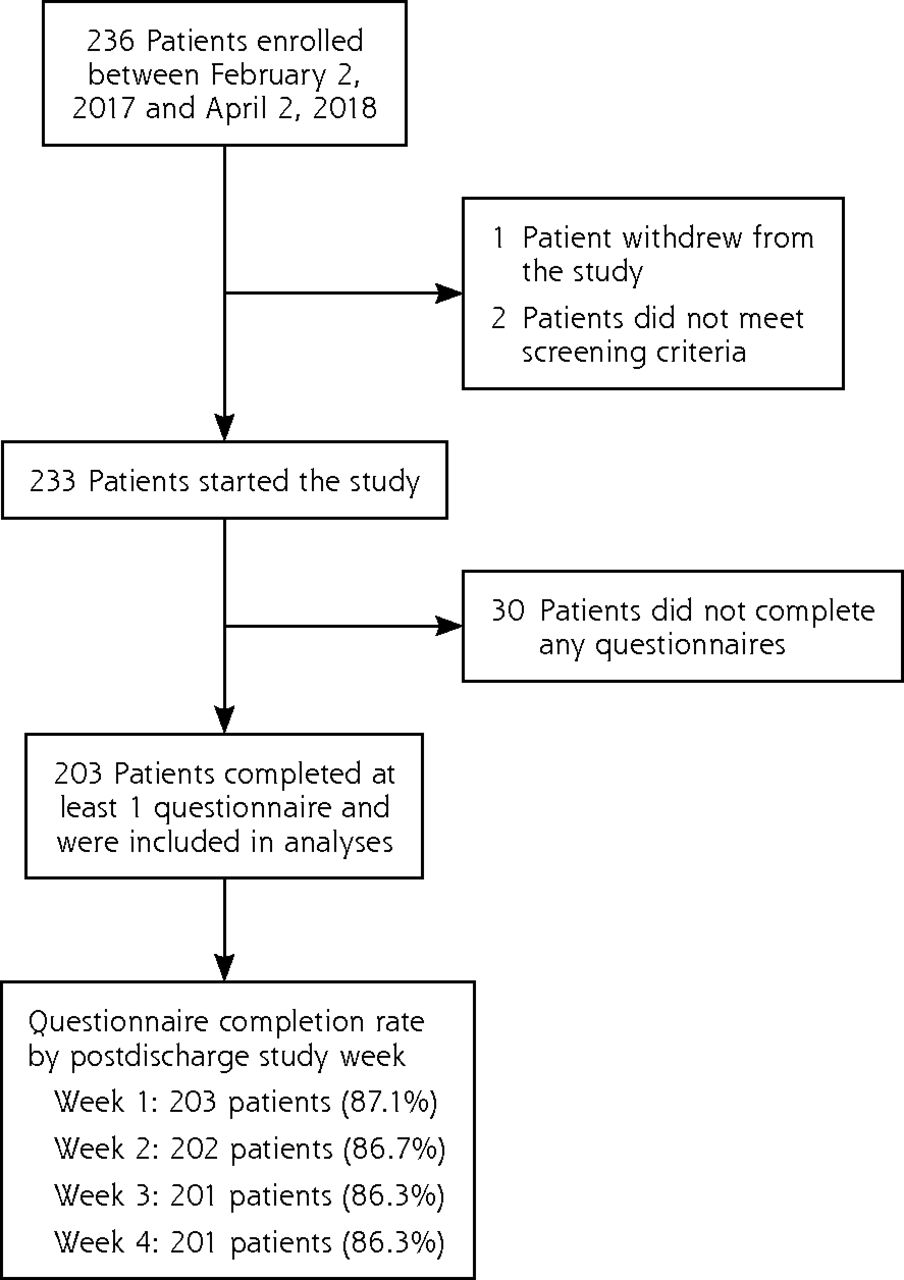
- Figure 1
Flow chart of study enrollment and follow-up.
Tables
- Table 1
Comparison of Patient, Procedural, and Perioperative Characteristics by Self-Reported Postdischarge Opioid Use (N = 203)
Characteristic Low Use (n = 90) High Use (n = 113) P Value Age, mean (SD) [median], y 32.4 (5.7) [32] 31.4 (5.3) [31] .22 Race, No. (%) .93 American Indian or Alaskan Native 2 (2.2) 0 (0) Asian 4 (4.4) 7 (6.2) Black or African American 8 (8.9) 5 (4.4) Native Hawaiian or other Pacific Islander 1 (1.1) 0 (0) White 65 (72.2) 81 (71.7) More than 1 race 3 (3.3) 6 (5.3) Other 7 (7.8) 12 (10.6) Unknown 0 (0) 2 (1.8) Would rather not answer 0 (0) 0 (0) Ethnicity, No. (%) .83 Hispanic 18 (20) 24 (21.2) Type of insurance, No. (%) .72 Medicare 0 (0) 0 (0) Medicaid 25 (27.8) 34 (30.1) Commercial insurer (Cigna, Aetna, Anthem, etc) 63 (70.0) 73 (64.6) Tri-Care or other government insurance 2 (2.2) 6 (5.3) Self-pay 0 (0) 0 (0) Other 0 (0) 0 (0) Unknown 0 (0) 0 (0) Preoperative opioid use, No. (%) <.02 Yes 0 (0) 5 (4.4) No 90 (100) 108 (95.6) Preoperative benzodiazepine use, No. (%) .87 Yes 1 (1.1) 1 (0.9) No 89 (98.9) 112 (99.1) ASA physical status class, No. (%)a .70 I 0 (0) 0 (0) II 69 (76.7) 84 (74.3) III 21 (23.3) 29 (25.7) IV 0 (0) 0 (0) V 0 (0) 0 (0) Emergency procedure, No. (%) .72 Yes 6 (6.7) 9 (8.0) No 84 (93.3) 104 (92.0) Surgery duration, mean (SD) [median], min 59.5 (25.0) [57.0] 55.7 (21.9) [51.0] .24 Cesarean order, No. (%) .83 Repeat 42 (46.7) 51 (45.1) Primary 48 (53.3) 62 (54.9) Associated procedure, No. (%) .90 Tubal ligation 18 (20.0) 18 (15.9) Salpingo-oophorectomy 5 (5.6) 11 (9.7) Hysterectomy 0 (0) 2 (1.8) Other 3 (3.3) 3 (2.7) None 67 (74.4) 85 (75.2) Opioids in 24 h before discharge, mean (SD) [median], MME 33.0 (28.5) [30] 59.3 (26.3) [60] <.001 Any acetaminophen in 24 h before discharge, No. (%) <.001 Yes 72 (80.0) 109 (96.5) No 18 (20) 4 (3.5) NSAIDs in 24 h before discharge, No. (%) .43 Yes 88 (97.8) 112 (99.1) No 2 (2.2) 1 (0.9) Gabapentin or pregabalin in 24 h before discharge, No. (%) .70 Yes 1 (1.1) 2 (1.8) No 89 (98.9) 111 (98.2) Discharge opioid prescribed, No. (%) .54 Oxycodone 15 (16.7) 19 (16.8) Acetaminophen-hydrocodone 2 (2.2) 5 (4.4) Acetaminophen-oxycodone 69 (76.7) 88 (77.9) Tramadol 0 (0) 1 (0.9) Other 0 (0) 0 (0) None 4 (4.4) 0 (0) Discharge opioid prescription amount, mean (SD) [median], MME 195.0 (117.8) [225.0] 216.8 (71.3) [225.0] .28 ASA = American Society of Anesthesiology; MME = morphine milligram equivalent; NSAID = non-steroidal anti-inflammatory drug.
a Higher class indicates poorer physical status.
Notes: Low use defined as ≤75 MMEs; high use defined as >75 MMEs. Comparisons of high vs low use groups were made with separate binomial regressions. Characteristics with multiple categorical variables were collapsed for statistical comparison as follows: race (white vs all other categories), type of insurance (Medicaid vs all other categories), ASA physical status (III vs II), associated procedure (any vs none), type of discharge opioid prescription (acetaminophen-hydrocodone and acetaminophen-oxycodone vs all other opioids).
- Table 2
Comparison of Patient-Reported Use of Opioids and OTC Analgesics, and Pain Over Time
Measure Week 1 (N = 203) Week 2 (N = 202) Week 3 (N = 201) Week 4 (N = 201) Interaction P Valuea Low Use (n = 90) High Use (n = 113) Low Use (n = 89) High Use (n = 113) Low Use (n = 89) High Use (n = 112) Low Use (n = 89) High Use (n = 112) Opioids taken, 20.1 146.0 2.7 32.1 0.93 21.6 0.93 15.9 .72b mean (SD) (23.9) (87.5) (6.6) (53.5) (3.5) (71.2) (3.9) (52.1) [median], MMEs [13.1] [140.0] [0] [7.5] [0] [0] [0] [0] Opioids left over, 102.8 74.6 94.2 57.0 89.4 56.7 83.3 54.1 .95 mean (SD) (114.4) (66.6) (108.9) (63.8) (103.9) (75.3) (103.0) (91.0) [median], MMEs [80.6] [60.0] [75.0] [37.5] [67.5] [30.0] [45.0] [15.0] OTC analgesics taken, No. (%) Acetaminophen 21 (23.3) 25 (22.1) 15 (16.9) 26 (23.0) 14 (15.7) 27 (24.1) 9 (10.1) 18 (16.1) .11 NSAIDs 57 (63.3) 72 (63.7) 51 (57.3)c 88 (77.9)c 35 (39.3)c 69 (61.6)c 26 (29.2)c 58 (51.8)c .03 Both 17 (18.9) 16 (14.2) 12 (13.5) 21 (18.6) 11 (12.4) 19 (17.0) 6 (6.7) 13 (11.6) .08 PROMIS pain, T score (SE)d Pain intensity 47.2 (5.6) 51.7 (5.7) 42.9 (6.5) 46.9 (6.6) 38.6 (6.6) 43.8 (7.4) 36.5 (6.6) 40.5 (7.1) .18b Pain interference 58.5 (6.8) 63.7 (6.1) 53.0 (7.4) 57.0 (7.5) 48.7 (7.7) 53.3 (8.2) 46.0 (7.2) 50.1 (8.3) .36b MME = milligram morphine equivalent; NSAID = nonsteroidal anti-inflammatory drug; OTC = over the counter; PROMIS = Patient-Reported Outcomes Measurement Information System.
Notes: Low use defined as ≤75 MMEs; high use defined as >75 MMEs. Associations between high vs low self-reported opioid use and each predictor were evaluated with separate binomial regressions accounting for repeated measures.
↵a Interaction of predictor by time.
↵b Measures for which a modified Poisson regression approach for clustered data was implemented. Significant predictor-by-week interactions were followed with post hoc tests between groups at each week.
↵c Significant (P <.002) group differences.
↵d A T score of 50 is the average for the US general population, with a standard deviation of 10. Higher scores indicate greater intensity or interference.
Outcome Week 1 (N = 203) Week 2 (N = 202) Week 3 (N = 201) Week 4 (N = 201) Reason for not taking any opioid pain pills, No. (%) My pain was controlled without taking opioid pain pills 29 (14.3) 96 (47.5) 138 (68.7) 144 (71.6) Side effects were too strong 7 (3.4) 11 (5.4) 11 (5.5) 11 (5.5) I was concerned about becoming addicted 6 (3.0) 4 (2.0) 7 (3.5) 5 (2.5) I was concerned because I was breastfeeding 12 (5.9) 21 (10.4) 18 (9.0) 21 (10.4) I had no opioid pain pills left 2 (1.0) 16 (7.9) 27 (13.4) 27 (13.4) Other 1 (0.5) 4 (2.0) 8 (4.0) 4 (2.0) Storage location of leftover opioid pain pills, No. (%) Cupboard or wardrobe 43 (21.2) 46 (22.8) 45 (22.4) 45 (22.4) Medicine cabinet/other box 97 (47.8) 80 (39.6) 80 (39.8) 67 (33.3) Refrigerator 0 (0) 1 (0.5) 1 (0.5) 0 (0) Other 8 (3.9) 10 (5.0) 4 (2.0) 4 (2.0) Leftover pills were disposed of 11 (5.4) 6 (3.0) 8 (4.0) 6 (3.0) Don’t have any leftover pain pills 1 (0.5) 3 (1.5) 1 (0.5) 1 (0.5) Locked storage location, No. (%)a 32 (15.8) 31 (15.3) 26 (12.9) 23 (11.4) Opioid disposal location, No. (%) Household garbage 1 (0.5) 1 (0.5) 2 (1.0) 2 (1.0) Sink or toilet 5 (2.5) 2 (1.0) 5 (2.5) 3 (1.5) Returned to pharmacy 1 (0.5) 1 (0.5) 0 (0) 0 (0) Returned to other medication take-back program 2 (1.0) 2 (1.0) 1 (0.5) 0 (0) Other 2 (1.0) 0 (0) 0 (0) 1 (0.5) Note: subsamples used where appropriate.
a Among the subsample with any opioid pain pills leftover; denominator was 148 in week 1, 137 in week 2, 130 in week 3, 116 in week 4.
Sample and Predictor Adjusted RR (95% CI) Standard Error P Value All patients (N = 203) Opioid use in 24 h before discharge: per 7.5 MMEsa 1.09 (1.06-1.13) 0.02 <.001 Predischarge acetaminophen use 2.16 (0.93-5.02) 0.93 .07 Patients completing study (N = 201) Opioid use in 24 h before discharge: per 7.5 MMEsa 1.09 (1.06-1.13) 0.02 <.001 Predischarge acetaminophen use 2.16 (0.93-5.01) 0.93 .07 Patients reporting no preoperative opioid use (N = 198) Opioid use in 24 h before discharge: per 7.5 MMEsa 1.10 (1.06-1.14) 0.02 <.001 Predischarge acetaminophen use 2.07 (0.90-4.80) 0.89 .09 MME = milligram morphine equivalent; RR = risk ratio.
Note: Poisson regression models that estimate adjusted risk ratios for predicting high opioid use postdischarge (>75 MMEs, equivalent to 10 oxycodone 5-mg tablets, taken over 4 weeks).
↵a Equivalent to the MME of 1 oxycodone 5-mg tablet taken in the 24 hours before discharge.
The Article in Brief
Predicting Opioid Use Following Discharge After Cesarean Delivery
Karsten Bartels , and colleagues
Background Women who take less opioid pain medication in the 24-hour period before being discharged from the hospital after a cesarean delivery also use less opioid medication during the four weeks following discharge. Doctors prescribe opioids to most C-section patients, though the total milligram morphine equivalents they prescribe vary widely, which can unintentionally result in overprescribing pain medication. While persistent opioid use after C-section is rare, overprescribing creates a pool of uncontrolled opioids in the community, which poses a potential risk for non-medical use.
What This Study Found A team of researchers at the University of Colorado who conducted a prospective cohort study of 203 C-section patients found that those reporting low opioid intake after discharge took on average 44% less opioids in the 24-hours prior to discharge compared with those reporting higher usage. Researchers also learned that most of the patients in the study did not properly dispose of leftover opioids.
Implications
- Quantifying the amount of opioids taken during the last day of hospitalization may help better inform prescribing practices for the continuation of pain medication during recovery. The researchers recommend further study to evaluate the impact of implementing such measures on prescribing practices, pain, and functional outcomes.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.