
Article Figures & Data
Figures
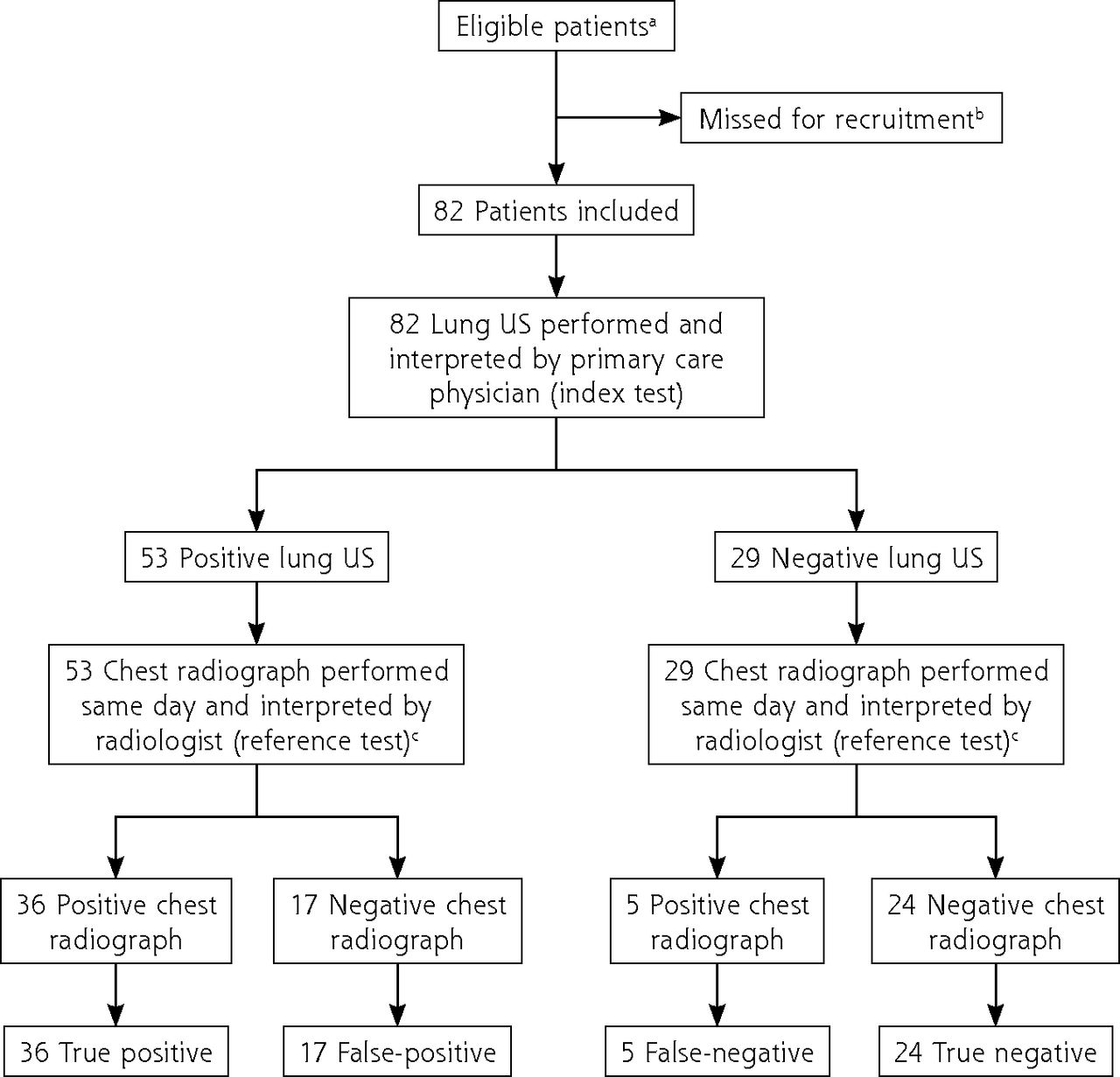
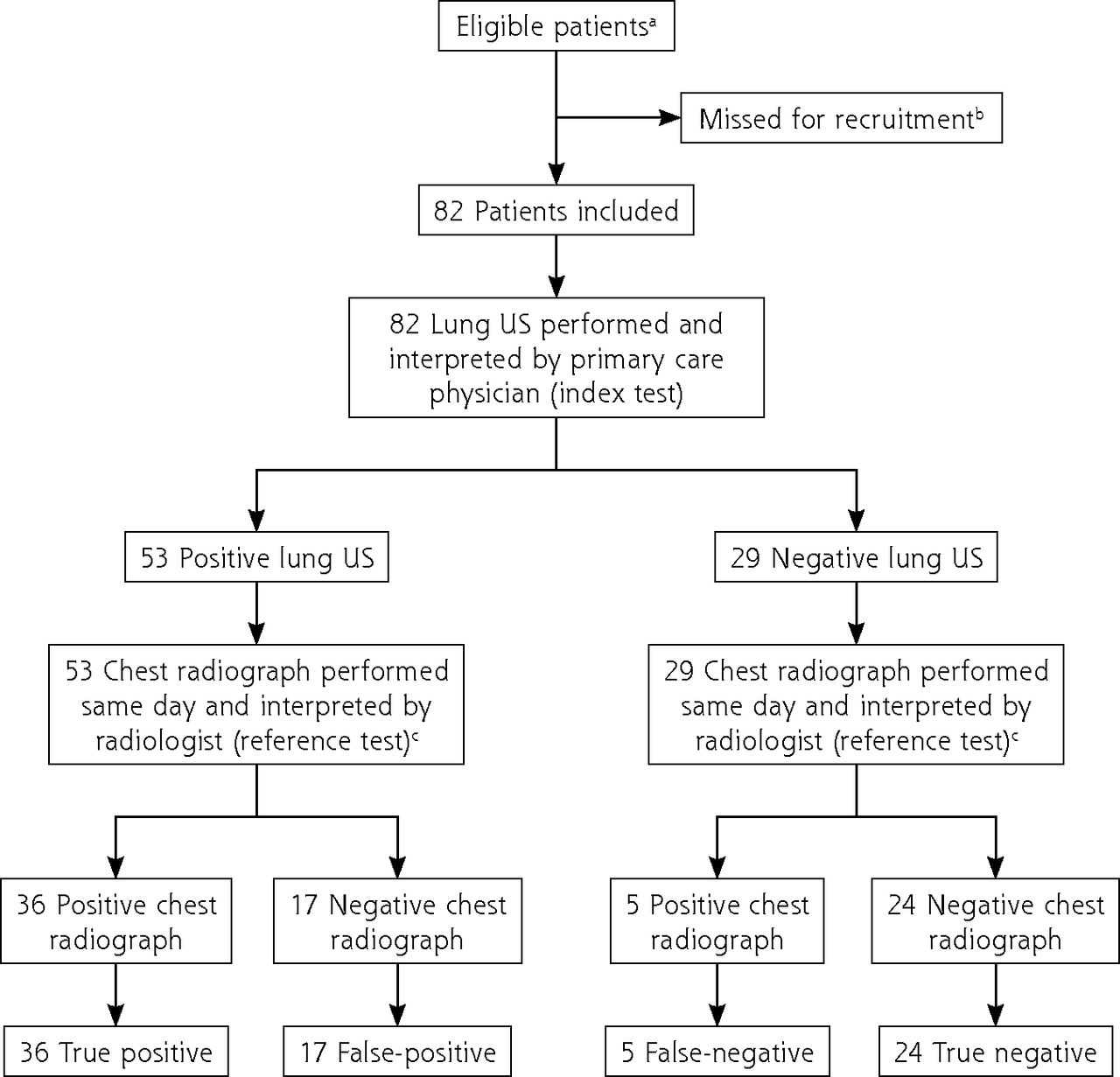
- Figure 1.
STARD diagram showing flow of patients in the study.
STARD = Standards for Reporting of Diagnostic Accuracy; US = ultrasound.
a Defined by the study’s inclusion and exclusion criteria (Table 1). All had a history and physical examination performed by the primary care physician.
b Study protocol did not require recording of number of potentially eligible patients who were missed (due to patient declining to participate or insufficient time to explain the study).
c All chest radiographs were performed the same day at the referral hospital. For this study, the chest radiograph result used for analyses was the one in the report from the hospital’s radiology department (interpretation of the radiograph by the primary care physician was not included).
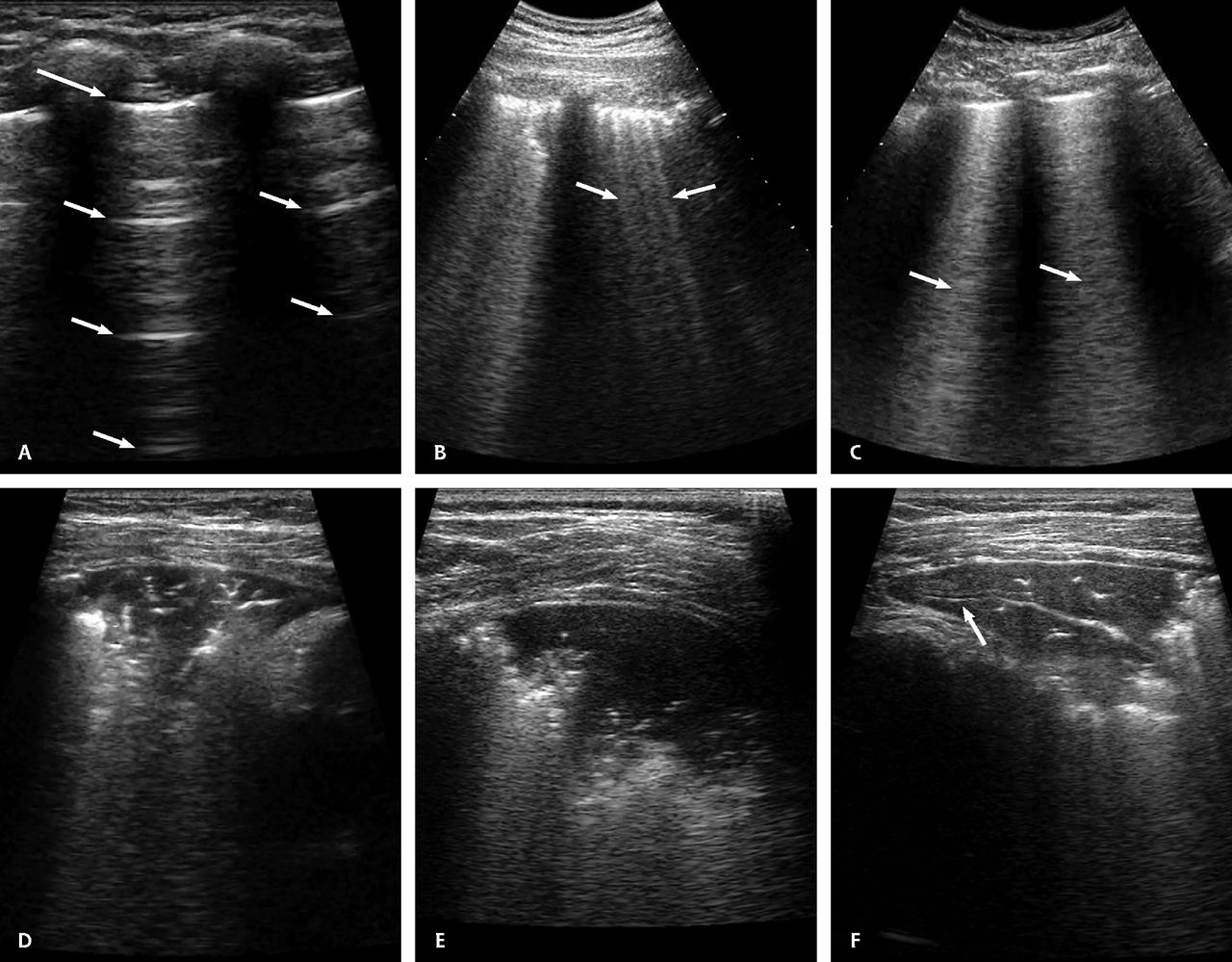
- Figure 2.
Representative images of various lung ultrasound patterns considered in this study.
Panel A: Normal lung ultrasound showing the A-lines pattern, with a well-defined pleural line (long arrow) and parallel A-lines (short arrows). Panels B and C: Pathological B-lines patterns showing multiple and separated B-lines (arrows in panel B) and coalescent B-lines (arrows in panel C). Panels D, E, and F: Images of consolidations, evident as subpleural hypoechogenic areas with an echogenic air bronchogram. Panel F also shows a hypoechogenic fluid bronchogram (arrow).
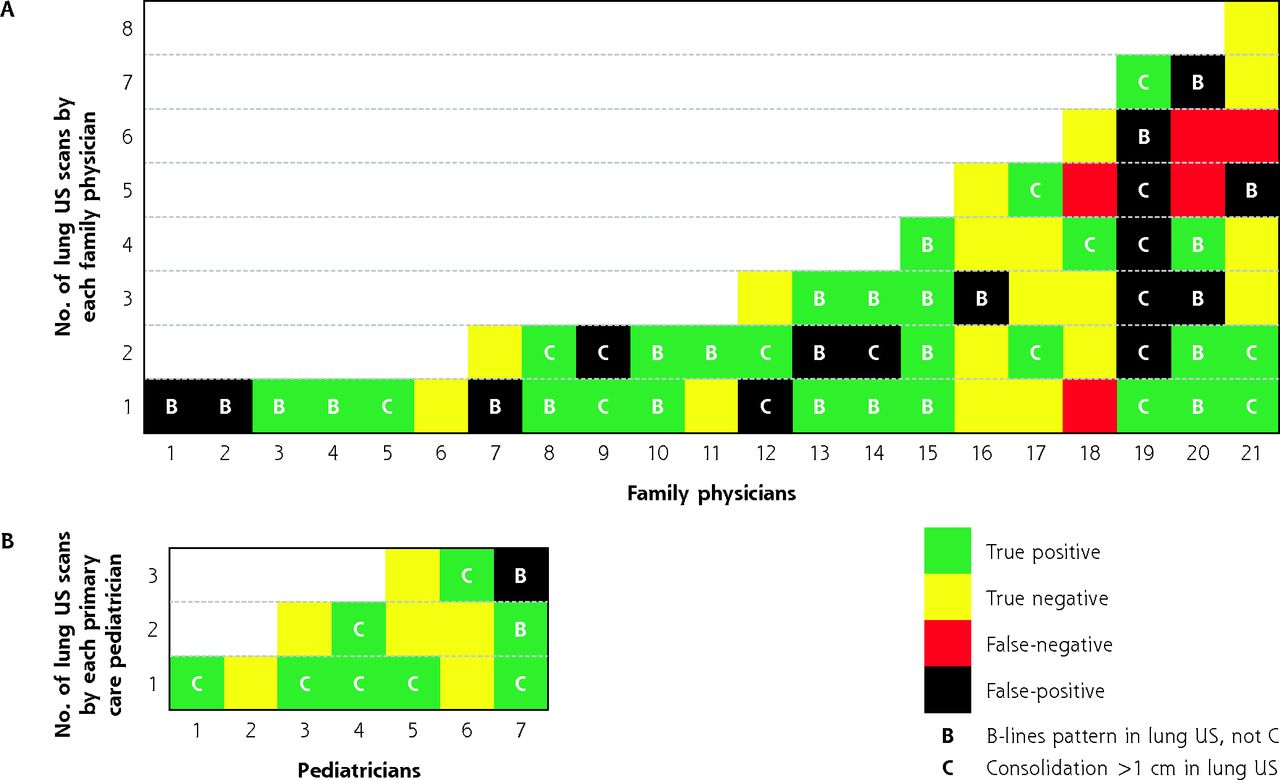
- Figure 3.
Concordance of lung US and chest radiography results for individual patients, according to type of primary care physician performing US.
US = ultrasound.
Notes: Figure shows result of lung US performed by primary care physicians (index test) compared with result of chest radiograph as interpreted by a radiologist (reference test). Each block represents a lung US scan and is color coded to show the test result. Blocks are arranged vertically in chronological order, with the first scan at the bottom. Panel A: Adult patients (aged >14 years) with lung US performed by family physicians. Almost one-half of all false results were accounted for by physicians 19 and 20, who had among the most US training and experience. Panel B: Pediatric patients (aged 5-14 years) with lung US performed by primary care pediatricians. Note that despite the initial clinical suspicion of pneumonia, patients with true-negative results (40% of pediatric results) would not have received antibiotics according to the algorithm shown in Figure 4.
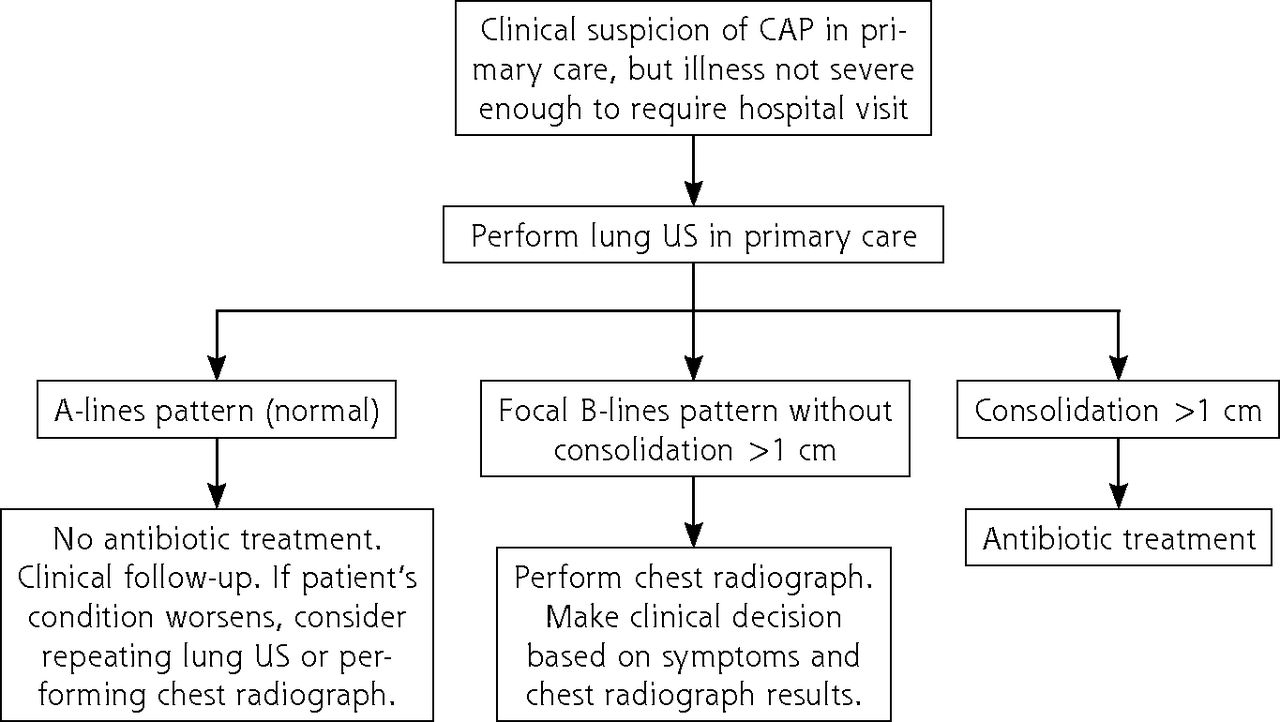
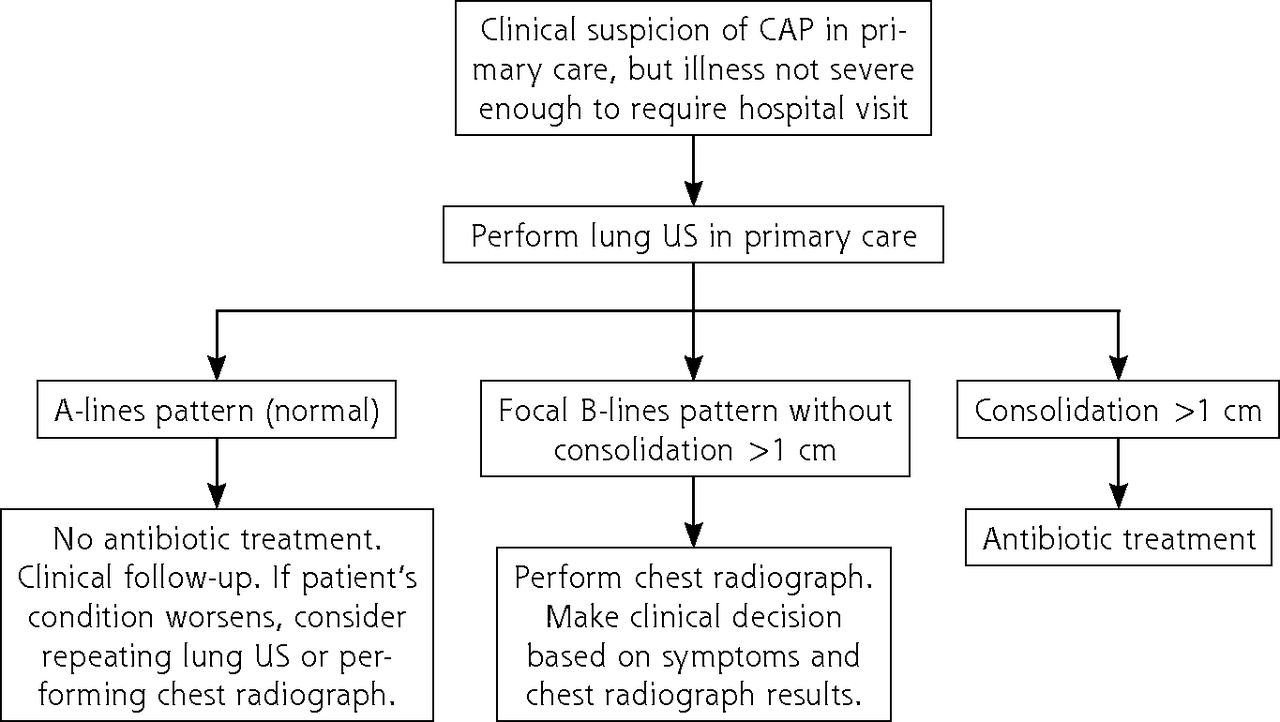
- Figure 4.
Proposed clinical algorithm to guide decision making when using lung US in patients with suspected CAP in primary care.
CAP = community-acquired pneumonia; US = ultrasound.

Tables
Inclusion criteriaa Aged 5 years or older with clinically suspected CAP and either of the following features: Feverb characterized by 1 of following: >72 hours of fever and cough without any improvement Fever >72 hours with purulent sputum Fever with ≥1 of following: pleuritic pain; focal or asymmetric auscultation of crackles or hypoventilation; dyspnea (subjective); signs of breathing distress such as tachypnea, retractions, or nasal flaring (objective); SpO2 <95%; hemoptysis Isolated fever without focus lasting >4 days Reappearance or worsening of fever after clinical improvement of a respiratory condition No fever, but presence of 1 of following: Cough and purulent sputum lasting >4 days Cough with ≥1 of following: pleuritic pain; focal or asymmetric auscultation of crackles or hypoventilation; dyspnea (subjective); signs of breathing distress such tachypnea, retractions, or nasal flaring (objective); SpO2 <95% Cough lasting >4 weeks, even as an isolated symptom Dyspnea in patients aged >75 years Exclusion criteriac Hospital admission within past 30 days (ie, possible nosocomial pneumonia instead of CAP) Pneumonia already diagnosed during current illness by an imaging test Receipt of antibiotics for current illness Previous diagnosis of chronic obstructive pulmonary disease Previous diagnosis of asthma, or suspicion of asthma attack or bronchial spasm in current illness Children with previous diagnosis of recurrent wheezing related to viral infections in whom current illness suggests same diagnosis Lung or pleural cancer Previous pleurodesis Previous thoracic surgery Other chronic lung diseases (eg, pulmonary fibrosis) Terminal disease (life expectancy <6 months) Hemodynamic instability Declined lung ultrasound and/or chest radiograph Inability to go to the hospital for chest radiograph the same day Declined to sign informed consent CAP = community-acquired pneumonia; SpO2 = peripheral oxygen saturation.
↵a Inclusion criteria were selected to avoid inclusion solely for clinical suspicion of pneumonia, a term that has greater potential subjectivity in its interpretation.
↵b Temperature ≥38°C not explained by extrathoracic symptoms.
↵c Exclusion criteria were primarily selected to avoid clinical conditions that might confound lung ultrasound findings.
Characteristic Value Patients Sex, female, No. (%) 42 (51.2) Age, median (IQR), y 47 (22-60) Age by age-groupa Pediatric, mean (SD), y 8.9 (2.3) Adult, mean (SD), y 51.3 (16.8) Temperature ≥38°C, No. (%) 58 (70.7) Signs and symptoms, No. (%) Cough 80 (97.6) Expectoration 58 (70.7) Hemoptysis 3 (3.7) Pleuritic pain 22 (26.8) Dyspnea (subjective) 27 (32.9) Signs of respiratory distress 9 (11.0) Auscultatory findings, No. (%)b Normal 16 (19.5) Crackles 49 (59.8) Hypoventilation 16 (19.5) Rhonchi 7 (8.5) Wheezing 6 (7.3) SpO2, median (IQR), % 97 (95-98) Primary care physicians Specialty, No. (%) Family physician 21 (75) Pediatrician 7 (25) Previous accredited US training, median (IQR), h 85 (49-244) Previous US experience, median (IQR), y 4.5 (2-6.75) Number of patients recruited per physician, median (IQR) [range] 2 (1-3.8) [1-8] Imaging Test and Result Patients, No. (%) Lung USa Negative (A-lines pattern) 29 (35.4) Positive 53 (64.6) ≥1 consolidation measuring >1 cmb 25 (30.5) B-lines pattern without any consolidation measuring >1 cm 28 (34.1) Chest radiography Negative 41 (50.0) Normal 36 (43.9) Peribronchial thickening 5 (6.1) Positive 41 (50.0) Alveolar consolidation 35 (42.7) Interstitial pneumonia 4 (4.9) Both alveolar and interstitial findings 2 (2.4) - Table 4.
Diagnostic Performance of Lung US Compared With Chest Radiography, in Full Cohort and in Subgroups
Chest Radiography Result Lung US Result Positive, No. (%) Negative, No. (%) Total, No. (%) OR (95% CI) [P Value] Diagnostic Performance of Lung US, Value (95% CI) Full cohort Positive lung US 36 (87.8) 17 (41.5) 53 (64.6) 10.2 (3.3-31.2) Sensitivity: 0.88 (0.75-0.95); specificity: 0.59 (0.43-0.72); PPV: 0.68 (0.55-0.79); NPV: 0.83 (0.66-0.92); positive LR: 2.12 (1.45-3.10); negative LR: 0.21 (0.09-0.49) Negative lung US 5 (12.2) 24 (58.5) 29 (35.4) [<.001] Total 41 (100) 41 (100) 82 (100) Patients’ age group
PediatricPositive lung US 8 (100) 1 (14.3) 9 (60.0) 96a (2.7-3,362) Sensitivity: 1 (0.68-1); specificity: 0.86 (0.49-0.97); PPV: 0.89 (0.57-0.98); NPV: 1 (0.61-1); positive LR: 6.99 (1.14-42.97); negative LR: not calculable Negative lung US 0 (0) 6 (85.7) 6 (40.0) [.001] Total 8 (100) 7 (100) 15 (100) Adult Positive lung US 28 (84.8) 16 (47.1) 44 (65.7) 6.3 (2.0-20.2) Sensitivity: 0.85 (0.69-0.93); specificity: 0.53 (0.37-0.69); PPV: 0.64 (0.49-0.76); NPV: 0.78 (0.58-0.90); positive LR: 1.80 (1.23-2.65); negative LR: 0.29 (0.12-0.68) Negative lung US 5 (15.2) 18 (52.9) 23 (34.3) [.001] Total 33 (100) 34 (100) 67 (100) Physicians’ accredited US training time <100 hours Positive lung US 18 (90.0) 6 (35.3) 24 (64.9) 16.5 (2.8-96.7) Sensitivity: 0.90 (0.70-0.97); specificity: 0.65 (0.41-0.83); PPV: 0.75 (0.55-0.88); NPV: 0.85 (0.58-0.96); positive LR: 2.55 (1.32-4.93); negative LR: 0.16 (0.04-0.60) Negative lung US 2 (10.0) 11 (64.7) 13 (35.1) [.001] Total 20 (100) 17 (100) 37 (100) ≥100 hours Positive lung US 18 (85.7) 11 (45.8) 29 (64.4) 7.1 (1.6-30.6) Sensitivity: 0.86 (0.65-0.95); specificity: 0.54 (0.35-0.72); PPV: 0.32 (0.44-0.77); NPV: 0.81 (0.57-0.93); positive LR: 1.87 (1.17-2.99); negative LR: 0.26 (0.09-0.80) Negative lung US 3 (14.3) 13 (54.2) 16 (35.6) [.005] Total 21 (100) 24 (100) 45 (100) Physicians’ experience using US <3 years Positive lung US 7 (100) 3 (37.5) 10 (66.7) 23.3a (1.0-576.1) Sensitivity: 1 (0.65-1); specificity: 0.63 (0.31-0.86); PPV: 0.70 (0.40-0.89); NPV: 1 (0.57-1); positive LR: 2.67 (1.09-6.52); negative LR: not calculable Negative lung US 0 (0) 5 (62.5) 5 (33.3) [.03] Total 7 (100) 8 (100) 15 (100) 3-6 years Positive lung US 20 (83.3) 5 (35.7) 25 (65.8) 9 (1.9-41.7) Sensitivity: 0.83 (0.64-0.93); specificity: 0.64 (0.39-0.84); PPV: 0.80 (0.61-0.91); NPV: 0.69 (0.42-0.87); positive LR: 2.33 (1.13-4.82); negative LR: 0.26 (0.10-0.69) Negative lung US 4 (16.7) 9 (64.3) 13 (34.2) [.005] Total 24 (100) 14 (100) 38 (100) >6 years Positive lung US 9 (90) 9 (47.4) 18 (62.1) 10 (1.1-95.2) Sensitivity: 0.90 (0.60-0.98); specificity: 0.53 (0.32-0.73); PPV: 0.50 (0.29-0.71); NPV: 0.91 (0.62-0.98); positive LR: 1.90 (1.13-3.19); negative LR: 0.19 (0.03-1.28) Negative lung US 1 (10) 10 (52.6) 11 (37.9) [.04] Total 10 (100) 19 (100) 29 (100) LR = likelihood ratio; NPV = negative predictive value; OR = odds ratio; PPV = positive predictive value; US = ultrasound.
↵a In the 2 cases where a cell contained a 0 value, the OR was calculated by imputing 0.5 for that cell.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.