
Article Figures & Data
Figures
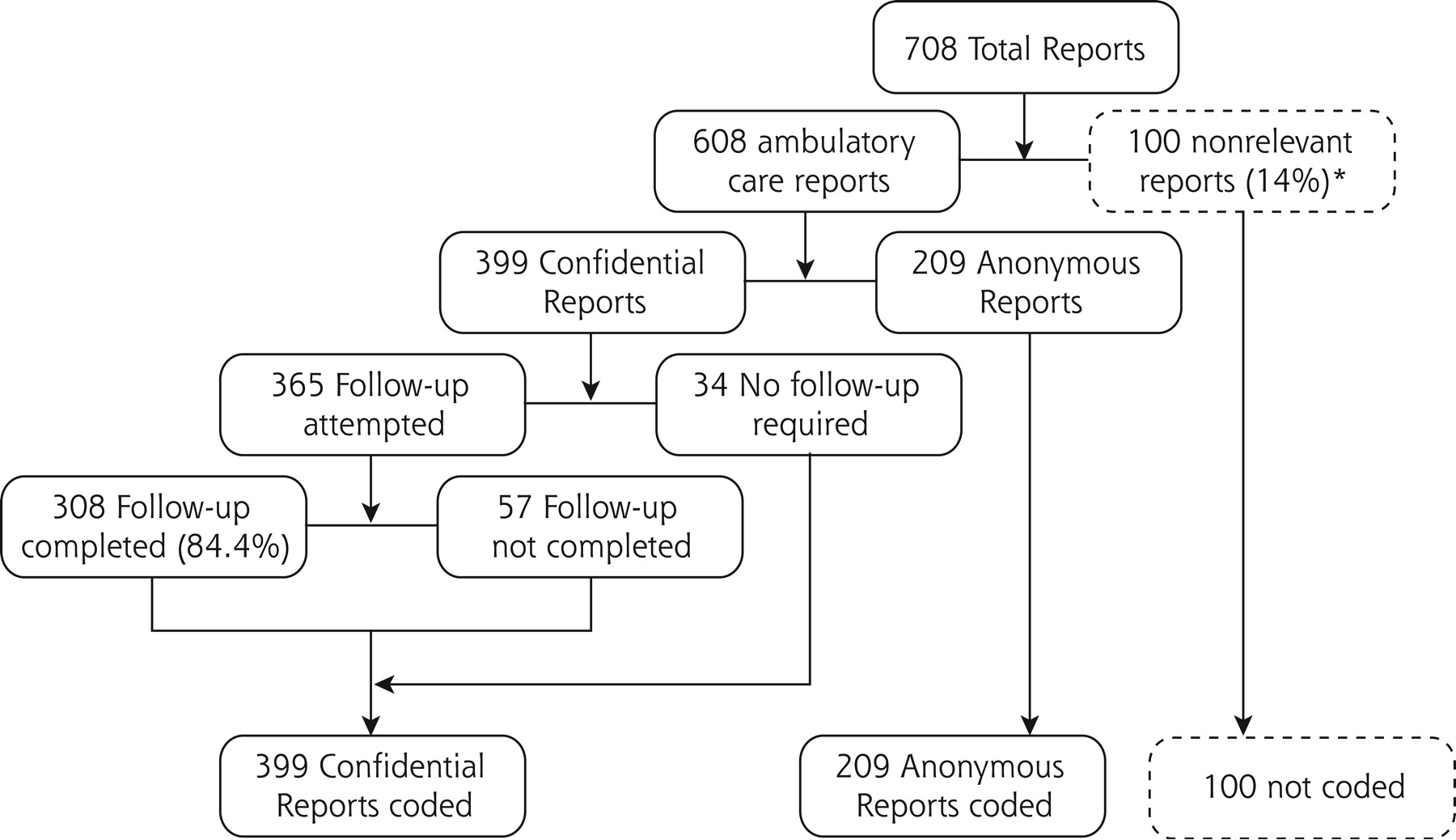
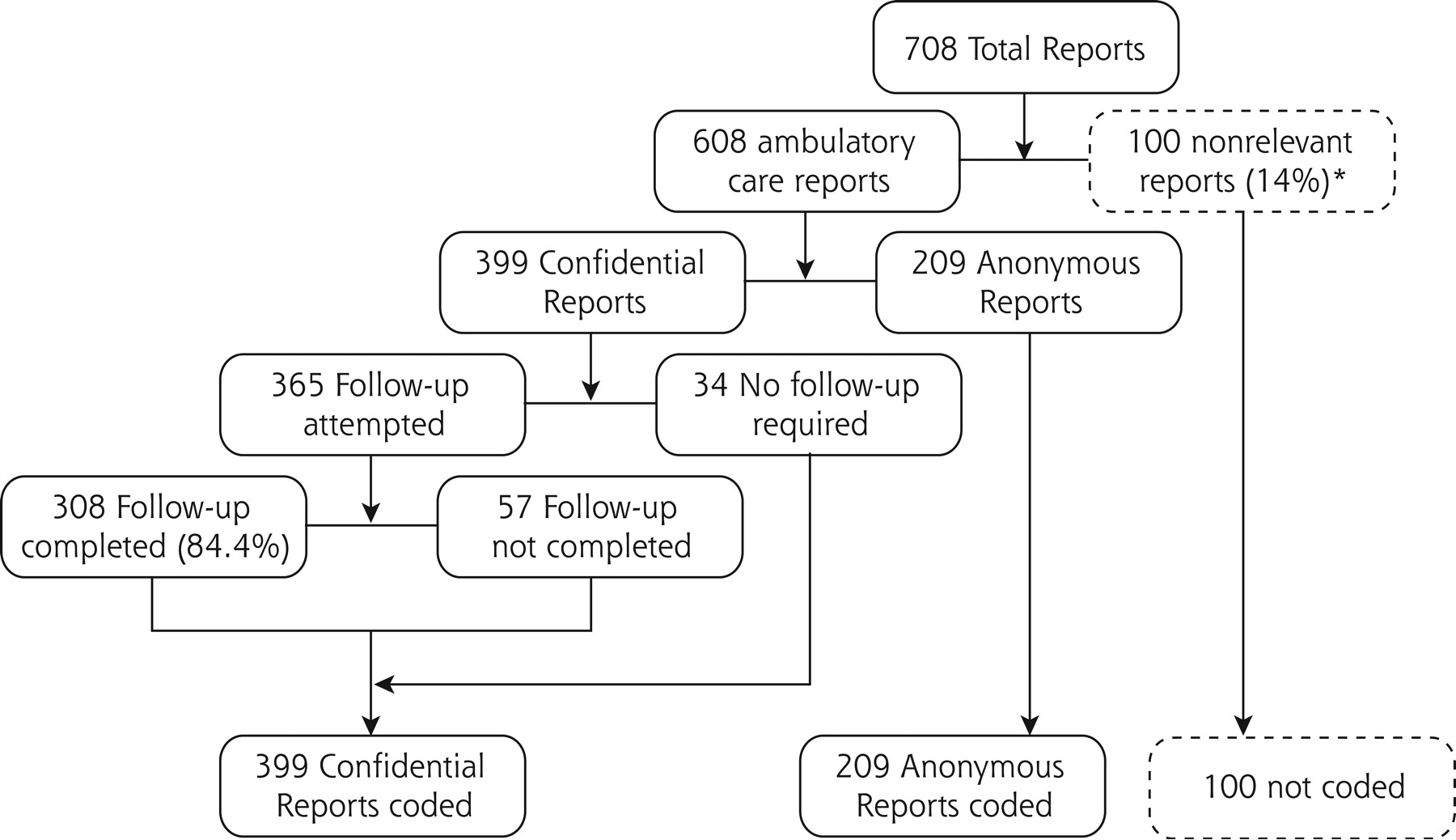
- Figure 1.
Inclusion and outcome flow diagram for reports to Applied Strategies for Improving Patient Safety (ASIPS). * Not relevant to ASIPS analysis or not an ambulatory event (eg, occurred entirely in inpatient setting; no unexpected outcome; not related to patient care or safety).
Tables
Questions Answer Format Anonymous report form Indicate the role you were performing when you discovered the event Check box; 6 choices Type of practice Check box; 4 choices Describe the event you wish to report Free text In your opinion, could this event have been prevented? Yes or no, plus free text In your opinion, was (were) the patient(s) harmed as a result of this event? Yes or no, plus free text In your opinion, does (do) the patient(s) know about this event? Yes or no, plus free text Approximately how often do you think events like the one you are reporting occur in your practice? Check box; 3 choices Does this event involve just 1 patient? If YES… Yes or no Enter the patient’s age Number What is the patient’s sex? Male/Female Does the patient consider himself or herself to be Hispanic or Latino? Yes or no Please check the racial group(s) you believe the patient would want to be associated with Check box(es); 6 choices Confidential report form Your name Free text Telephone number where you can be reached Telephone number Indicate the best time to call Check box; 2 choices Briefly describe the event you wish to report Free text Type of Error Total No. Anonymous Reports No. (%) Completed Confidential Reports No. (%) All Confidential Reports (Intention to Treat) No. (%) * P <.10. † P <.05 Diagnostic testing errors (all laboratory tests imaging, cytology, pathology, and stress tests) 325 101 (48.33) 194 (56.73)* 224 (56.14)* Blood test 129 36 (17.22) 84 (24.56)† 93 (23.31)* Other specimen 67 24 (11.48) 40 (11.70) 43 (10.78) Imaging 58 18 (8.61) 33 (9.65) 40 (10.03) Other or unspecified test 31 6 (2.87) 18 (5.26) 25 (6.27)* Medication errors 165 65 (31.10) 89 (26.02) 100 (25.06) Wrong drug 32 13 (6.22) 14 (4.09) 19 (4.76) Right drug: wrong dose or timing 99 39 (18.66) 53 (15.50) 60 (15.04) Right drug: wrong administration or dispensing 39 13 (6.22) 26 (7.60) 26 (6.52) Drug not prescribed 6 1 (0.48) 5 (1.46) 5 (1.25) Communication errors 437 148 (70.81) 250 (73.10) 289 (72.43) Reporter Group Reports No. (%) Confidential Reports* % * P <.001; based on 522 (of 608) reports for which there were reporter data. MD = doctor of medicine; DO = doctor of osteopathy; PA = physician’s assistant; NP = nurse praditioner; RN = registered nurse; LPN = licensed practical nurse; MA = medical assistant; lab tech = laboratory technician. Clinicians (MD, DO, PA, NP) 358 (68.58) 55.03 Nursing staff (RN, LPN, MA, lab tech) 128 (24.52) 84.38 Nonclinical staff (front office, medical records, administrative and billing staff) 36 (6.90) 80.56 Completed Confidential Reports All Confidential Reports Insufficient Information to Code (Unknown) Anonymous Reports % % PValue % PValue NS = not significant. * Based on 79 anonymous, 198 completed confidential, and 222 total (intention-to-treat) confidential event reports that had a system issue code. Unknown in this instance means insufficient information to code the specifics of the system issue. Participants 26.79 11.11 <.0001 14.79 .0003 Participant contribution 16.27 8.77 .0077 12.03 NS Setting of event 0.96 1.46 NS 2.26 NS Clinical intent 8.13 7.89 NS 9.77 NS Cause (latent error) 19.62 12.57 .0256 15.04 NS Patient outcome 24.40 21.35 NS 25.06 NS Intervention 29.61 21.64 .0359 28.07 NS Event discoverer 18.66 5.85 <.0001 11.53 .0160 System issue* 44.30 23.23 .0005 25.23 .0015 Any unknown 66.99 49.71 <.0001 55.39 .0057 >1 unknown 39.71 23.39 <.0001 30.58 .0236 Harm Category All Anonymous Reports No. (%) Completed Confidential Reports No. (%) All Confidential Reports No. (%) Clinical harm now 21 (10.05) 38 (11.11) 41 (10.28) Increased risk of clinical harm 21 (10.05) 25 (7.31) 34 (8.52) Nonclinical harm 11 (5.26) 28 (8.19) 28 (7.02) Unstable 22 (10.53) 20 (5.85) 25 (6.27) No known harm 134 (64.11) 231 (67.54) 271 (67.92) Total 209 (100.00) 342 (100.00) 399 (100.01)
Supplemental Appendixes
Files in this Data Supplement:
- Supplemental data: Appendix 1 - PDF file, 1 page, .63 MB
- Supplemental data: Appendix 2 - PDF file, 2 pages, .78 MB
- Supplemental data: Appendix 3 - PDF file, 1 page, .61 MB
The Article in Brief
A system has been developed to collect and manage reports of harm or potential harm to patients in primary care practices. The system offers medical and non-medical personnel the opportunity to submit reports by telephone, paper, or online. Reports can be confidential, in which the reporter's name and phone number are collected, or anonymous. Among 475 participants in 33 medical practices, 66% used the confidential form. The most frequently reported errors involved communication problems and problems with diagnostic tests and medications.




{kind=link}
Jump to section
Related Articles
Cited By...
- Looking Back to Move Forward: Reflections of PBRN Directors
- Ambulatory Medication Safety in Primary Care: A Systematic Review
- Exploration of prescribing error reporting across primary care: a qualitative study
- Implementation and Evaluation of a Laboratory Safety Process Improvement Toolkit
- International recommendations for national patient safety incident reporting systems: an expert Delphi consensus-building process
- Patient safety principles in family medicine residency accreditation standards and curriculum objectives: Implications for primary care
- System hazards in managing laboratory test requests and results in primary care: medical protection database analysis and conceptual model
- Reporting and Using Near-miss Events to Improve Patient Safety in Diverse Primary Care Practices: A Collaborative Approach to Learning from Our Mistakes
- Laboratory Medicine Handoff Gaps Experienced by Primary Care Practices: A Report from the Shared Networks of Collaborative Ambulatory Practices and Partners (SNOCAP)
- A comparison of calls subjected to a malpractice claim versus 'normal calls' within the Swedish Healthcare Direct: a case-control study
- Managing Patient Populations in Primary Care: Points of Leverage
- Emotional Impact of Patient Safety Incidents on Family Physicians and Their Office Staff
- Safety incidents in family medicine
- Central or local incident reporting? A comparative study in Dutch GP out-of-hours services
- Feasibility of centre-based incident reporting in primary healthcare: the SPIEGEL study
- Field Test Results of a New Ambulatory Care Medication Error and Adverse Drug Event Reporting System--MEADERS
- Safety learning system development--incident reporting component for family practice
- What happens between visits? Adverse and potential adverse events among a low-income, urban, ambulatory population with diabetes
- Management of Test Results in Family Medicine Offices
- "Every error counts": a web-based incident reporting and learning system for general practice
- Medication errors reported by US family physicians and their office staff
- Mitigation of patient harm from testing errors in family medicine offices: a report from the American Academy of Family Physicians National Research Network
- Testing process errors and their harms and consequences reported from family medicine practices: a study of the American Academy of Family Physicians National Research Network
- Patient safety events reported in general practice: a taxonomy
- Evaluation of an intervention aimed at improving voluntary incident reporting in hospitals
- Ambulatory care adverse events and preventable adverse events leading to a hospital admission
- Rural Community Members' Perceptions of Harm from Medical Mistakes: A High Plains Research Network (HPRN) Study
- Stopping the error cascade: a report on ameliorators from the ASIPS collaborative
- Harm Resulting from Inappropriate Telephone Triage in Primary Care
- Anatomy of a patient safety event: a pediatric patient safety taxonomy
- Electronic Data Collection Options for Practice-Based Research Networks
- Primary Care Practice-Based Research Networks: Working at the Interface Between Research and Quality Improvement
- Why Isn't It Better?
- In This Issue: Practice Change and Patient Safety