
Abstract
PURPOSE Operational failures are system-level errors in the supply of information, equipment, and materials to health care personnel. We aimed to review and synthesize the research literature to determine how operational failures in primary care affect the work of primary care physicians.
METHODS We conducted a critical interpretive synthesis. We searched 7 databases for papers published in English from database inception until October 2017 for primary research of any design that addressed problems interfering with primary care physicians’ work. All potentially eligible titles/abstracts were screened by 1 reviewer; 30% were subject to second screening. We conducted an iterative critique, analysis, and synthesis of included studies.
RESULTS Our search retrieved 8,544 unique citations. Though no paper explicitly referred to “operational failures,” we identified 95 papers that conformed to our general definition. The included studies show a gap between what physicians perceived they should be doing and what they were doing, which was strongly linked to operational failures—including those relating to technology, information, and coordination—over which physicians often had limited control. Operational failures actively configured physicians’ work by requiring significant compensatory labor to deliver the goals of care. This labor was typically unaccounted for in scheduling or reward systems and had adverse consequences for physician and patient experience.
CONCLUSIONS Primary care physicians’ efforts to compensate for suboptimal work systems are often concealed, risking an incomplete picture of the work they do and problems they routinely face. Future research must identify which operational failures are highest impact and tractable to improvement.
INTRODUCTION
High-quality health care depends on well-functioning operational systems that ensure that what is required to meet patient needs is in the right place at the right time.1 Operational failures, defined as system-level errors in the supply of necessary materials, equipment, or information to employees,2 frequently frustrate health care professionals’ efforts to care for their patients. These failures (eg, no thermometer probe covers in stock; searching for missing devices; reordering incorrect medicines sent to ward, etc) have been well-studied in the hospital literature, revealing that cumulative time losses associated with even minor recurrent failures are significant.2–4 By degrading individual and organizational performance, operational failures complicate the delivery of high-quality care, with multiple adverse consequences for patient safety and experience, efficiency, and worker satisfaction.2,3
Since operational failures are potentially tractable to improvement, for example through work systems and process redesign,4 it is important that they are recognized and addressed. The challenges associated with operational failures have, however, received far more attention in the hospital research literature than in the primary care literature. This is problematic because failings that affect the ability to provide safe, high quality care are likely to be highly consequential in primary care, where the majority of health care contacts occur5,6 and where escalating workload, unprecedented levels of stress, and a crisis in recruitment and retention are major threats to sustainability.7,8
In this article, we report a review that sought to produce a synthesis of the existing research literature on operational failures in primary care, with the aim of optimizing learning from studies thus far. We sought to move beyond simply cataloging the failings described in the literature to characterizing how they affected primary care physicians’ work.
METHODS
We conducted a critical interpretive synthesis,9 a method that seeks to incorporate elements of conventional systematic reviews with an interpretive and critical approach to analysis, allowing synthesis of complex, diverse bodies of literature, and that is especially suited to theory generation. In this approach, processes of question formulation, searching, selection, data extraction, critique, and synthesis are characterized as iterative, interactive, dynamic, and recursive rather than as fixed procedures in a predefined sequence. Searching and selection of relevant articles was undertaken systematically, but the main focus of our analysis, consistent with the critical interpretive synthesis approach, was conceptual development rather than data summary.
Formulating the Review Question
We formulated our review question iteratively in response to initial search results and early findings. We began by using “operational failures” as a sensitizing concept,10 using the definition that had been developed in the context of hospital medicine: “system-level errors in the supply of necessary materials, equipment, or information to employees.”2 Our initial sweep of the literature identified that the term “operational failures” was absent from the primary care literature. However, many studies reported problems that conformed to the general definition. After team discussion, we devised the exploratory review question: “What problems can be identified in the literature as representing operational failures in primary care and how do these problems affect primary care physicians’ work?” Further, given the system-level characteristics of operational failures, we specified “system” holistically to include anyone or anything a primary care physician must interact with in order to perform their work.6
Searching the Literature
We developed our search strategy in collaboration with a medical librarian (search protocol in Supple-mental Appendix 1, http://www.AnnFamMed.org/content/18/2/159/suppl/DC1). We searched 7 databases (Table A1, Supplemental Appendix 1), as well as gray literature to find citations that addressed organizational problems, supply errors, disruptions, and interruptions in primary care from database inception until October 17, 2017. The search was conducted by author J.P. We did not restrict our search by study design or method.
Developing the Inclusion and Exclusion Criteria
We developed our inclusion and exclusion criteria (Table 1) to capture empirical studies of problems that represented operational failures in primary care. The principal inclusion criterion, that a study described how a problem affected primary care physicians’ work, helped to distinguish the literature of interest from adjacent literatures on adverse events, medical errors, quality and safety, task distribution, and workflow that were not strictly relevant to our goals.
Inclusion and Exclusion Criteria
Sampling
Once all results had been saved, each citation was screened, facilitated by Endnote software. One author (J.P.) reviewed titles and/or abstracts for all citations retrieved. Two authors (C.S., A.G.) undertook second screening of 15% of the total set of citations each, meaning that 30% of the entire set received a second screening. The results from each reviewer were discussed and compared in a daylong team meeting. We did not undertake a formal test of interrater agreement, but all of the articles deemed potentially relevant by C.S. and A.G. (n = 130) had also been deemed potentially relevant by J.P. in his screen of the whole data set, suggesting high reliability. A highly inclusive approach to full-text retrieval was used to ensure that any potentially eligible article was considered. Two reviewers (C.S., A.G.) assessed all full texts independently and resolved discrepancies in inclusion decisions by consensus.
Determination of Quality
We assessed all studies using the 5 quality criteria (Table A2, Supplemental Appendix 1) described in the original account of critical interpretive synthesis9 and, consistent with the approach, only excluded papers with major methodological limitations that were deemed “fatally flawed.” This resulted in exclusion of 2 papers that would otherwise have been included on the basis of relevance (journalistic-style papers).
Data Extraction
We extracted prespecified information on study setting, design, sample, and key findings (qualitative and numerical) on what and how failings in primary care work systems affect primary care physicians’ work using a template (Table A3, Supplemental Appendix 1). We used shared tables in GoogleDocs for data extraction. Key findings were imported into NVivo 11 to facilitate data analysis.11
Analysis and Synthesis
We began by inspecting papers’ key findings, identifying recurring issues and generating themes across papers. As part of this process, we updated and refined the categories of operational failures in hospital nursing proposed by Tucker et al2,3 (Table 2) to better account for issues evident in our data.
Using authorial skills,12 we undertook a critique of the entire corpus of data and characterized the impacts of operational failures on primary care physicians’ work. This analysis was aimed at the development of a synthesizing argument9: a critically informed integration of evidence from across included studies. This analysis involved the generation of synthetic constructs (new constructs generated through synthesis) that, where appropriate, drew on relevant literatures from social science and engineering—for example, relating to emotional labor, which describes how management and regulation of emotions may be a work requirement for many occupational groups,13 and resilience engineering, which describes the difference between work-as-done vs work-as-imagined.14 As a team, we met to engage reflexively with findings at each stage and to discuss how material would be handled. We secured dependability by seeking evidence of repetition or saturation of themes and thorough iterative analysis.
RESULTS
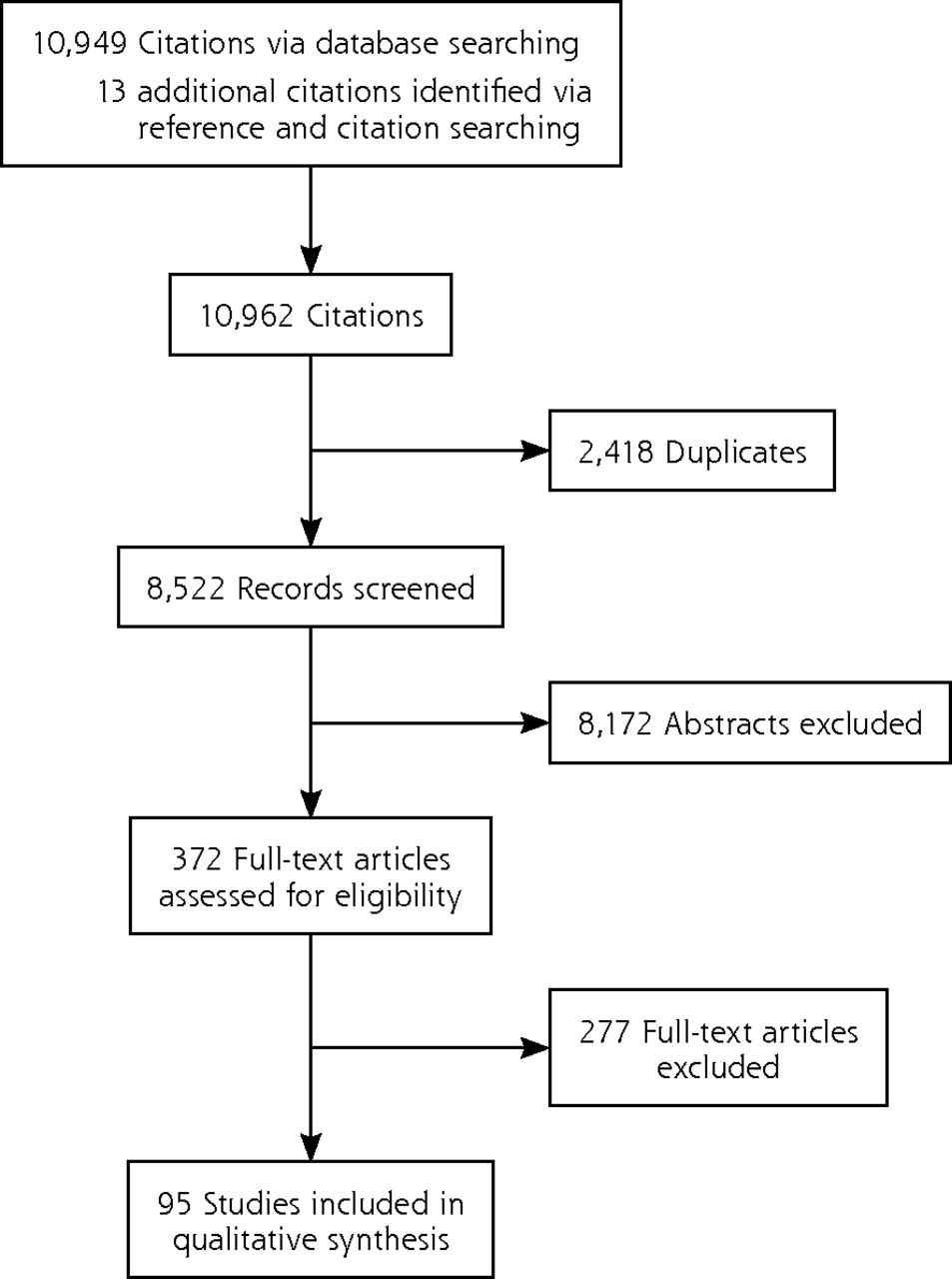
Our bibliographic searches identified 8,544 unique citations. We retrieved 372 full-text articles, of which 95 studies satisfied our inclusion and exclusion criteria (Figure 1).

Flow diagram of search.
Critical Summary of the Literature
As noted in the Methods section, a perhaps remarkable feature of the literature on primary care physicians’ work is the limited explicit attention given to operational failures. Further, even when studies address what might on the face of it appear to be operational failures, they often do not examine the impacts of those failures on physicians. Thus, we excluded over 200 studies because they did not examine the effects of suboptimal work systems on primary care physicians. For example, 48 papers identified discrepancies in patients’ medication lists at transitions of care as a frequent problem, but 44 did not refer to the impact on or work required of primary care physicians to resolve the discrepancies and were thus excluded. Even among included studies, few quantified the specific impacts of operational failures, instead tending to focus on generalized metrics such as physician satisfaction.
An overview of the 95 included studies is provided in Table A4, Supplemental Appendix 1. In summary: 39 were qualitative, 38 quantitative, 15 mixed-method, and 3 were reviews. Most studies came from the United States (65), followed by the United Kingdom (12), Canada (5), Ireland (3), Israel (2), and 1 each from Australia, Cyprus, Malaysia, New Zealand, Norway, Singapore, Spain, and the United Arab Emirates.
The most frequently reported operational failures related to information technology, with accounts of problems with electronic health records (n = 19 studies), computer decision support systems (18), e-prescribing (9) and e-referral systems (3). Failures in practice processes were the next most frequent focus, and mostly related to inefficient channeling of information through the practice (30) or inefficient material supplies (3). Fewer studies dealt with operational failures arising from secondary care, such as suboptimal communication of patient information (7), medication discrepancies (4), and flawed systems for patient testing (2). The impacts of the operational failures (Table 3) included consuming time, disrupting task completion, delaying clinical decisions, and interfering with the doctor-patient relationship.
Impact of Operational Failures on Primary Care Physicians’ Work and Examples Associated With These Impacts
Synthesizing Argument: Operational Failures Configure Primary Care Physicians’ Work and Require Compensatory Labor
Our synthesizing argument is that operational failures contribute to how primary care physicians’ work is configured; much of the effort to address work-as-configured can be characterized as compensatory labor, involving multiple mundane and frustrating tasks that often remain invisible and undervalued, but are essential to delivering on the obligations of physicians’ professional role. This argument mobilizes 2 synthetic constructs: work-as-configured and compensatory labor, which we elaborate on below.
The literature suggests that operational failures are pervasive in primary care physicians’ daily work. The failures described were characteristic of what Hollnagel describes as the gap between “work-as-imagined” (work as it ought to be) and “work-as-done.”14 An important feature of the literature we examined was how the gap between what physicians perceived they should be doing and what they were doing was to a large extent actively organized by operational failures over which they themselves often had very limited control. We generated the synthetic construct of “work-as-configured” to describe how operational failures structured work-as-done.
Further reflecting Hollnagel’s suggestion that complex systems like health care only succeed because of resilience of responses to imperfect work conditions,15 we found that work-as-configured compelled physicians to take action to compensate for the suboptimal systems in which they worked.15 Pivoting from the notion of “emotional labor,”13 which was developed to describe how the management and regulation of emotions may be a work requirement for many occupational groups, we generated the synthetic construct of “compensatory labor” to describe the demand for primary care physicians to undertake additional work in response to work-as-configured. Compensatory labor was essential for primary care physicians to fulfill their duties of overseeing, coordinating, and safeguarding patients’ care, yet was not usually clinical in character. Instead, it tended to involve characteristically mundane tasks (eg, chasing information from hospitals, resolving technology malfunctions; Table 3). Physicians perceived much compensatory labor as distracting and detracting from their proper work with patients.
The mundane nature of compensatory labor surfaced repeatedly, for example, in studies of technology-related tasks. Poorly designed technologies configured work via slow running speeds, time-consuming searches for information within electronic records, or requirements for duplicated data entry16–41 perhaps as a consequence of technologies being designed around the needs of administrators, regulators, and insurance providers rather than physicians.16–18,20,42,43 Similarly, the daily work of repeat prescribing was frequently interrupted by problems including incorrect information in electronic formularies, out-of-date medication histories, and prescriptions “going missing” on their journey between practice and pharmacy, leaving physicians to undertake additional work to fulfil their duties to the patient.17,35–38,40,44–51
Primary Care Physicians’ Nodal Position and Work- as-Configured
Primary care physicians occupied a nodal position among multiple interacting but fragmented components of the health system (the patient, secondary care, community care, pharmacy etc). This nodal position required them to integrate scattered information to produce plans for patient care,52–58 and led to the frequently reported operational failure of “information discontinuity.” For example, discharge and outpatient letters from secondary to primary care physicians were delayed, ambiguous, or absent in up to 77% of patients,52,53,56,59–62 and letters that did arrive often lacked detail about in-patient treatment (7% to 22%), test results (65%), patient counseling (90% to 92%), or follow-up plans (2% to 43%).47,52,53,60 Information discontinuity hindered physicians’ ability to implement clinical decisions,52,56,59,60,63 to which they generally responded by taking multiple compensatory steps to find the missing information.53
“Information overload” arose from physicians’ responsibility to review all patient-related information. US physicians received approximately 60 notifications from other care clinicians daily,64–67 and though many were for trivial nonclinical issues, physicians reported anxiety about missing critical information among the many notifications received.64 “Information scatter” described health records cluttered with entries from other health care clinicians.21,44,66,68 Difficulties
finding “buried” information”21,23,34 led many physicians to simply ask patients for required information instead23,32,36,44,68, while others kept memos for themselves on complex cases, or developed tracking systems for important outgoing correspondence, prescriptions, and test requests.16,19,20,22,25,27,29,30,32,36,44,47,57,63,65,67–69
Amplification of Compensatory Labor by Suboptimal Task Distribution and Delegation Within Practices
Although up to 80% of primary care physicians’ tasks were potentially “do-able” by other practice staff, physicians tended to retain ownership of response to operational failures.16,47,67,70–72 Work-as-configured was an important explanation for this low level of delegation. External agents determined that certain administrative tasks (eg, obtaining insurance authorization, contacting laboratories for test results) must be completed by physicians.25,48 Within practices, delegated tasks could “loop” between clinical and clerical staff, often creating more work for the physician and delaying task completion.70 Intended improvements in practice processes sometimes inadvertently lead to more work for physicians.16,20,73–76 For instance, the adoption of electronic health records meant that tasks previously done by clerical staff were now being left to physicians: “Earlier I dictated referrals. Now I type them myself.”16,18–20,27,28,32,43,48,68,70
Compensatory Labor is Invisible and Unrewarded
A unifying feature of many operational failures was that they were unaccounted for in primary care work systems, which were typically based on work-as-imagined and did not encode the requirement for compensatory labor. Hidden from view, little valued, and unrewarded, compensatory labor shared similarities with Allen’s construct of “organizing work,” which describes the everyday work nurses do to coordinate and organize patient care, much of which goes unnoticed and uncounted.1 Primary care physicians regularly fell behind schedule due to unpredictable operational failures that occurred within consultations,24,47,67,72,77–79 including repetitive, clinically-irrelevant electronic alerts that distracted physicians from patients’ primary clinical issues,19,21,22,42 pushed them into dealing with other tasks,24,33,37,38,53,78,80–84 and crowded their ability to think.24,26,38,42,46,66,80,82–91 Nine studies portrayed interrupted consultations (manifesting as phone calls or questions from other staff) as operational failures,92–100 that could affect from 5% to 90% of consultations.
As a consequence of the obscuring of compensatory labor and insufficient time to complete tasks elsewhere during the working day, consultations often ran longer than allocated. However, practices did not change physicians’ schedules to allow for these pressures, resulting in a problem labeled by Chesluk et al as the “fictive schedule.”72 The fictive schedule pushed compensatory labor into the interstices or out-of-hours, which further contributed to stress, low job satisfaction and burnout.16,47,48,67,68,70,72,77,101–104
DISCUSSION
Our interpretive overview of 95 studies has identified multiple problems in operational systems in primary care. These operational failures, combined with the role of primary care in synthesizing information and coordinating care, actively configure the work that physicians have to do to care for their patients, requiring significant compensatory labor to deliver on the goals of care. Often invisible and unaccounted for in scheduling or reward systems, compensatory labor typically involves mundane tasks that crowd clinical work and lead to unwanted consequences such as physician-stress and burnout.70,105 We further identified that even the research literature itself obscures work-as-configured, often identifying problems but not their impact on the work of physicians. Limitations in the evidence therefore risks presenting an incomplete picture of the work done by primary care physicians and the problems they routinely face, and of diminishing opportunities to improve the primary care work environment. Based on our findings, we concur with others that adding more physicians into broken systems is unlikely to solve the primary care crisis on its own: what is also needed is significant investment in improving the primary care work environment.48,106
Recommendations for Practice, Policy, and Future Research
These findings have important implications for practice and policy, suggesting that renewed attention to basic operational systems in primary care, including how these systems interact with others in the health and social care ecosystem, is much needed. Unless these challenges are addressed, bold efforts at practice redesign (eg, the Chronic Care Model, the patient-centered medical home, and more recently, in the United Kingdom, the NHS General Practice Development Programme) may flounder.32,107
Our findings also raise important questions for research. Hollnagel has suggested that studying the everyday performance adjustments made in the context of work conditions can highlight some of the challenges associated with complex systems like health care.15 Yet we found no papers that looked holistically at all aspects of primary care physicians’ work environment, limiting the ability to identify most critical operational failures, the overlaps or knock-on effects.20,21,23 Without closer examination of how the overall health system supports primary care and the “basic science” of what happens in primary care practice, efforts to improve operational systems themselves risk limited success.32
Strengths and Limitations
A Critical Interpretive Synthesis approach offered what a traditional systematic review could not: the ability to reframe and reinterpret existing literature through a synthesizing argument that could generate new insights and highlight research gaps9 Our multidisciplinary team supported reflexivity throughout the review process and guarded against framing of the analysis according to a single perspective, as did allowing the research question to be defined emergently rather than a priori. We further enhanced trustworthiness by searching multiple databases and using inclusive search terms, and achieved confirmability through team reflexivity and documentation of decisions.
Given the range and number of topics covered by our review, it is possible that we may have missed relevant studies. However, as our goal was conceptual saturation rather than finding every conceivable paper on a topic, we feel this pragmatic trade-off was acceptable. A further limitation of our study inheres in the literature itself and the research questions it has chosen to address: for instance, the dominance of technology papers is likely an artifact of the 2009 US legislation that incentivized physicians to use electronic records to achieve improvements in care, and may not reflect the true prevalence, nature, or range of impacts of operational failures in primary care.
Conclusions
Our synthesis of the literature demonstrates that operational problems in primary care configure the work of primary care physicians, requiring them to engage in compensatory labor to safeguard patient care. Future research must look more closely at the primary care work environment to determine which operational failures have the highest impact and which to prioritize for improvement. Practice and policy should recognize the significance and impacts of system-level operational failures on the work of physicians and the experiences and outcomes of patients.
Acknowledgments
We gratefully acknowledge the expertise and assistance of Ms Veronica Phillips, Medical Librarian at the School for Clinical Medicine, University of Cambridge, UK.
Footnotes
Conflict of interest: authors report none.
To read or post commentaries in response to this article, see it online at http://www.AnnFamMed.org/content/18/2/159.
Funding support: This work has been supported by an NIHR (UK) Clinical Lectureship (C.S.), an Academy for Medical Sciences (UK) Starter Grant (SGL018\1023) (C.S), and a Wellcome Trust Senior Investigator Award (WT09789) (M.D.-W.). M.D.-W. is supported by the Health Foundation’s grant to the University of Cambridge for The Healthcare Improvement Studies Institute. The Health Foundation is an independent charity committed to bringing about better health and healthcare for people in the United Kingdom. M.D.-W. is a senior investigator in the National Institute for Health Research (NF-SI-0617-10026). The views expressed in this article are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, the Department of Health and Social Care, the Health Foundation, the Academy for Medical Sciences or the Wellcome Trust.
Previous presentation: This review was presented at the Society for Academic Primary Care Annual Scientific Meeting; July 10-12, 2018; London, England.
Supplemental materials: Available at http://www.AnnFamMed.org/content/18/2/159/suppl/DC1/.
- Received for publication January 8, 2019.
- Revision received July 11, 2019.
- Accepted for publication July 22, 2019.
- © 2020 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Understanding access to general practice through the lens of candidacy: a critical review of the literature
- Operational failures in general practice: a consensus-building study on the priorities for improvement
- Applying an equity lens to hospital safety monitoring: a critical interpretive synthesis protocol
- Using an electronic safety netting tool designed to improve safety with respect to cancer referral in primary care: a qualitative service evaluation using rapid appraisal methods
- Identifying how GPs spend their time and the obstacles they face: a mixed-methods study
- Operational failures and how they influence the work of GPs: a qualitative study in primary care
- Impacts of Operational Failures on Primary Care Physicians Work: A Critical Interpretive Synthesis of the Literature