
Article Figures & Data
Figures
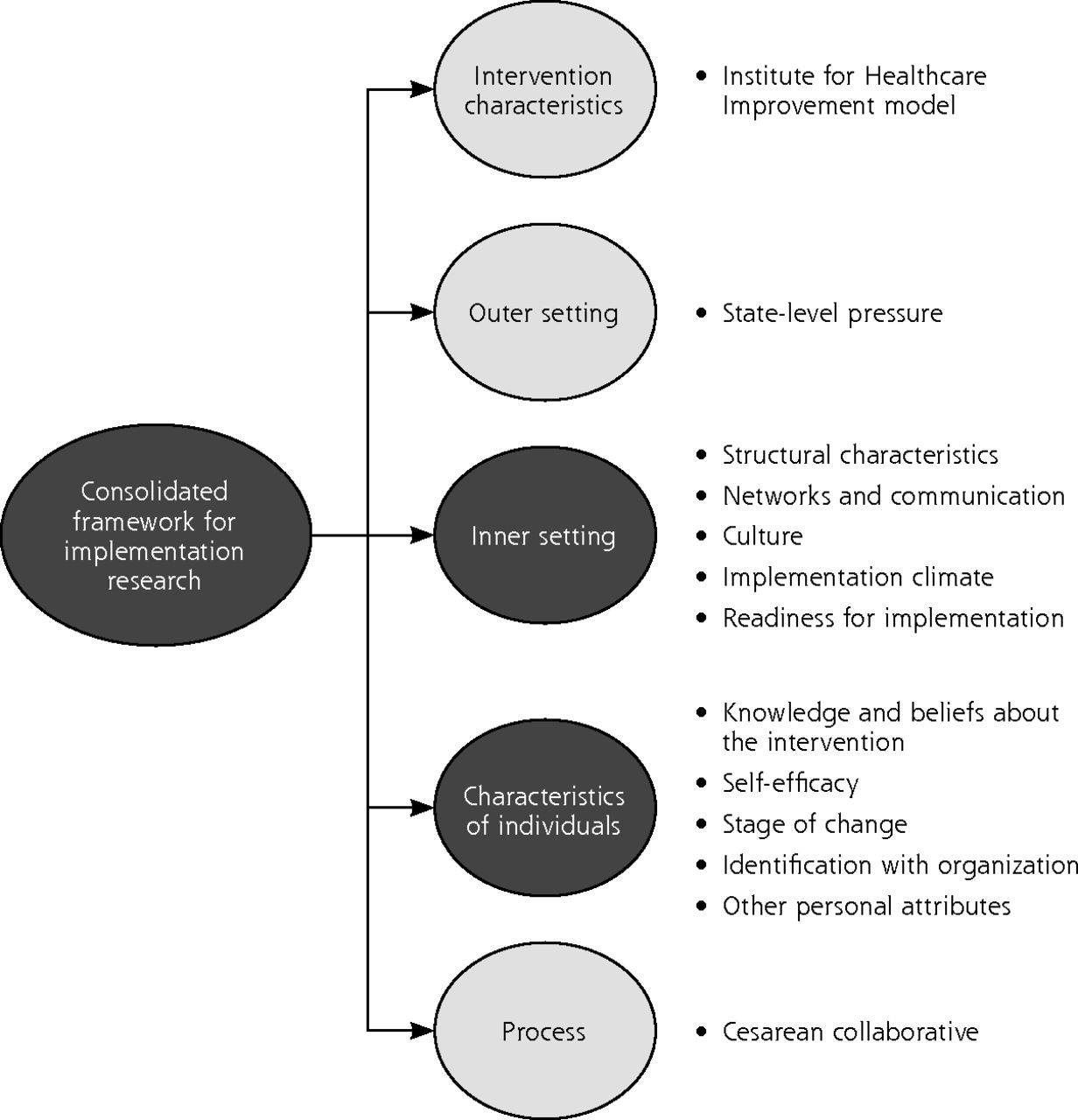
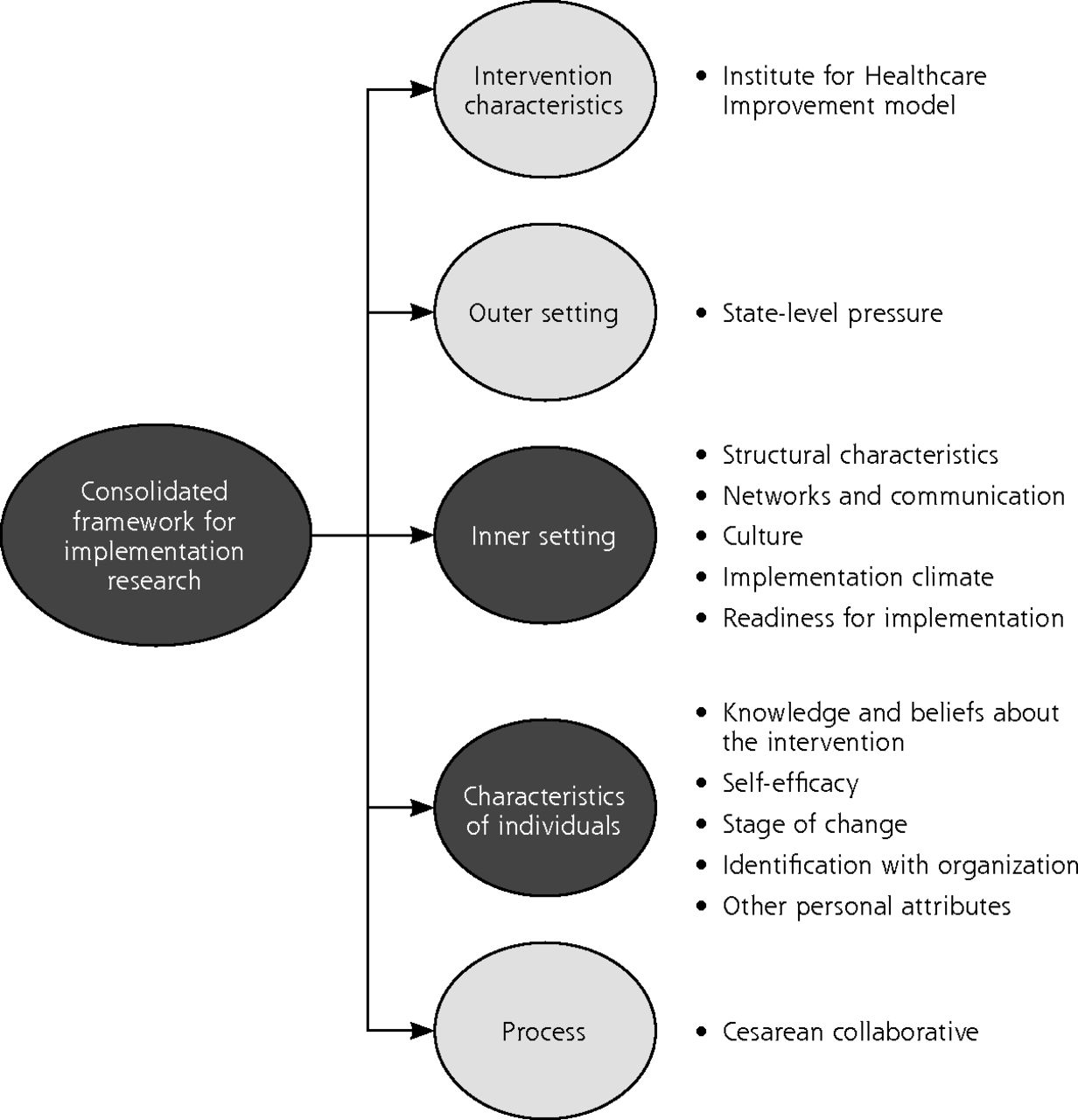
- Figure 1.
The consolidated framework for implementation research.16
Notes: This framework is annotated with the Supporting Vaginal Birth initiative’s existing and needed domains. Black circles denote domains with poorly characterized barriers and facilitators of success. Gray circles denote domains with existing facilitating infrastructure.
Tables
Best Practice, % in agreement Registered Nurses Medical Doctors Nonresponder Hospitals (n = 281) Successful Hospitals (n = 378) P Value Nonresponder Hospitals (n = 41) Successful Hospitals (n = 130) P Value Providing more midwifery service 61.4 66.1 .23 24.4 45.4 .017a Implementing a program that supports early labor at home 87.2 89.3 .44 57.5 76.2 .022a Providing more direct (in room) nursing time with laboring women 75.2 81.9 .045a 68.3 81.4 .077 Providing more doula services 40.2 47.9 .06 17.1 43.9 .002a Reducing the number of inductions of labor for nonmedical indications 96.4 94.6 .30 63.4 85.4 .002a ↵a Statistically significant result.
- Table 2.
CFIR Inner Setting Constructs, Contextualized Definitions, and Illustrative Quotes
Construct Contextualized Definition Example Quotes From Focus Groups Facilitators of Change Barriers to Change Structural characteristics Existing clinicians - generational differences in communication and teamwork styles “In general, everyone does have the desire to get along and some of the older generation doctors still live in the world of they’re the boss and ‘don’t tell me what to do.’ But the majority of the physicians...do appreciate the collaboration and have that understanding that there’s multiple checkpoints along a patient’s care path, and that anyone can catch those.”
“A lot of these new physicians coming in listen to the nurses now. They have a better relationship. They know that the nurses are the ones at the bedside… it’s not so much, ‘I’m the doctor. You’re going to do everything that I’m telling you to do.’ There is a different culture with physicians coming out of med school now.”“Some of the older doctors that were kind of set in their ways, we still have two of them that just will not change no matter what we do. We’re just waiting for them to retire…because it’s hard to change a culture when you have somebody who’s been doing something for like 25 years and refuses to change, if they have a large portion of the deliveries.” Size of the organization or hospital unit and how this impacts perceived organizational characteristics and impacts outcomes “With the doctors too...we know each other very well, especially because we have such a small number of physicians working here.” “We have certain doctors … their episiotomy rate is so high that it drags [the quality metrics down] – it’s a small hospital.… They’ll do maybe 20, 30 deliveries a month, but they do episiotomies on half of them so that bumps your epis rate. So individual practices like that, especially in a small hospital that doesn’t [have a large] deliver(y) [volume], has a huge impact on your numbers.” The current provider mix of L&D providers “we’re in a pretty good place… [because we have been] adding in midwives as the first call for low risk patients. And so the nurses…find that so helpful that they’ve got a midwife to work alongside.” Quantitative/LCS Insight: Increasing the presence of midwives on L&D was seen as a good way to reduce cesarean by only 24% of physicians at non-responder hospitals versus 45% at successful hospitals. The existence or lack of formalized communication processes and hierarchies; and the functional role of informal communication processes “I would say when we were really doing [Formal Team Training Program], one of the things was after every single delivery, good, bad or otherwise, we did a debrief. And one of the things I liked about that was we didn’t wait for bad outcomes to do debriefs.”
“…It’s often centered around some discrepancy in management, where I want the nurse to do something and she says, ‘I can’t. That’s not protocol or that’s not policy,’… instead of...discarding that…[we] dive into why nurses continue to follow certain policies...It’s just a larger discussion.”“It can be awkward. Oftentimes, if a nurse is having trouble with a provider or with another nursing staff member, they’ll talk to the charge nurse...The first thing I’ll say is, well have you talked to the person? So sometimes it gets difficult because people don’t want to hold each other accountable...or they feel it’s not their job to do it.…You can’t always just escalate every problem to [Nurse Manager].” Culture Norms and values of unit, subcultures of nurses and physicians and professional siloes; Cultural flexibility “Well I would say we’re a huge team, and we treat each other like family, and that includes the physicians too that work with us. As far as patients, I feel like we try to provide holistic patient care, including patients, their family members, friends.”
“When we’re making the assignment, we take different things into consideration...if there’s someone who has a natural approach… well so and so’s going to be great for this patient because that’s… how she likes to practice… the nurse then feels rewarded because they’re having the type of experience…that is in alignment with their beliefs as well.”“One of the things we’ve been able to overcome, the nurses’ story “we’re the patient advocate,” somehow pinning the physician as not the patient advocate. I don’t hear that as much anymore. It’s been better recognized that all of us are patient advocates, but the nurses are still on a 12-hour shift and they’re going to check out in 12 hours and many of us [physicians] will still continue on for days with a patient, if that’s how long it takes.” Implementation climate Fear and resistance to change “Just making it more obvious that there are more people reaching out and trying to address this problem and it’s not going to go away. To me, the bottom line is the physicians. The physicians are the ones who make the call to do the C-section, nobody else. So it’s bottom line, you’ve got to get the physicians more on board with everything.” “Liability is a major player when it comes to physicians and NTSV rates. I think the physicians are scared to take risks and not go to C-section because they’re worried about the liability.”
“I think… fear of a bad outcome, fear of sitting on a strip too long and fear of getting sued. But even more so is fear of having to tell the mom, ‘Your baby has a lot of problems because, you know, we waited too long [to call for a cesarean]’.”Organizational incentives & rewards “Evidence based process and allow you to do audits and all staff [were] audited. Amazing opinions on how do things better. Did all units and started working. Put up reward boards, celebration,..., personal notes and acknowledgement in huddles. Now they are working on communication. Next collaboration and teamwork. Staffing last per their assessment.” “And those individuals that lack some motivation or lack the understanding of, the importance of some of this stuff and working with them individually... If I were to talk about something right now to help improve, it would be recognizing people for doing a great job and getting that out there.” Goals & feedback “A lot of it is during our meetings. We have separate meetings regarding the C-section rate, and sometimes we may outline certain problem physicians or certain physicians who are a little bit more quick in making decisions. So some of those physicians have to be spoken to individually and to encourage them to do what they can to be a little bit more conservative.” Learning climate Team members feel safe, input is/isn’t valued “The nurses are very strong and they’re solid in their skills, their knowledge in Labor & Delivery. And so I think that gives them more confidence with the physicians and with the providers. And at the same time, the providers then trust them when they are asking them for something or if they’re needing support on something, the doctors are receiving that pretty well because of the trust that they have with their knowledge.” “Some of our charge nurses can be a little bit hard on newer people...When someone’s more of a slow learner or a slower learning curve, there’s sometimes not much patience for that. I think we could do better.” Leadership engagement Leadership commitment, involvement, and accountability “Well, I just think that working together for so many years, building that trust. I know we have a … our chief medical officer is not an obstetrician, but he’s doing everything he can to learn about obstetrics. So he really drives that from the doctor’s side of it. He is really instilling in the doctors the importance of collaborating as a team. Not that they needed it too much, but he just really reinforces it.” “With [Nurse Manager] being the director when she’s telling people to please do something, it really is more likely to be done than if I was to ask them to do something...[Nurse Manager] is stretched very thin. She has a lot of responsibilities around the hospital and I think maybe it wasn’t totally on her radar so much either, even though we had talked about it. But then when it came down to it, it wasn’t. And with [Physician] being our physician champion, it wasn’t on her radar so much either, even though we had talked about it.” Readiness for implementation Level of resources dedicated to implementation and operations; Ease of access to shared resources “We did a lot of joint education, which was great. We did some fetal monitoring education with the providers and the nurses. We’ve been doing simulations. That’s been great with pulling the providers in. We conducted a retreat, a unit retreat about a year ago.” “The physicians themselves too, we don’t have a laborist program, so the doctors aren’t necessarily...here in-house. So knowing that these other providers have 30-minute response times, sometimes the doctors will decide to do a C-section a little bit sooner than maybe they would in another department when they know that they have everyone readily available...like a Category 2 strip they might wait a little bit longer at another facility because they have resources readily available, but because we don’t have those resources always readily available sometimes the doctors will make the decision to do a C-section a little bit earlier than they may have at a different facility.” C-section = cesarean section; CFIR = Consolidated Framework for Implementation Research; L&D = labor and delivery; LCS = Labor Culture Survey; NTCV = nulliparous, term, singleton, vertex.
- Table 3.
Illustrative Quotes for Theme of Interprofessional Communication by Hospital Success
Successful Hospital Nonresponder Hospital “We communicate right when it’s happening. [We want to show] one team effort. [Patients] want to see us as a united front.” (Physician) “You have to be pretty diplomatic. You can’t... tell them what to do. Make some soft suggestions and maybe try to encourage them to [use best practices].” (Physician) “If a nurse is having trouble with a provider or with another nursing staff member, they’ll talk to the charge nurse. The first thing I’ll say is, ‘Well have you talked to the person?’” (Charge Nurse) “I do have a few nurses that are meek or don’t feel comfortable standing up to doctors or don’t feel comfortable contradicting what the doctor wants them to do.” (Nurse)
Supplemental tables
Supplemental tables 1-3
- Supplemental data -
PDF file
- Supplemental data -
The Article in Brief
Culture That Facilitates Change: A Mixed Methods Study of Hospitals Engaged in Reducing Cesarean Deliveries
Emily C. White VanGompel, and colleagues
Background Most patients with depression are treated in primary care, and the majority of those patients prefer psychotherapy over treatment that includes medication (i.e., pharmacotherapy). Primary care physicians, however, don’t usually provide psychotherapy and are inclined to prescribe antidepressants to patients with depression in their care.
Although studies have shown the effectiveness of psychotherapy in primary care patients, researchers haven’t extensively examined the outcomes in which psychotherapy for primary care patients is compared with pharmacotherapy, combined treatment, and other clinical scenarios.What This Study Found Researchers at the Vrije University Amsterdam examined the effects of the two major approaches to treating depression: psychotherapy and pharmacotherapy, as well as combined treatment and care-as-usual. The study integrated the results of 58 randomized controlled trials with a total of 9,301 patients. Results concluded that both psychotherapy and pharmacotherapy were significantly more effective than care-as-usual or waitlist control. However, they found no significant difference between psychotherapy and pharmacotherapy as stand-alone treatments. Combined treatment, particularly in studies that included cognitive behavioral therapy, was better than either pharmacotherapy or psychotherapy alone.
Implications
- Treatment in primary care should be organized to accommodate any of these treatments in response to patients’ preferences and values.




{kind=link}