
Article Figures & Data
Figures
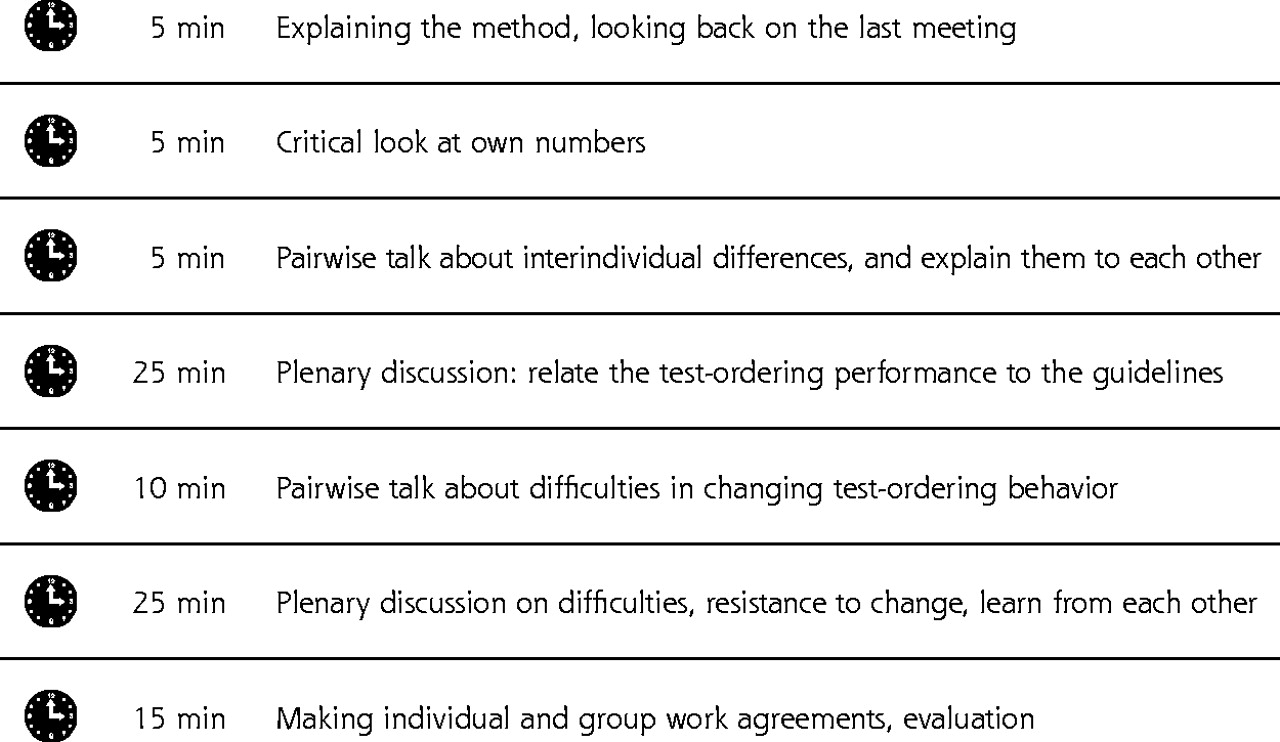
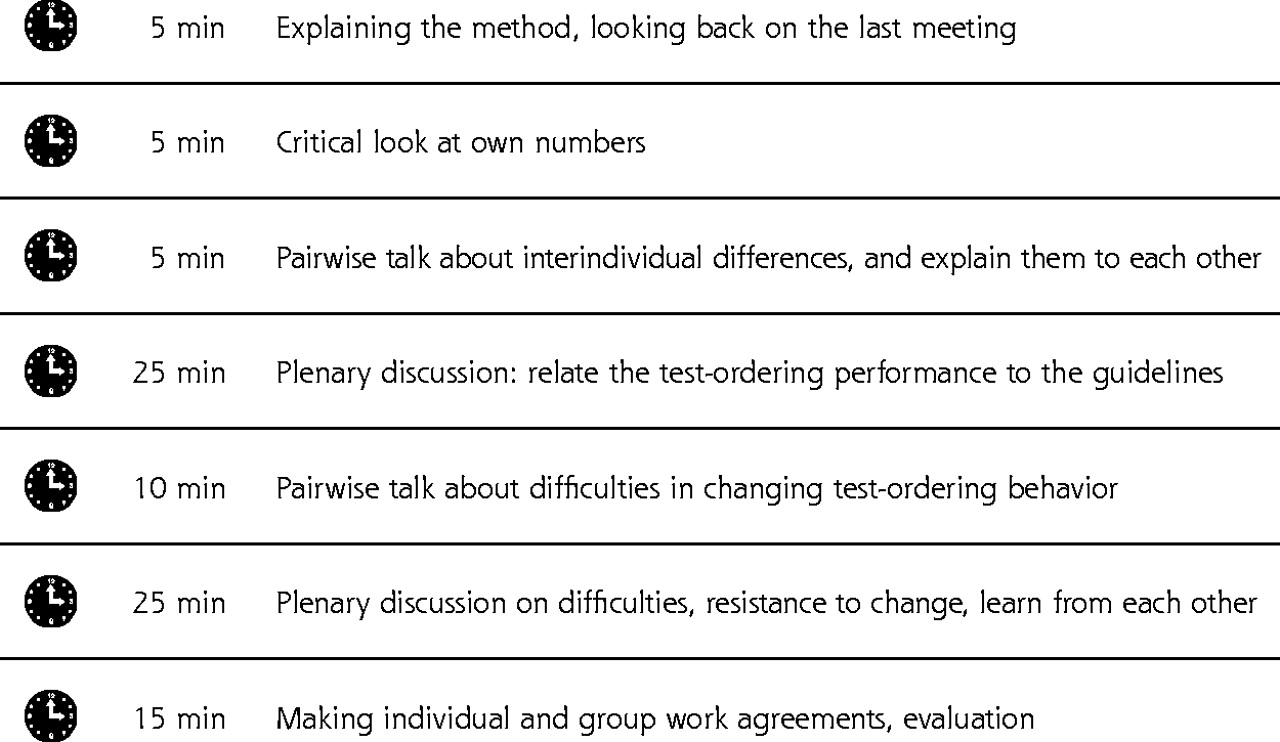
- Figure 1.
Structure of the 90-minute small-group quality improvement meeting.
- Figure 2.
Flow of randomized trial. PCP = primary care physician.
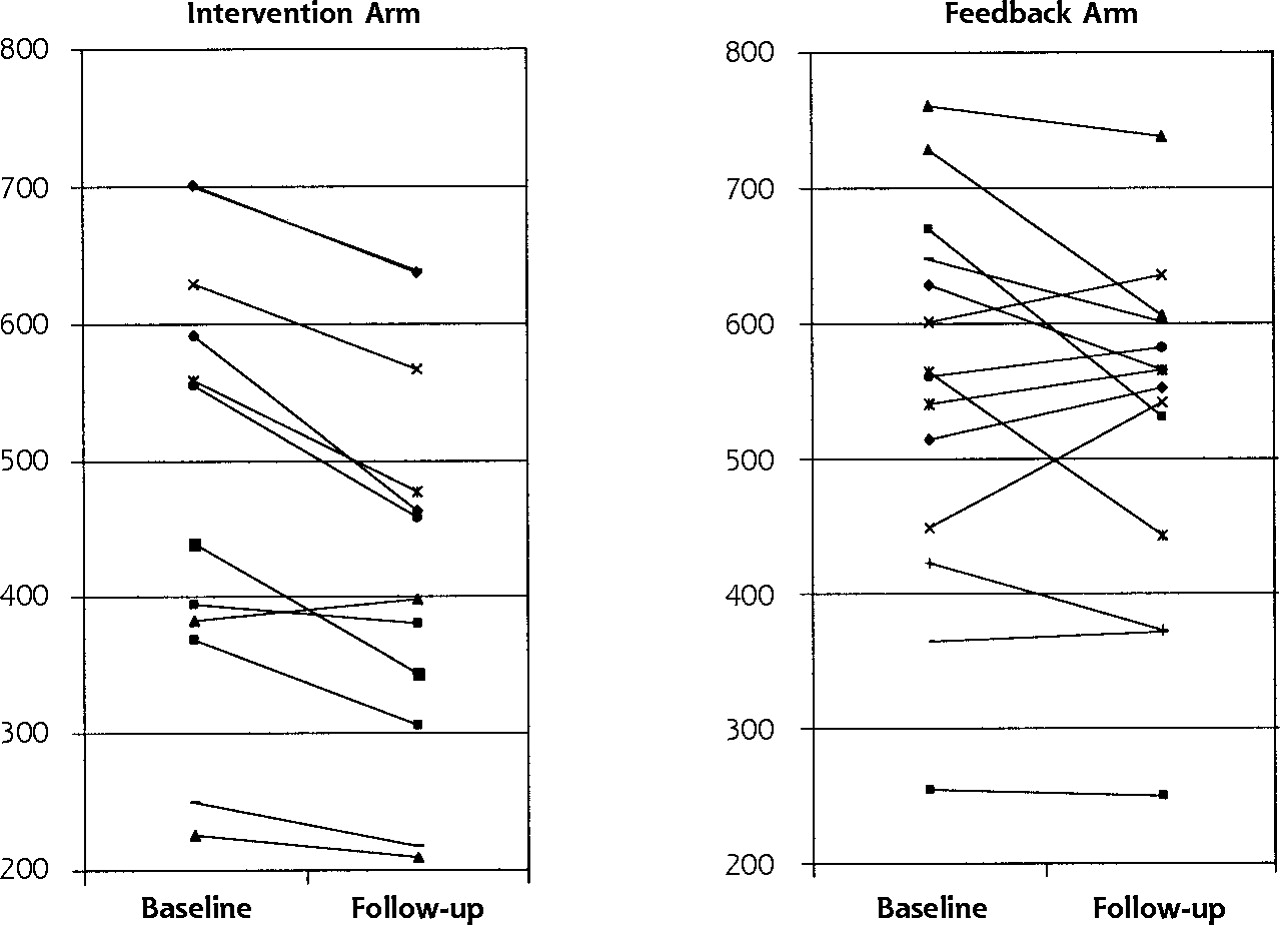
- Figure 3.
Baseline and follow-up measurements in mean total numbers of tests per 6 months at aggregated local practice group level for the 13 intervention and the 14 feedback local practice groups.


Tables
Clinical Problems Tests BUN = blood urea nitrogen; ECG = electrocardiogram; ALT = alanine aminotransferase; AST = aspartate aminotransferase; LDH = lactic dehydrogenase. *Tests that are inappropriate according to national evidence-based guidelines on upper abdominal complaints (see Supplemental Appendix). Cardiovascular conditions Cholesterol, subfractions, potassium, sodium, creatinine, BUN, ECG (exercise) Lower abdominal complaints Prostate-specific antigen, C-reactive protein, ultrasound scan of the kidney, intravenous pyelogram, double-contrast barium enema, sigmoidoscopy Upper abdominal complaints ALT, AST,* LDH*, amylase,* γ-glutamyltrans- ferase, bilirubin,* alkaline phosphatase,* ultrasound scan of hepatobiliary tract Characteristic Intervention Arm Feedback Arm * Total practice population for whom the primary care physician is responsible. † Working time factor, full time = 100% = 5 days; each half-day = 10%, so a physician with a part-time factor of 70% works 7 half-day periods. Number of physicians 85 109 Age, mean (SD), y 46.2 (6.6) 46.2 (6.6) Female, No. (%) 14 (16) 11 (10) Patients per physician, mean No. (SD)* 2,587 (641) 2,444 (416) Patients >65 y, mean % (SD) 15 (6.8) 15 (6.5) Working time factor, % (SD)† 91 (15) 92 (12) Physicians with a solo practice, No. (%) 43 (51) 44 (40) Physicians who use computerized registration system, No. (%) 66 (78) 75 (69) - Table 3.
Effects of Strategy on the Mean (SD) Number of Tests and the Coefficient of Variance, per Primary Care Physician and per 6 Months
Intervention Arm Feedback Arm Study Subjects Baseline Mean (SD) CV* Follow-up Mean (SD) CV* Baseline Mean (SD) CV* Follow-up Mean (SD) CV* β† SE β 95% CI P Note: analysis of covariance adjusted for baseline number of tests and the regions. CV = coefficient of variance; CI = confidence interval. * CV = SD / mean. † β = intervention effect = the total change between baseline and follow-up of mean numbers of tests in Intervention arm less the total change of numbers between baseline and follow-up of mean numbers of tests in the feedback arm. Total number of tests 478 (309) 0.65 422 (235) 0.56 541 (337) 0.62 535 (309) 0.58 −51 17.94 −87 to −16 .005 Cardiovascular conditions 293 (189) 0.65 276 (157) 0.57 322 (214) 0.66 333 (205) 0.62 −25 13.08 −51 to 1 .056 Lower abdominal complaints 20 (20) 1.00 18 (19) 1.06 30 (40) 1.43 30 (27) 0.90 −6 2.18 −10 to −2 .008 Upper abdominal complaints 165 (125) 0.76 128 (82) 0.64 188 (143) 0.76 171(117) 0.68 −24 7.98 −40 to −8 .003 Inappropriate upper abdominal tests 55 (60) 1.09 39 (32) 0.82 60 (63) 1.05 56 (54) 0.96 −13 4.1 −22 to −5.2 .002
Supplemental Appendix and Figure
Supplemental Appendix. Upper Abdominal Complaints; Supplemental figure. An Example of a Feedback Report.
Files in this Data Supplement:
- Supplemental data: Appendix - PDF file, 1 page, 46 KB
- Supplemental data: Figure - PDF file, 1 page, 41 KB
The Article in Brief
Physicians who participate in specially designed meetings with their peers order fewer diagnostic tests than physicians who receive only written reports about test ordering. The small-group meetings were held among primary care physicians in the Netherlands to discuss tests they ordered for patients with cardiovascular conditions (such as high cholesterol levels) and upper and lower abdominal complaints, and to review national guidelines on those topics. Meeting participants ordered fewer tests than physicians who received only written feedback about their test-ordering behavior. This strategy may be an effective way to reduce unnecessary test ordering and is being implemented throughout the Netherlands.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Improving ondansetron use and oral rehydration instructions for pediatric acute gastroenteritis
- Strategies to reduce the use of low-value medical tests in primary care: a systematic review
- What motivates general practitioners to change practice behaviour? A qualitative study of audit and feedback group sessions in Dutch general practice
- Quality circles for quality improvement in primary health care: their effectiveness, gaps of knowledge, origins and significance - a scoping review
- Explaining variations in test ordering in primary care: protocol for a realist review
- Temporal growth and geographic variation in the use of laboratory tests by NHS general practices: using routine data to identify research priorities
- Canadian Quality Circle pilot project in osteoporosis: Rationale, methods, and feasibility
- "Our community of reflective practitioners will continue its quest informed...."
- In This Issue: New Model Finances, Systematic Reviews, Patients and Health Care