
Article Figures & Data
Figures
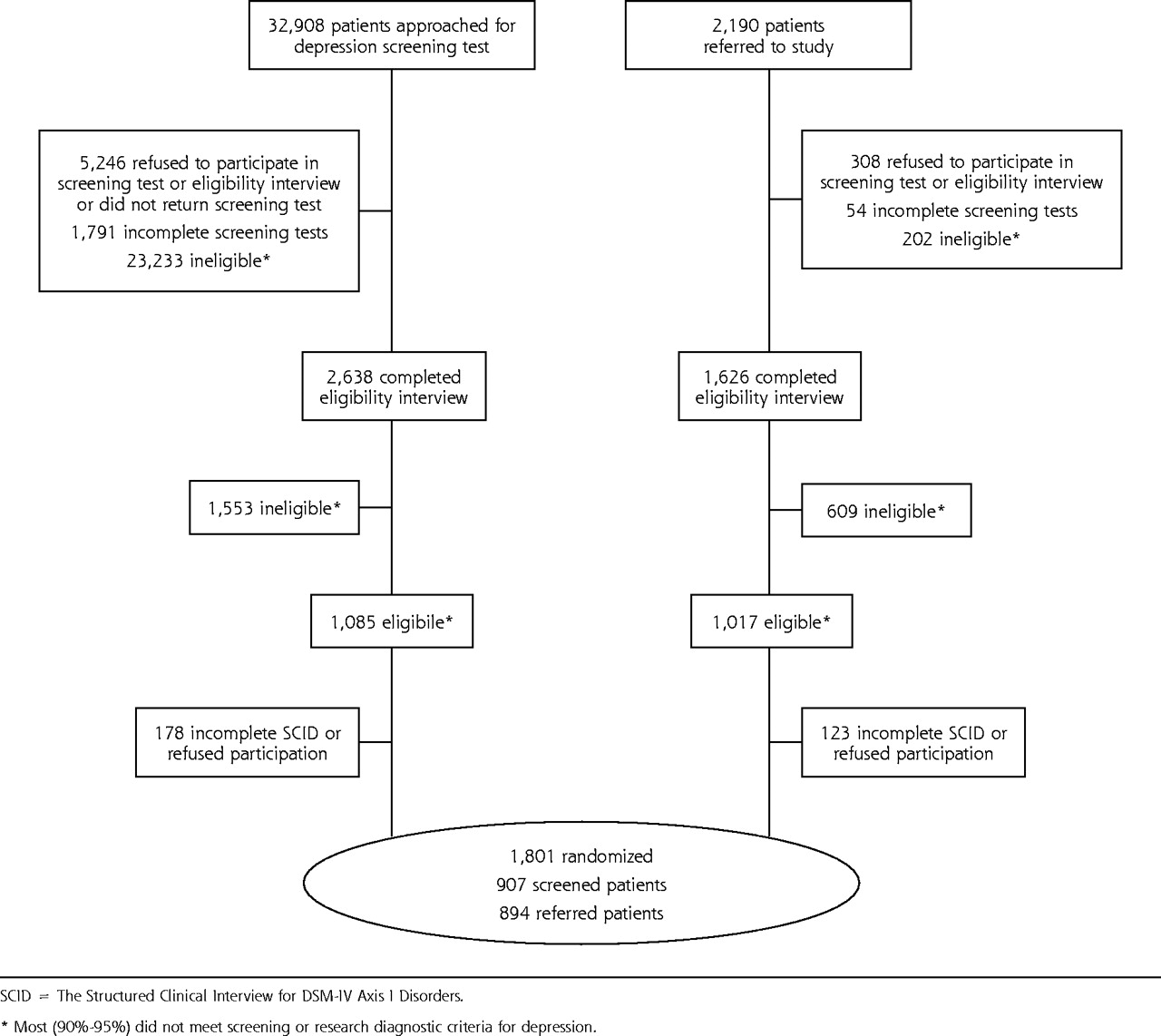
- Figure 1.
IMPACT participant flow. SCID = The Structured Clinical Interview for DSM-IV Axis I Disorders. *Most (90%–95%) did not meet screening or research diagnostic criteria for depression.
Tables
Sample Characteristics Mean SE % PCS-12 = physical component score of the Short Form-12; MCS-12 = mental component score of the Short Form-12); QOL = quality of life; SDI = Sheehan Disability Index. Sociodemographic characteristics Age ≤64 y 23.2 65–69 y 22.5 70v74 y 19.5 5–79 y 20.1 ≥80 y 14.7 Sex, female 64.9 Race or ethnicity White 77.0 African American 12.3 Hispanic 7.6 Other 3.1 Education Less than high school graduate 19.2 High school graduate or general equivalency diploma 22.7 Some college 35.3 College graduate or graduate degree 22.8 Marital status Married or living with partner 46.3 Divorced, separated, or never married 28.9 Widowed 24.8 Psychiatric illnesses Depression severity (0–4), ↑ scores indicate ↑ depression 1.68 0.014 Chronic depression 83.0 Positive screening test for posttraumatic stress disorder 10.6 Positive screening test for panic disorder 21.7 Anxiety-neuroticism, ↑ scores indicate ↑ neuroticism 19.62 0.126 Positive screening test for mild cognitive impairment 35.4 Medical Illnesses Chronic lung disease 23.3 Hypertension 57.9 Diabetes 23.2 Arthritis 55.6 Sensory deficit 55.2 Cancer (excluding skin cancer) 10.9 Neurological disease 8.4 Heart disease 27.6 Chronic pain 56.8 Gastrointestinal disease 20.9 Urinary/prostate disease 38.7 Sum of all chronic diseases (0–11) 3.79 0.046 General health indicators PCS-12 (0–100), ↑ scores indicate better functioning 40.26 0.150 MCS-12 (0–100), ↑ scores indicate better functioning 36.68 0.235 QOL (0–10), ↑ scores indicate better QOL 5.35 0.047 SDI (0–10), ↑ scores indicate greater disability 4.63 0.061 MCS-12 (PValue) QOL (PValue) SDI (PValue) PCS-12 = physicial component of the Short Form-12; MCS-12 = mental component of the Short Form-12; QOL = quality of life. PCS-12 −0.18 (<.001) 0.17 (.397) −0.41 (<.001) MCS-12 0.26 (<.001) −0.24 (<.001) QOL −0.30 (<.001) - Table 3.
Final Models Predicting Physical Functioning (PCS-12), Mental Functioning (MCS-12), Disability (SDI), and Quality of Life (QOL) (N = 1,801)
PCS-12 ↑Scores Indicate Better Physical Functioning MCS-12 ↑Scores Indicate Better Mental Health Functioning SDI ↑Scores Indicate More Disability QOL ↑Scores Indicate Better Quality of Life Characteristics Coeff 95% CL Coeff 95% CL Coeff 95% CL Coeff 95% CL Coeff = coefficient; CL = confidence limits; PTSD = posttraumatic stress disorder. * Indicates standardized regression coefficients with P ≤.001. † Indicates standardized regression coefficients with P <.05 . ‡ Indicates joint test for categorical variables with more than 2 levels, collapsed across levels for presentation in table. § Indicates standardized regression coefficients with P <.01. || Indicates significance of difference of likelihood ratio χ2. Intercept 48.23* 45.29, 51.17 49.85* 46.80, 52.89 1.17† 0.15, 2.19 7.99* 7.18, 8.80 Demographics, P value <.001 <.001 <.001 <.001 Age‡ 0.28 1.04 0.07 0.26 Male 0.86† 0.10, 1.67 −0.17 −0.98, 0.63 0.04 −0.23, 0.32 −0.41* −0.62, −0.20 Education‡ 3.04† 0.38 0.30 2.29 Ethnic group‡ 3.00† 2.59 0.38 1.52 Marital status‡ 0.46 1.09 0.64 3.54† Organization‡ 3.79§ 8.02* 3.65§ 2.71§ Psychological, P value <.016|| <.001|| <.001|| <.001|| Depression severity, ↑scores indicate ↑ severity −0.26* −1.90, −0.63 −3.96* −4.62, −3.29 1.43* 1.21, 1.66 −1.24* −1.44, −1.05 Chronic depression 0.14 −0.73, 1.00 −0.40 −1.32, 0.51 −0.07 −0.37, 0.23 −0.01 −0.24, 0.23 Positive screening test for PTSD 0.06 −0.95, 1.07 −0.04 −1.02, 1.09 0.20 −0.16, 0.56 −0.01 −0.29, 0.26 Positive screening test for panic 0.05 −0.75, 0.84 −0.23 −1.06, 0.60 0.05 −0.23, 0.33 −0.03 −0.25, 0.18 Neuroticism, ↑ scores indicate ↑ neuroticism −0.07† −0.14, − 0.001 −0.01 −0.08, 0.06 0.003 −0.02, 0.03 0.01 −0.01, 0.03 Positive screening test for mild cognitive Impairment −1.13§ −1.82, −0.44 0.14 −0.58, 0.87 0.44§ 0.20, 0.68 0.07 −0.12, 0.25 Medical illness, P value <.001|| .447|| <.001|| .071|| Chronic lung disease −1.63* −2.37, −0.89 0.11 −0.66, 0.89 0.42§ 0.16, 0.69 −0.05 −0.26, 0.15 Hypertension −0.99§ −1.64, −0.34 −0.28 −0.96, 0.39 0.10 −0.13, 0.32 −0.02 −0.20, 0.16 Diabetes −1.56* −2.33, −0.78 −0.27 −1.09, 0.54 0.38§ 0.11, 0.66 −0.04 −0.25, 0.17 Arthritis −2.09* −2.77, −1.41 0.73† 0.02,1.45 0.24 −0.003, 0.48 −0.13 −0.32, 0.06 Sensory deficit −0.43 −1.09, 0.24 0.04 −0.65, 0.74 0.14 −0.10, 0.37 −0.11 −0.29, 0.07 Cancer excluding skin Cancer −0.92 −1.91, 0.08 −0.35 −1.39, 0.69 0.13 −0.23, 0.48 −0.06 −0.33, 0.22 Neurological disease −1.80§ −2.91, −0.69 0.25 −0.93, 1.42 0.86* 0.47, 1.25 −0.21 −0.52, 0.10 Heart disease −0.99§ −1.71, −0.27 −0.61 −1.36, 0.14 0.32† 0.06, 0.57 −0.80§ −1.39, −0.21 Chronic pain −3.08* −3.78, −2.39 −0.01 −0.72, 0.71 0.56* 0.32, 0.81 −0.02 −0.20, 0.17 Gastrointestinal disease −1.08§ −1.86, −0.29 −0.11 −0.92, 0.71 0.12 −0.16, 0.39 −0.03 −0.24, 0.18 Urinary tract or prostate disease −0.48 −1.15, 0.19 0.38 −0.31, 1.08 0.0001 0.24, 0.24 −0.14 −0.32, 0.05 Interactions, P value .021|| <.041|| Depression chronicity X ethnic group‡ 3.26† Depression severity X heart disease 0.35† 0.01, 0.68
The Article in Brief
Treatment of depression may lead to more dramatic improvements in the health of elderly patients than treatment for other chronic illnesses. Researchers found that patients' mental functioning, disability and quality of life are affected more by the severity of a patient's depression than by other chronic medical conditions like diabetes, lung disease, hypertension, cancer, chronic pain and heart disease. Patients with more severe depression experience lower quality of life, lower physical and mental functioning, and more disability. Late-life depression can be treated, and improved recognition and treatment of this condition could significantly improve patients' lives, in spite of other medical illnesses.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Impact of psychiatric comorbidities on health care utilization and cost of care in multiple myeloma
- Effect of comorbidities and medications on frequency of primary care visits among older patients
- Managing Patient Populations in Primary Care: Points of Leverage
- Depression Treatment in Patients With General Medical Conditions: Results From the CO-MED Trial
- Mental Health Conditions are Associated With Increased Health Care Utilization Among Urban Family Medicine Patients
- Barriers to Self-Management and Quality-of-Life Outcomes in Seniors With Multimorbidities
- "Our community of reflective practitioners will continue its quest informed...."
- In This Issue: New Model Finances, Systematic Reviews, Patients and Health Care